Article Text

Abstract
Objectives To develop and validate a simplified Bleeding Audit Triage Trauma (sBATT) score for use by lay persons, or in areas and environments where physiological monitoring equipment may be unavailable or inappropriate.
Design The sBATT was derived from the original BATT, which included prehospital systolic blood pressure (SBP), heart rate, respiratory rate, Glasgow Coma Scale (GCS), age and trauma mechanism. Variables suitable for lay interpretation without monitoring equipment were included (age, level of consciousness, absence of radial pulse, tachycardia and trapped status). The sBATT was validated using data from the UK Trauma Audit Research Network (TARN) registry.
Setting Data sourced from prehospital observations from multiple trauma systems in the UK.
Participants 70 027 motor vehicle collision (MVC) patients from the TARN registry (2012–2019). Participants included were those involved in MVCs, with exclusion criteria being incomplete data or non-trauma-related admissions.
Interventions Not applicable.
Primary and secondary outcome measures Death within 24 hours of MVC. Secondary: need for trauma intervention.
Results In a cohort of 70 027 MVC patients, 1976 (3%) died within 24 hours. The sBATT showed an area under receiver operating characteristic curve of 0.90 (95% CI: 0.90 to 0.91) for predicting 24-hour mortality, surpassing other trauma scores such as the Shock Index and Assessment of Blood Consumption score. Sensitivity was 96% and specificity 72%, with a negative likelihood ratio below 0.1, indicating strong rule-out capability. Sensitivity analyses confirmed consistent performance across varying SBP and GCS thresholds. The sBATT was equally effective across sexes with no significant predictive discrepancies.
Conclusions The sBATT is a novel, simplified tool that performs well at predicting early death in the TARN dataset. It demonstrates high predictive accuracy for 24-hour mortality and need for trauma intervention. Further research should validate sBATT in diverse populations and real-world scenarios to confirm its utility and applicability.
- ACCIDENT & EMERGENCY MEDICINE
- TRAUMA MANAGEMENT
- Triage
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Clearly understood and patient centred outcome measure (24-hour mortality) and a large validation cohort (70k + patients).
Sensitivity analyses across different physiological thresholds (eg, systolic blood pressure, Glasgow Coma Scale) and demographic groups (sexes).
Validation cohort consisted of patients from the UK, limiting generalisability to other geographic regions, particularly lower and middle income countries where emergency medical services availability and patient demographics may differ significantly. The actual implementation and feasibility of using simplified Bleeding Audit Triage Trauma (sBATT) by lay persons were not directly assessed and would require further investigation.
Deriving and validating such a scoring system from the same dataset can lead to overfitting, where the model performs well on the training data but may fail to generalise to new data.
Data Source Bias: Trauma Audit Research Network only includes cases that were severe enough to warrant inclusion in the registry with an injury severity score >9; we do not know how sBATT performs in those with minor or no injuries.
Background
Road traffic injury is the leading cause of death in children and young adults aged 5–29 years.1 In addition to the 1.3 million deaths per year associated with road trauma, an additional 20–50 million people incur significant injury and often long-term disability.1 Ninety-three per cent of fatalities occur in lower and middle income countries (LMICs) where emergency medical services (EMS) are often not available.2 3 In many such countries, motor vehicle collisions (MVCs) are attended by lay bystanders, non-clinical professionals (such as firefighters) and frequent road users such as taxi drivers.4–6 These non-clinical responders will not have access to physiological monitoring equipment which is ubiquitously available to clinical responders in higher income countries (HIC).
Following an MVC, up to 40% of patients may remain trapped in their vehicle which may be for an extended period of time.7–10 These patients have more severe injuries and an excess mortality.9 The application of physiological monitoring equipment to a patient and the clinical responders’ interaction with this system are associated with prolonged entrapment times.10 New UK national guidance recognises that frequent clinical monitoring may prolong entrapment time and as such should be kept to the minimum.11
In established emergency care systems, initial risk stratification occurs with a patient or bystander call to EMS, with key data points extracted through conversation inputting into algorithmic decision trees. Systems such as advanced priority medical dispatch system tend towards being sensitive but not specific.12 Such systems have low specificity which may result in unnecessary resource utilisation. This in turn may prolong response times to subsequent incidents, and limit availability of EMS, especially in LMICs where resource is already most limited. In both LMIC and HIC, decision-making at initial emergency call may activate varying levels of ambulance service response from first responders through to critical care teams. Depending on patient condition, instructions to bystanders may be given, for example, to start cardiopulmonary resuscitation or arrest haemorrhage. Bystander instructions for the approach to trauma patients vary significantly between regions and often specific instructions are not available.13 Accurate early risk stratification is challenging and fundamental to the chain of survival for patients with trauma as it ensures optimum use of clinical and operational resources.14 15
The Bleeding Audit Triage Trauma (BATT) score is a simple triage tool that has been derived from an international cohort of trauma patients across 274 trauma centres and validated in a variety of European settings.16 This score includes systolic blood pressure (SBP), heart rate (HR), respiratory rate (RR), Glasgow Coma Scale (GCS), age and simple mechanism of trauma (high-energy and penetrating injury). BATT has been identified as a tool that is useful in ensuring equitable and appropriate utilisation of Tranexamic Acid (TXA) and is both sensitive and specific at predicting death from bleeding at 24 hours.16 The BATT outperforms other recognised scoring systems such as the Shock Index (SI).16
The purpose of this study is to validate a simplified BATT (sBATT) score derived from the initial prognostic model equation of BATT using clinical variables that may be measured in environments where physiological monitoring equipment is unavailable, is impractical, or may prolong entrapment times.
Methods
This study consists of a validation of a simplified version of the BATT score in the Trauma Audit Research Network (TARN) data and compared with existing trauma score.
The original BATT was previously developed in an international cohort of 23 202 injured patients treated in 274 trauma centres in 40 countries and subsequently validated in different European studies to predict death due to bleeding and early death.16–18 In this study, the sBATT was developed by simplification of the covariables used in the original BATT to be collected without monitoring equipment (table 1). The sBATT weighting was derived using the integer from the coefficient of the regression equation of the prognostic model previously published (ref bmj open 17). Points were assigned based on their significance (table 1) giving a sBATT range from 0 to 14.
Variables suitable for use by bystanders from original BATT and their suggested lay application
Primary outcome
Death within 24 hours. This is the most relevant primary outcome as bystander and prehospital care is most likely to impact on early deaths.14
Secondary outcome
Need for trauma intervention (NFTI). We used a previous definition of NFTI which includes transfusion, damage control surgery or intensive care unit admission.19
Comparison
The performance of the sBATT is compared with other frequently used trauma scores including the original BATT, the Assessment of Blood Consumption (ABC) score, Shock Index (SI), Kampala Trauma Score (KTS), Mechanism/Glasgow Coma Scale/Age/Pressure (MGAP) and Revised Trauma Score for Triage (T-RTS).20–24
We considered the UK TARN registry in patients injured in an MVC between January 2012 and December 2019 to validate the sBATT. See Box 1 for inclusion and exclusion criteria for TARN.
Inclusion and exclusion criteria for the UK Trauma Audit Research Network (TARN)
The TARN database includes data on patients with an injury severity score of 9 or more who are admitted to hospital in England and Wales for at least three nights, died in hospital or were transferred to another hospital for specialist care. TARN exclude patients with isolated mild traumatic brain injury with loss of consciousness, superficial scalp injury, patients 65 years or older with femoral neck or single pubic rami fracture, fracture or dislocation of the foot or hand, closed fracture or dislocation of an isolated limb, or simple skin laceration with blood loss <20%.
Continuous variables were described by the mean and SD or the median and IQR according to the parametric or non-parametric distribution.
We estimated the discrimination of each trauma score. Sensitivity (Se) is the true-positive rate from which the false-negative rate (commonly named under-triage) is derived. Specificity (Sp) is the true-negative rate from which the false-positive rate (commonly named over-triage rate) is derived. We plotted the receiver operating characteristic (ROC) curves for each score. We calculated the area under the ROC curve (AUROC) as an overall indicator of discrimination. An AUROC of 1 corresponds to an ideal score. We calculated the likelihood ratio (LR). A positive LR of 10 or above results in a large increase in the probability of the outcome and a negative LR of 0.1 or less results in a large decrease in the probability of the outcome. In trauma risk stratification, a negative LR is the most useful indicator to safely rule-out injured patients who do not have major trauma.
Because AUROC is a composite of sensitivity and specificity and as such has little practical application for clinical decision-making, we plotted separately the sensitivity and the specificity for each value of the score with a grey zone approach.25 The grey zone approach identifies two boundaries of a score threshold corresponding to different objectives in clinical decision-making. The lower boundary represents the ‘rule-out’ limit in which major trauma could be safely excluded. The American College of Surgeons recommends an under-triage rate less than 5%, that is a sensitivity higher than 95%.26 To avoid overloading of the trauma system, over-triage should not exceed 50% at this boundary. The upper boundary represents the ‘rule-in’ limit in which major trauma is highly certain. A specificity of 90% or higher is usually acceptable for recommending an expensive intervention, a treatment with serious side effects or the use of scarce resources. For trauma risk stratification, the ‘rule-in’ boundary is often not useful.
It is important that trauma scores perform equitably for women and men; we report a sex-disaggregated analysis of the sBATT to evaluate this.
Missing data
Multiple imputation by chained equations was used in replacement of missing data. We drew 20 imputed datasets to impute values for SBP, HR, RR and GCS. We did not report any missing value for the outcomes.
Sensitivity analysis
There will be a range of accuracy of interpretation of the parameters included in the sBATT. This is particularly the case for the ‘GCS’ where we could find no supporting literature on lay application and interpretation, and ‘the absence of a radial pulse’ where a range of collected minimum SBP values (55–85 mm Hg) were reported.27–30 To allow for this, we performed sensitivity analysis with a GCS of 13 for level of consciousness and an alternative threshold of 60 mm Hg of SBP for the loss of radial pulse.
All analyses were performed using STATA software (V.16.1; StataCorp, Station, TX, USA).
Ethics approval and consent to participate
TARN data analyses are conducted using anonymised data which are governed by a code of practice approved by the Confidentiality Advisory Group who are appointed by the Health Research Authority. Additional individual ethical approval was not required for this analysis.
Patient and public involvement
Patients or the public were not involved in the design, conduct, or reporting, or dissemination plans of this research.
Results
Patient characteristics
Overall, 70 027 patients were included in the TARN registry and injured in an MVC between 2017 and 2021. The mean age was 46 (SD 20) years (table 2). There were 13 851 (20%) older injured patients over 65 years and 18 175 (26%) women. Entrapment was recorded for 7 754 (11%) patients. The mean injury severity score was 17 (SD 12). There were 1976 (3%) patients who died at 24 hours and 3868 (6%) died at 30 days. Considering each score threshold to identify injured patients with significant risk of early death, 20 082 (29%) injured patients were considered at risk with a sBATT ≥3, 7407 (11%) patients with a SI ≥0.9, 9393 (13%) patients with an MGAP <23, 27 650 (40%) patients with a KTS ≤13 and 12 627 (18%) patients with a T-RTS ≤11.
Characteristic of the study population presenting vehicle incident or collision
Trauma score performance
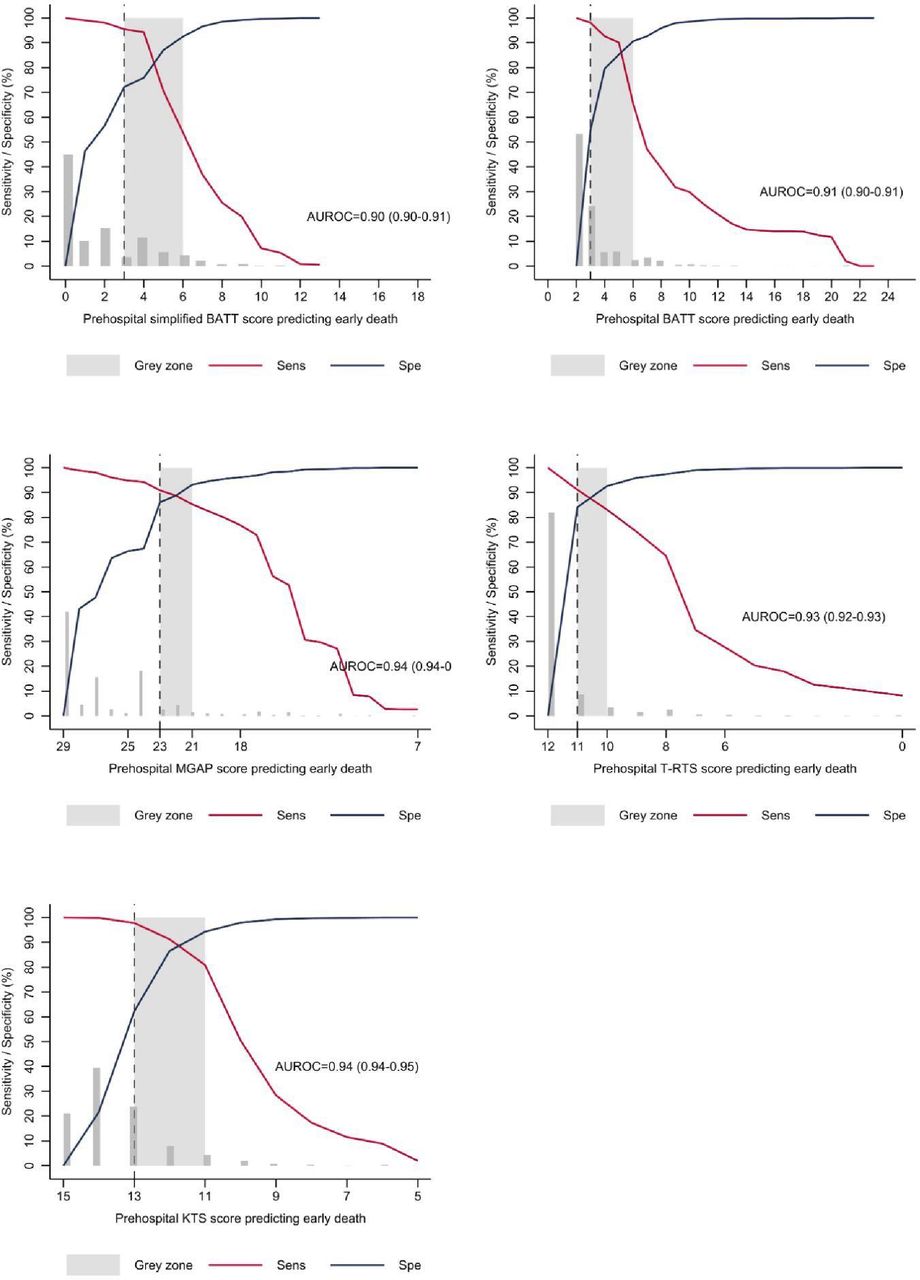
The AUROC for the sBATT was 0.90 (95% CI: 0.90 to 0.91) (table 3 and figure 1). BATT, MGAP, T-RTS and KTS scores presented an AUROC between 0.91 and 0.94. The SI and the ABC score presented a low discrimination with an AUROC less than 0.70. The sensitivity of all scores was above 0.90 except for the SI and the ABC score. The negative LR of the sBATT, BATT and KTS scores was below 0.1. The grey zone approach showed appropriate sensitivity for the rule-out limit with specificity exceeding 50% for sBATT, BATT, MGAP, T-RTS and KTS (figure 2). The sensitivity analysis of different thresholds of SBP and GCS of the sBATT did not show a difference on AUROC, sensitivity and negative LR (table 4). The performances of all scores to predict NFTI were between 0.70 and 0.75 and were summarised in online supplemental figure 1. The sex-disaggregated analysis did not find any heterogeneity of the AUROC and negative LR by sex (online supplemental table 1). The performance of the sBATT to predict secondary outcomes (NFTI and NFTI or death) was summarised in online supplemental table 2.
Supplemental material
Discrimination of the different trauma scores

Receiver operating characteristic curves for trauma scores predicting early death.

{kind=link}
{kind=link}
Sensitivity and specificity with grey zone approach.
Sensitivity analysis according to systolic blood pressure (SBP) and Glasgow Coma Scale (GCS) threshold.
Discussion
We present the sBATT, a novel trauma score which uses clinical variables that may be measured in environments where physiological monitoring equipment is unavailable or impractical. The sBATT performs well at predicting death at 24 hours with an AUROC of 0.90 (95% CI: 0.90 to 0.91). This performs well compared with the original BATT and other established trauma scores. Neither established trauma scores or sBATT performed well at predicting NFTI-Death or NFTI alone.
Our study has important strengths. sBATT was derived and validated within TARN, a well-established UK dataset with high standards of data collection and validation. We have assessed the performance of the score across values to allow for the range of SBPs at which a radial pulse might be lost and at which GCS could be incorrectly allocated—the consistently high AUROC across these ranges adds strength to the utility of the score. This score is unique in that we have demonstrated its performance for injured females and males. The precision of our results is enhanced by the substantial number of patients included in this study. Predictor variables had minimal missing values and there was no absence of outcome data (table 2). The outcome was clearly defined and documented at a specific time point, contributing to the robustness of the results.
Our research also comes with constraints. The accuracy of predictor variable measurements may impact discrimination and calibration. Random errors could potentially emerge in all predictors (SBP, HR, GCS), resulting in diminished discrimination and calibration. The use of monitoring devices to collect the original TARN data may be prone to systematic errors, which are likely to influence calibration.31 The rate of missing data is relatively high and may lead to bias or misclassification. However, we performed multiple imputation to fulfil the missing value of physiological parameters. As missing values are more likely to be missing at random and dependent on the outcome, multiple imputation is more appropriate than complete case analysis that may lead to bias towards the null. Deriving and validating such a scoring system from the same dataset can lead to overfitting, where the model performs well on the training data but may fail to generalise to new data.32 This approach may inadvertently capture noise or specific characteristics of the dataset rather than true physiological relationships. Our validation on the TARN dataset threatens the external validity of the sBATT and risks an overoptimistic performance estimate. The TARN database includes a more severely injured population than typical MVC patients encountered by EMS in limiting generalisability; further, differences in measurement timing may affect transportability of the result to lay persons, requiring validation before use by EMS or laypersons in other settings. Validation from a non-TARN dataset, from settings other than high-income countries, and/or a dataset for each intended population group is an important next step.
Frequently used trauma scores rely on physiological data and/or specific details of the injuries sustained. We could not identify a comparable trauma score that had been rigorously derived and did not rely on variables that were captured by a monitoring device. This limits the utility of other scores to contexts where clinical professionals are able to undertake such monitoring or where the necessary equipment is available. Nordberg and team developed a simplified bystander score and demonstrated its utility in the hands of untrained lay rescuers; the efficacy of the sBATT when used by untrained lay rescuers, trained lay rescuers and professional bystanders (such as police and fire services) would similarly need to be ascertained.33 Such validation would be necessary in each target population and region to ensure utility, accuracy and acceptability across a range of sociocultural contexts.
Ninety-three per cent of road trauma deaths occur in LMICs.1 LMICs are a large range of countries and regions: often with disparate approaches to road trauma, a wide range of nascent and evolved EMS and sociocultural differences that may affect the utility and adoption of such a score by lay and professional bystanders. As such, significant validation and context-specific adaptation will be required in relation to sBATT.
Subject to appropriate validation sBATT has significant potential for utilisation in environments where physiological monitoring systems are not available or impractical. The use of the sBATT by those first on scene may add utility through enabling more accurate risk stratification and as such dispatch of specialist resources to the scene, trigger particular care pathways such as the administration of intramuscular TXA and improve multidisciplinary on-scene communication through the use of a common language which delineates casualty severity. Members of this team have previously demonstrated the inequitable administration of TXA to women, and the adoption of a score such as this and its incorporation into documents that guide practice such as Patient Group Directives could help overcome these inequalities.34 Patients that are trapped following an MVC have significant injuries and are more likely to die.9 Previous work has demonstrated that pauses in extrication for physiological monitoring contribute to extended entrapment times.10 The use of sBATT may offer an opportunity to decrease entrapment times as it has the potential to be performed quickly and with minimal disruption to the process of extrication. The ‘extrication buddy’ who joins the patient in the vehicle to explain the extrication process will be well placed to use the sBATT.11 Further exploration of these areas in relation to the utility of sBATT from a clinical, operational and systems perspective is justified.
Key questions as to how the sBATT performs in different population groups and when delivered by a range of clinicians, non-clinical professionals and bystanders are essential next steps. In particular, studies should address the question of lay persons ability to determine hypotension and tachycardia as defined in sBATT. Following validation studies, prospective clinical, operational and communication effectiveness studies of the performance of sBATT in the hands of clinicians caring for trapped patients following an MVC are warranted.
Conclusion
We present sBATT, a simple and reliable trauma score for use in patients injured in MVC to predict early death. This score has the potential to be used in various settings where monitoring equipment is unavailable or impractical. Future studies should validate the use of this tool by lay persons in a variety of healthcare environments.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
TARN data analyses are conducted using anonymised data which are governed by a code of practice approved by the Confidentiality Advisory Group who are appointed by the Health Research Authority. Additional individual ethical approval was not required for this analysis.
References
Footnotes
X @timnutbeam, @willem_stassen, @ageron_fx
Contributors TN, FXA, EF and WS contributed to the conception and study design, analysis and interpretation of data, and drafting and revising the manuscript. All authors read and approved the final manuscript. FXA is the guarantor.
Funding This work was supported by Vision Zero South West (UK) grant number DA01.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.