Article Text

Abstract
Objectives To identify and assess the social support interventions provided to caregivers of older adults with dementia. By synthesising the findings, it seeks to provide insights into effective strategies that can enhance caregivers’ support.
Design A scoping review.
Data sources The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews was strictly followed in this study. Searches were systematically conducted across five databases (PubMed, Web of Science, Embase, Cochrane Library, CINAHL) from their inception up to February 2025.
Eligibility criteria for selecting studies We included original intervention studies published in English that examined social support interventions for caregivers of older adults with dementia, focusing on outcomes reporting social support.
Data extraction and synthesis Data extraction was conducted using a standardised Microsoft Excel chart based on Arksey and O’Malley’s method. Two reviewers independently collected information on study characteristics (authors, country, publication year, design, sample size, assessment tools, interventions and outcomes). Disagreements were resolved by a third independent reviewer.
Results A total of 31 studies were selected for this review, revealing six distinct categories of social support interventions for caregivers of older adults with dementia. These categories included peer support (n=7), counselling group intervention (n=2), health education (n=2), mindfulness-based stress reduction intervention (n=1), individual therapy (n=1) and multicomponent interventions (n=18). The findings indicate that these interventions significantly enhanced the social support available to caregivers, leading to positive outcomes such as reduced caregivers burden, anxiety, depression and improved coping skills.
Conclusion This review underscores the variety of interventions designed to enhance social support for caregivers of older adults with dementia. The findings provide valuable insights for caregivers, administrators and other stakeholders, emphasising the critical need to adopt and promote effective social support strategies for this population.
Trial registration details A review protocol was registered on the OSF(Open Science Framework) registries, with the following registration doi: https://doi.org/10.17605/OSF.IO/D9C53.
- Dementia
- Caregivers
- Social Support
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This scoping review performed a comprehensive search strategy to identify articles that focused on interventions specifically designed to support caregivers of older adults with dementia.
We conducted a quality assessment on the included randomised controlled trials; however, this assessment did not extend to other types of studies included in the review.
This study was limited to articles published in English and did not include grey literature or conference literature.
Background
According to the WHO 2023 report, dementia affects over 55 million people globally, with projections indicating a rise to 139 million by 2050, largely driven by global population ageing.1 Dementia is anticipated to become the seventh leading cause of mortality worldwide.2 Caring for older adults with dementia presents significant challenges due to the progressive cognitive decline and neuropsychiatric manifestations associated with the condition, including behavioural and psychological symptoms of dementia.3
Caregivers of older adults with dementia can be categorised as formal or informal, with informal caregivers—typically family members, friends or relatives—playing a crucial role in supporting older adults suffering from advanced, terminal illnesses.4 These informal caregivers are unpaid5 and often dedicate substantial time, with approximately 16 million individuals providing over 18.6 billion hours of care annually.6 The caregiving role is time-intensive, demanding substantial personal and temporal commitments. The progressive nature of dementia exacerbates the challenges faced by family caregivers, particularly in managing neuropsychiatric symptoms and functional decline.7 Many caregivers experience feelings of isolation and helplessness due to a lack of emotional, informational and practical support.8 Research indicates that family caregivers of individuals with dementia experience elevated caregiver burden, depressive symptoms and reduced quality of life compared with those caring for patients with non-dementia chronic conditions.9 In contrast, formal caregivers refer to professionally trained nursing staff, such as nurses, nursing assistants and rehabilitation therapists, who provide compensated professional nursing services to individuals with dementia and usually receive compensation.10 Given the critical role caregivers play in dementia care, understanding their needs and experiences is essential for developing effective social support interventions. However, studies have shown that these needs are often overlooked in the service development process.11 Interventions developed in collaboration with caregivers have demonstrated more favourable outcomes in reducing caregiver burden and improving mental health, underscoring the importance of involving caregivers in the design of support programmes.12
Social support encompasses the emotional, informational, material and behavioural assistance individuals receive within their social relationships, which can alleviate stress, enhance psychological resilience and promote individual mental health.13 It reflects both subjective or objective effects of various social relationships embedded in social networks,14 and is derived from multiple societal aspects, including emotional, specific and informational support.15 This concept involves the exchange of emotional connections—such as affection, love, admiration and respect—alongside affirmation, which includes agreement and acknowledgement of the appropriate action or perspectives, as well as assistance in the form of resources, financial support, information, guidance or favours.16 Social support represents the consistent engagement between individuals and groups sharing common values, serving as a source of mental motivation, feedback, assistance and material aid.17 Theoretically, the social support framework can be viewed as a provider-centric model, in which one or more individuals or network participants offer valuable assistance to the beneficiary.18 By providing a defence against stress, social support fosters psychological resilience19 and coping strategies in individuals.20 Additionally, it moderates the relationship between self-efficacy and mental health,21 highlighting its critical role in promoting well-being.
As an external resource, social support contributes to enhancing the physical well-being of caregivers.19 20 The substantial stress associated with caregiving responsibilities can exacerbate negative emotions such as anxiety and depression, adversely impacting both mental and physical health,22 which may, in turn, diminish the quality of care provided. Additionally, the demands of the caregiving role can lead to increased feelings of loneliness.23 While social support is crucial for overall well-being, a study revealed that stigma often leads caregivers to be reluctant to seek out such support, resulting in isolation that further intensifies their caregiving burden.24 These factors can severely affect the caregivers’ physical and mental health, increasing their vulnerability to heart-related diseases and other health issues.25 Therefore, addressing the barriers to social support is essential for improving the well-being of caregivers and the quality of care they provide.
Targeted social support interventions are essential to caregivers of older adults with dementia, a population that frequently relies on informal support networks to alleviate caregiving burden and maintain psychosocial resilience.26 Interventions such as psychological training, therapeutic treatments and self-care programmes have demonstrated efficacy in reducing stress associated with emotional and behavioural issues.27 In England, respite care is often the preferred option for those caring for individuals with advanced dementia.28 Since the 1990s, computer networks have played a pivotal role in delivering these interventions.29 Emerging evidence indicates that technology-based interventions, such as digital communication platforms, can improve social connectedness and reduce feelings of loneliness among older adults, particularly those experiencing social isolation.30 As social support improves, individuals find it easier to deal with life’s challenges. Another study has shown that the levels of satisfaction with social support significantly influence the attitudes of Korean American caregivers towards individuals with dementia.31 However, despite the increasing diversity of social support interventions for dementia caregivers, the fragmented nature of existing evidence—characterised by methodological heterogeneity and inconsistent outcome reporting—hinders a robust synthesis of their effectiveness and implementation fidelity.
This scoping review aimed to synthesise the existing research on social support interventions specifically targeting caregivers of older adults with dementia. It seeks to achieve three main objectives: (1) to summarise the various types of research evidence available, including studies focused on social support and evaluation of the research populations; (2) to provide an overview of the specific content of interventions for social support and their associated outcomes as measured by various metrics; and (3) to assess the effectiveness of documented social support interventions for caregivers. By integrating these elements, this review aims to clarify the current landscape of social support research in this critical area and identify potential gaps for future investigation.
Methods
Research questions
The review addressed the following research questions: (1) What types of interventions are designed to improve the social support of caregivers of older adults with dementia? (2) What assessment tools are used to evaluate social support, and what specific outcomes are measured? (3) What effects are observed following the implementation of these interventions for caregivers of older adults with dementia?
Search strategy
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension for Scoping Reviews checklist and adhered to Arksey and O’Malley’s methodological framework.32 The framework includes five key steps: identifying the research question, searching for relevant studies, selecting studies, charting the data and collecting, summarising and reporting the results. To map the existing research in this field, we conducted comprehensive searches across five major databases: PubMed, Web of Science, Embase, Cochrane Library and CINAHL, with the aim of identifying studies that met the inclusion criteria. A preliminary search was performed to locate relevant literature on the topic (see online supplemental search strategy). The search strategy was collaboratively developed by team members, and the literature retrieval was carried out independently by two master’s students with medical experience. Our search used the keywords ‘dementia caregivers’, ‘social support’ and ‘intervention’ to ensure a thorough exploration of pertinent evidence, covering the period from the inception of the databases up to February 2025.
Supplemental material
Inclusion criteria
This scoping review focused on research examining social support interventions specifically designed for caregivers of older individuals with dementia. Eligible studies included those that targeted these caregivers and reported outcomes related to social support. Only original intervention studies with full texts were considered for inclusion. Additionally, the review was limited to literature published in English to ensure the synthesis of globally accessible evidence aligned with the review’s objective.
Exclusion criteria
Studies were excluded if the full text was unavailable, vital information was absent, an explicit methodology was absent, or the publication language was not English.
Types of sources
In alignment with the review questions, this scoping review included a variety of intervention studies, specifically randomised controlled trials (RCTs), non-randomised controlled trials (NRCTs) and mixed-methods studies.
Study selection
The study selection process involved importing citations into EndNote X9 citation management software, followed by the removal of duplicates. Prior to screening, all reviewers received standardised training to ensure consistency in the evaluation process. Two researchers independently conducted an initial screening of eligibility based on the titles and abstracts, subsequently reviewing the full texts for further assessment against the predefined inclusion and exclusion criteria. The rationale for excluding any studies was meticulously documented. Any discrepancies among the authors were resolved through consultation with an additional author. The search results are illustrated in the PRISMA flow diagram (figure 1).

Preferred Reporting Items for Scoping Reviews and Meta-Analyses flow diagram.
Data extraction
A standardised extraction data chart was developed in Microsoft Excel, drawing on Arksey and O’Malley’s data extraction form,32 following consultation among all authors to ensure comprehensive data collection from the included studies. Two investigators independently gathered relevant information from the eligible records. The Excel table was designed to facilitate the extraction of key details, including authors’ name, country of origin, publication year, study design, sample characteristics, sample size, assessment tools, intervention strategies (such as types, frequency, tools and outcomes) and the main findings of each study. Any disagreements in the data extraction process were resolved by an additional independent reviewer, ensuring the accuracy and reliability of the collected data.
Patient and public involvement
Patients and the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
Overview of findings
The initial search identified 3127 relevant citations (see figure 1). After deduplication, 1871 articles were selected for inclusion. A review of titles and abstracts led to the identification of 183 studies for full-text assessment. Of these, 143 articles were excluded for various reasons: 36 were designed with protocols, 24 had participants who did not meet the eligibility criteria, 52 focused on outcomes that did not include social support, 25 were not published in English and 8 had missing full texts. Ultimately, 31 studies were incorporated in this scoping review. Efforts were made to contact the author of the article for which the full text cannot be obtained; however, no responses were received.
Study characteristics
The 31 studies were published between 1988 and 2025. Among these, 16 were RCTs,33–48 8 were NRCTs,49–56 and 7 were mixed methods studies.57–63 The majority of the studies were conducted in the USA (n=19), followed by Europe (n=11), Oceania (n=1) and Asia (n=2). Table 1 presents an overview of the of the fundamental details of the included studies. In terms of intervention settings, 2 studies were conducted in long-term care institutions,23 64 10 in community settings33 34 48 49 52 53 55 57 58 61 and 19 in the older adults’ homes.32–41 43 44 47 49 52 53 55 56 The total sample size of caregivers across the studies was 4629, with individual study sizes ranging from 12 to 494 participants and a median of 85 cases. The majority of studies targeted family caregivers of older adults with dementia, with representation across diverse cultural contexts. Notably, three studies specifically evaluated social support interventions tailored for African American caregivers, highlighting gaps in evidence for underserved populations.57 59 60 Additionally, one study focused on caregivers of Turkish and Moroccan backgrounds living in the Netherlands,46 while another investigated ways to enhance social support among Chinese Canadian caregivers.63 Although interventions were frequently delivered in community-based or clinical settings, the majority targeted family caregivers of individuals with dementia broadly, with only one study explicitly focusing on spousal caregivers through dyadic, kinship-specific support frameworks.41
Characteristics of included studies
Quality appraisal
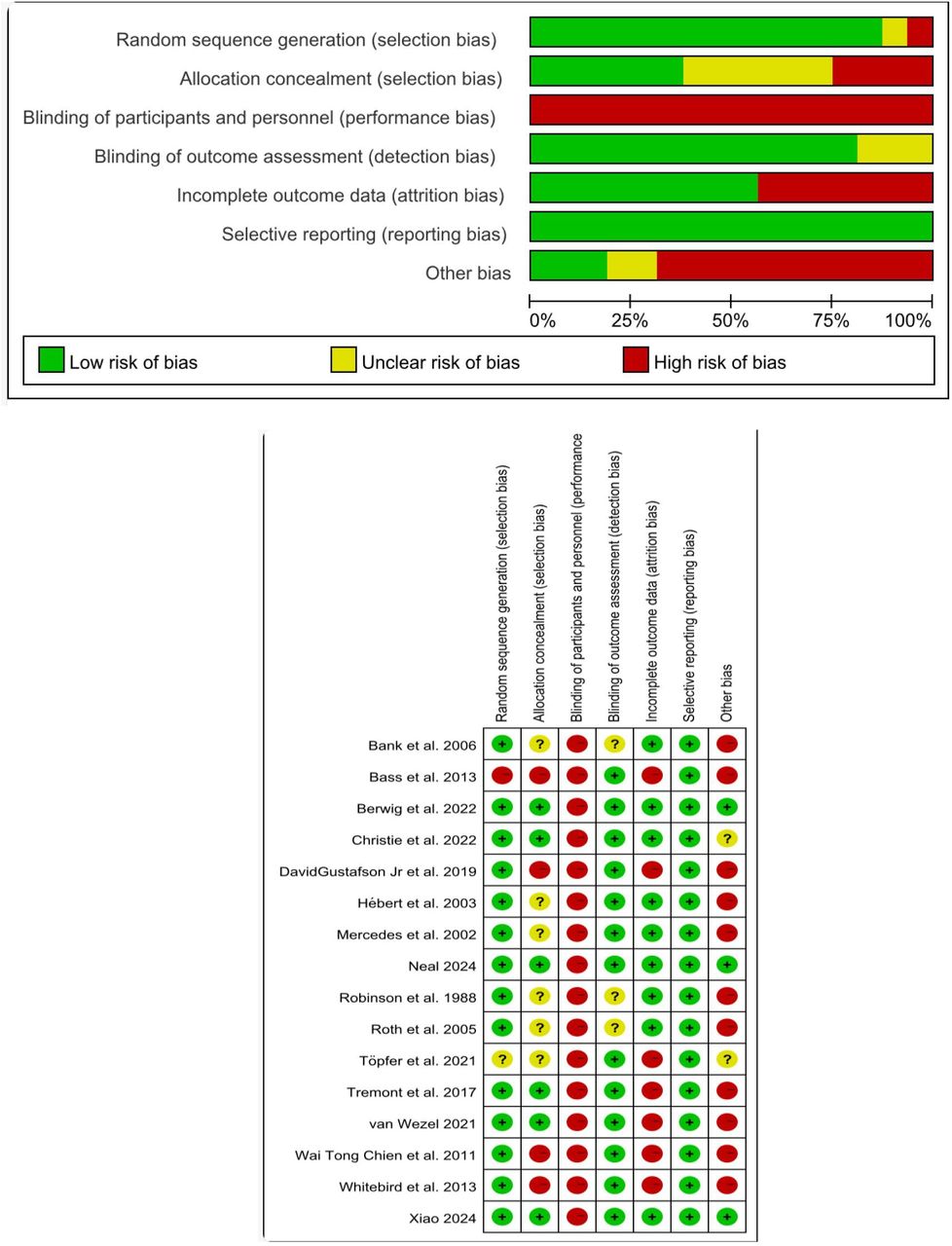
This scoping review also conducted a quality appraisal of the included RCTs, revealing that over 75% of the studies were assessed to have a low risk of bias in the subsequent domains, including sequence generation, blinding of outcome assessment and selective reporting. However, less than 60% of the studies were rated as low risk in other critical areas, such as allocation concealment, blinding of participants and personnel, incomplete outcome data; and the presence of other potential biases (see figure 2). This assessment underscores the variability in methodological rigour across the included RCTs.

{kind=link}
{kind=link}
Risk of bias graph.
Theoretical frameworks utilisation research design
Among the 31 studies, 12 studies were guided by six distinct theoretical frameworks to inform their research design: the Stress Process Model, the Sociocultural Stress and Coping Model, the Stress-appraisal Coping and the Crisis Model, the Role Transformation Framework, Rural Nursing Theory and Tolsdorf’s Conception of Social Support. Specifically, five studies followed the Stress Process Model,34 48 49 54 59 while three adhered to the Sociocultural Stress and Coping Model.40 57 60 Additionally, one study employed Lazarus and Folkman’s Stress-Appraisal Coping model alongside the Crisis Model of Moos and Tsu,61 one was guided by the Framework of Role Transformation,56 another implemented the Rural Nursing Theory51 and another one was based on Tolsdorf’s Conception of Social Support.38 Furthermore, 19 studies did not reference any theoretical framework, indicating a gap in the theoretical grounding of a significant portion of the research.
Social support measurements
As detailed in online supplemental table 2, a total of 23 methods were employed to measure social support across the studies reviewed, with the Medical Outcomes Study social support survey (MOS) being the most frequently used, appearing in five studies. The MOS is a multidimensional, self-administered and concise survey designed to measure social support among patients.65 Additionally, the Multidimensional Scale of Perceived Social Support was used in four studies, while another four studies extracted between 10 and 21 items from three different broad scales to measure social support. Several studies also developed their own measurement tools, including a 13-item questionnaire consisting of four domains: satisfaction with support, social support network, received support and negative interactions. Other instruments included the Interpersonal Support Evaluation List, a brief form of the Perceived Social Support Questionnaire, which assesses various dimensions of social support, and the Inventory of Socially Supportive Behaviours, among others. Online supplemental table 2 indicates that the majority of studies did not report on scale reliability and validity.
Supplemental material
Social support interventions
As presented in online supplemental table 3, the social support interventions identified in the reviewed studies were categorised into six distinct types based on their specific content: peer support (n=7), counselling group (n=2), health education (n=2), mindfulness-based stress reduction (n=1), individual therapy (n=1) and multicomponent interventions (n=18). Notably, one study highlighted that the development of intervention methods involved organising multiple focus groups to assess caregivers’ needs.39 The delivery of the interventions varied, encompassing online and offline and hybrid formats. 14 studies used online interventions,33 35 36 39 44 45 47 48 50 53 54 56 59 63 10 studies employed offline interventions37 38 40 42 43 46 55 57 60 61 and 7 studies implemented a combination of online and offline approaches.34 41 49 51 52 58 62 This diversity in intervention types and delivery methods underscores the multifaceted nature of social support interventions aimed at addressing various needs within different populations.
Supplemental material
Peer support
Peer-support interventions are characterised by group-based programmes facilitated by trained peers or mentors who possess lived caregiving experience. These programmes foster shared experiential learning, mutual problem-solving and emotional reciprocity among participants. In the reviewed studies, eight used peer-support interventions, comprising two RCTs and six employing mixed methods. The duration of these interventions varied, with the shortest lasting 4 hours,46 while others spanned up to 24 weeks; one study implemented a three-steps intervention over 32 weeks58 and the majority opted for a 6 months duration.35 57 62 Additionally, one study was conducted for 3 months,60 and another lasted 6 weeks.56 Among the findings, three studies showed improvement in perceived social support,35 60 62 one indicated enhanced satisfaction with social support57 and another demonstrated advancements in emotional and informational support.56 Furthermore, one study noted an increase in support from home care staff; however, improvements in support from family, friends, neighbours and advice from doctors were not statistically significant.46 Overall, one study highlighted an enhancement in overall social support,58 underscoring the potential effectiveness of peer-support interventions.
Counselling group intervention
Counselling group intervention involves caregivers participating in support groups that provided personal and family consultations. In the reviewed literature, two studies implemented group counselling interventions, both of which were RCTs. With durations of 12 months41 and 6 months.44 One study reported a significant improvement in caregivers’ utilisation of community support services; however, it noted no significant improvement in the utilisation of community services and medical resources by the care recipient.44 Additionally, another study identified 11 indicators of social support, with 8 showing significant improvement.41
Health education
Health education intervention in the context of dementia care encompasses a social skills programme aimed at enhancing caregivers’ care skills and confidence. These programmes typically involve 12 hours of sessions designed to achieve various objectives, such as developing emotional resilience, understanding the disease and fostering a sense of control. In the reviewed studies, two used health education interventions, one was an RCT, while the other was an NRCT study. The intervention duration was 2 months38 and 12 hours,55 respectively. One study reported a significant increase in service utilisation,55 indicating that the educational component effectively encouraged caregivers to seek additional resources. In contrast, the other study reported no significant increase in social support among participants.38 These findings highlight the potential benefits of health education interventions in enhancing caregivers’ skills, although the impact on social support may vary.
Mindfulness-based stress reduction
Mindfulness-based stress reduction interventions for caregivers involve weekly guidance on mindfulness principles, complemented by meditation and gentle yoga sessions led by a trained instructor. One RCT examined the effectiveness of such an intervention, which lasted for 2 months.43 The results indicated a significant improvement in caregivers’ social support following participation in the programme.
Individual therapy
The expanded Tele.TAnDem programme provided caregivers with 12 individual therapy sessions, each lasting 50 min, conducted via telephone across a 6 months period.45 This comprehensive programme included 10 therapeutic modules designed to address various aspects of caregiving. A 3-year follow-up of the study revealed that informal caregivers experienced a significant reduction in caregiver burden, improved quality of social relationships and enhanced skills in managing the behavioural issues associated with dementia. While the intervention significantly improved caregivers’ social relationships, it did not demonstrate a significant increase in service utilisation.
Multicomponent interventions
Multicomponent interventions integrate psychological education, systematic communication and physical therapy. 18 studies used multicomponent interventions, of which 6 were NRCTs, 9 were RCTs and 3 were mixed methods. The shortest intervention duration was 4 weeks,48 the longest was 18 months33 and the most common intervention duration was 6 months.39 42 47 49 51 52 54 63 Among the 18 studies mentioned above, a total of 11 studies reported a slight increase in social support without statistical significance, but also pointed out that the interventions were in the correct direction.33 36 39 41 47–49 51 52 54 63 One study reported an increase in overall social support,38 one mentioned that the intervention improved the perceived social support of caregivers,59 one mentioned an increase in emotional support61 and another mentioned a significant increase in support resources.34 Meanwhile, one study reported an increase in social support satisfaction,50 another study proposed that social support was associated with lower stress response to cope with the care recipient’s decline in function and cognitive impairment,53 by the way, one study showed that the intervention group’s utilisation of family services was significantly decreased.42
Intervention outcomes
In addition to enhancing social support, nine studies showed that intervention significantly reduced caregiver depression.34 35 43 49 52 54 55 59 63 Furthermore, eight studies reported reduced caregiver burden,38 49 50 52 54 56 57 61 while three studies reported reduced stress,34 43 56 two studies reported improved mental health of the caregivers,43 53 one study reported improved caregiver coping skills.57 Additionally, one study reported improved caregiver satisfaction,61 one study reported increased health-related quality of life47 and one study reported a significantly higher sense of competence among caregivers compared with care-as-usual.48
Qualitative research results
Among the included studies, seven studies conducted qualitative research,56 57 59–63 with all interviews conducted after the intervention. One study conducted interviews with both caregivers and older adults with dementia; the caregivers reported positive feedback while the older adults with dementia did not. Other studies described caregivers’ positive feedback from the interviews. The theme mainly focused on caregiving skills, mastery of dementia-related knowledge, benefits from interventions, satisfaction with interventions, emotions and burdens and various aspects of social support.
Discussion
Previous studies have reported interventions aimed at improving the social support of caregivers caring for older adults with dementia. Nevertheless, evidence on the categories of intervention, implementation, evaluation and effects of these interventions is dispersed in the literature, and an up-to-date summary is lacking. This scoping review comprehensively summarises existing studies published in English that describe interventions to enhance social support for dementia caregivers. Six effective interventions, including peer support, group counselling, health education, mindfulness-based stress reduction, individual therapy and multicomponent interventions were identified in this review. These interventions differed in terms of content, duration, acceptance and effectiveness.
Characteristics of the participants
Among the included studies, family caregivers consisted of spouses, children, other relatives, neighbours and friends; only one study focused on spousal caregivers,41 while the remaining studies included all categories of caregivers. Individuals with dementia are mostly looked after by informal caregivers, particularly spouses who are considered to be at a higher risk of social isolation.58 This finding shows that spouses and other caregivers exhibit different responses to social support aimed at alleviating caregivers’ pain.59 Meanwhile, social support among African Americans has gradually received more attention, with three studies investigating social support interventions for African Americans.57 59 60 According to one systematic review, almost 95% of Chinese individuals with dementia are primarily cared for by their family members at home, largely influenced by the cultural values of filial piety and Confucian traditions.66 Recent research has explored the cultural adaptation of iSupport, a global online intervention developed by the WHO for informal caregivers of people with dementia. This investigation underscores the critical need for contextually tailored interventions that align with local cultural practices and values,47 ensuring that support for caregivers is both relevant and effective in addressing their unique challenges.
Social support measures
A total of 23 different assessment tools were used to measure social support. Online supplemental table 2 shows that most studies used scales that can only measure a certain aspect of social support, such as subjective perceived social support or the level of social support judged solely by whether caregivers seek help. Only three types of tools were described in terms of their reliability and validity. Since social support is a multidimensional concept, different interventions aim to improve different dimensions. While subjective social support is difficult to measure using quantitative methods, more methods focus on objective social support and consider only some aspects of social support, such as restrictions in social participation,35 measuring supported resources,34 perceived support from significant others, family and friends,36 63 social networks and the four dimensions of functional social support23 or satisfaction with support.49 Because of the multidimensional nature of the concept of social support, the measurement results can only reflect part of the situation. Therefore, more precise measurement tools need to be developed.
Social support interventions
According to the current study, six types of interventions to improve social support exist. Apparently, support from others is crucial; caregivers of older adults with dementia need this support initially, and eventually seeking help and support. Caregivers from various regions possess distinct requirements regarding the methods and types of support they need. In the included studies, this review found that peer support can significantly enhance caregivers’ perceived social support, satisfaction of social support, emotional and informational support, as well as overall social support. Peer support has demonstrated advantages for individuals with various requirements, including alleviating depressive symptoms,60 enhancing coping strategies61 and reducing feelings of isolation and loneliness. Support provided by caregivers or volunteers with similar experience is more easily accepted by caregivers who are deeply burdened with caregiving.67 Peer support also performs well in different environments, such as in educational settings where peer support can help improve academic performance and build confidence,68 and in chronic disease management, peer-support groups have played an effective role in promoting self-management and emotional health.69 The excellent performance of peer support may be attributed to the same caregiving experience as peers.70 71 Caregivers who are burdened with caregiving are more likely to empathise with them and accept their help without reservation. At the same time, as the providers of support, with the same experience, they know better where to provide help and guidance to their caregivers.
And counselling groups can enhance social support through the utilisation of support. Counselling group is widely used in the field of mental health and can effectively improve sexual satisfaction among women with multiple sclerosis.72 And can also improve all levels of mental health of midwifery students.73 Health education, like counselling groups, improves the utilisation of support by caregivers.55 Mindfulness-based stress reduction, and individualised treatment, have good outcomes in improving social support. The findings from the included studies indicate that multicomponent interventions enhance social support for caregivers across different domains, such as emotional, practical and informational support. According to the current study, multicomponent interventions typically combine multiple interventions to address different aspects of complex problems, fit the concept of multidimensional social support and involve integrating multiple interventions in the fields of health education, care skills, coping strategies and social support for dementia caregivers, these have been demonstrated to effectively alleviate the burden on caregivers,49 50 52 54 61 decrease depressive symptoms34 49 52 54 59 63 and increase their perceived satisfaction,50 from the included studies, multicomponent interventions demonstrated moderate efficacy in improving caregivers’ perceived social support and utilisation rates59; however, only one study explored the impact of multicomponent interventions on overall social support.38
According to the included studies, this discrepancy may reflect methodological heterogeneity in intervention components (eg, variable duration, intensity) and limited generalisability due to insufficient sample diversity or longitudinal follow-up. Health education has better effects in interventions such as consultation groups. However, the angle of improvement is relatively one-dimensional, which can be used as a part of multicomponent intervention, so as to achieve multidimensional improvement. Delivery interventions include face-to-face, telephone-based and internet-based intervention, as well as online and offline combinations. Both face-to-face and online interventions have their advantages and disadvantages. The main disadvantage of face-to-face interaction is that caregivers find it difficult to leave older adults with dementia behind and go to specific institutions to receive specific interventions.35 Therefore, telephone and internet-based interventions are increasingly being applied to social support interventions. Another study indicates that technology-assisted interventions help alleviate caregiver burden and enhance support, similar to face-to-face support.63
Considering that online and offline interventions have their own characteristics and shortcomings, the combination of the two can effectively reduce inconvenience and provide better and more comprehensive application of intervention measures to caregivers, to ensure they can receive more effective support to reduce their burden, ultimately enhancing the well-being of older individuals with dementia. Only one included study derived its intervention design from prior needs assessments of caregivers in control groups. However, the small sample size limited statistical power to detect intervention effectiveness, precluding robust conclusions. Future studies should prioritise co-design methodologies grounded in user-centred needs assessments, coupled with adequately powered trials to enhance ecological validity and generalisability.58
Intervention outcomes
Drawing from the studies that were included, improvement of social support can lay a good foundation for reducing the care burden, depression and stress and eventually enhancing the well-being of caregivers and multicomponent interventions can improve multiple dimensions of social support. In the implementation of interventions in the future, smarter and easier-to-operate intervention equipment can be developed for caregivers, such as voice control or AI(Artificial Intelligence) equipment, so that their operation can be more easily mastered and the distance between people can be narrowed. Simultaneously, it is crucial to consider the unique requirements of caregivers with diverse backgrounds in order to amplify the benefits of ongoing support initiatives. In the future, it is also possible to develop interventions that simultaneously contain the essence of six categories, leverage their respective characteristics, integrate their advantages into one intervention and maximise their effectiveness. The qualitative research section supplemented the unmeasured parts of the scale. From the results, it can be seen that most caregivers provided positive feedback, and the implementation of interventions not only reduced their caregiving burden, but also enhanced their mastery of dementia-related knowledge and improved their social support. However, almost all qualitative studies are conducted after intervention, neglecting the understanding of the needs of caregivers before and after intervention. Future research can consider conducting qualitative studies before and after intervention to fully understand the needs of caregivers, develop interventions based on their reported results and conduct qualitative studies again after intervention to better improve caregivers’ social support and quality of life.
Limitations
Although this study provides a comprehensive overview of social support interventions for dementia caregivers, some methodological limitations must be mentioned. Due to language barriers, this review only included English language literature and did not include grey literature, which might have overlooked pertinent information. In addition, we included only primary studies and excluded reviews, which may have resulted in missing significant findings. Since this scoping review did not involve a quality assessment of the raw data, it may not be possible to completely rule out the impact of low-quality research on the results. In addition, as we only assessed the risk of bias of RCTs, it may not be possible to completely rule out systematic errors.
Conclusion
This scoping review comprehensively examined the landscape of social support interventions implemented in the field of dementia care; however, in the process of caring for older adults with dementia, problems remain related to caregivers seeking support and in the delivery of interventions. We suggest that combining online and offline interventions for caregivers can probably achieve the best results. Future research should integrate existing technologies and use them to provide comprehensive interventions to caregivers. Meanwhile, it is necessary to conduct research with larger sample sizes and different cultures, and identify the interventions most suitable for different types of people. Interventions with more durable effects also need to be explored.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
This scoping review did not require ethical approval because it solely analysed publicly available literature and did not involve direct research on human or animal subjects. All included studies were published, and were accessible through academic databases, ensuring compliance with ethical standards for secondary data analysis. We adhered to academic integrity principles throughout the study, including transparency in reporting methods and results, proper citation of sources, and integrity of the data used.
References
Footnotes
Contributors Guarantor is SY. SY (First Author): Develop a search strategy, Literature screening, Writing—Original draft, Creating charts and illustrations. LP: Writing—Review and Editing. JL: Writing—Review and Editing. XFX: Writing—Review and Editing. LL: Revise search strategy, Literature screening. MQ: Writing—Review and Editing. LH: Writing—Review and Editing. WJ: Revise search strategy. JZ: Literature screening. LW: Writing–Original Draft. FZ (Corresponding Author): Methodology, Writing—Review and Editing, Funding acquisition.
SY accepts full responsibility for the work and the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This work was supported by the National Nature Science Foundation of China (Grant no. 71871147), and Science and Technology Department of Sichuan Province Project (Grant no. 2024YFFK0128).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.