Article Text

Abstract
Objectives To collaboratively develop a music-supported video-based exercise programme for people with multiple sclerosis (pwMS) with mild to severe disability.
Design and setting We performed this participatory mixed methods study from 15 March 2022 to 22 July 2023 at two Austrian multiple sclerosis (MS) centres.
Participants This research included 67 pwMS, of whom 18 pwMS (including two patient representatives and five MS support group leaders/members) and an additional three family members served as stakeholders. Six neurologists and six physiotherapists, each with >5 years of experience in treating pwMS were interviewed.
Intervention Stakeholders actively participated as members of study advisory, project steering and research groups. Researcher-supported peer-to-peer focus groups and individual interviews, conducted in three stages, gathered information on musical preferences and exercise needs. We co-developed, co-evaluated and co-adapted the music-supported exercise programme with the stakeholders. Involvement levels were measured using the Participation Check and Patient Public Involvement (PPI) Assessment Survey, self-efficacy with the Unidimensional Self-Efficacy Scale for Multiple Sclerosis and emotional states with the Self-Assessment Manikin.
Results We identified four themes through reflexive thematic analysis: (1) engagement; (2) ease; (3) autonomy; (4) musical meaning. Integration of qualitative and quantitative components highlighted the success of PPI activities: (a) 148 co-created, free videos are publicly available; (b) four videos provide expert interviews with general information, while 144 offer music-supported exercises tailored to pwMS with mild to severe disability; (c) patients found the videos relevant, feasible and usable in interviews and focus groups; (d) ‘easy’ category exercises (seated or lying) are suitable for severely affected pwMS; (e) stakeholders felt included, respected and heard, as shown by quantitative PPI assessments.
Conclusions Stakeholders were essential in identifying key aspects, preferences and constraints early on. Their feedback on music and exercise shaped the project. This study transformed our approach to exercise for pwMS. Future studies are required to evaluate the programme’s efficacy.
Trial registration number DRKS00027979.
- multiple sclerosis
- patient participation
- exercise
- qualitative research
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This participatory mixed methods study actively involved people with multiple sclerosis (pwMS) in the collaborative development of a music-supported exercise programme.
Purposeful and word of mouth sampling ensured the involvement and participation of a diverse and representative group of pwMS ranging from mild to severe disability.
Early and continuous involvement of pwMS, including multiple sclerosis support group leaders/members and patient representatives, and their family members as stakeholders, enhances the relevance and trustworthiness of our findings.
Although the programme includes a wide range of exercises, it is not comprehensive and could be expanded in future work, with additional options for individualised music selection.
Due to the limited timeframe of this externally funded study, it has not yet been possible to assess the safety, feasibility and effectiveness of the co-created music-supported exercise programme, representing a study limitation.
Introduction
Multiple sclerosis (MS) is a chronic disease of the central nervous system characterised by inflammation, demyelination and secondary neurodegeneration.1 MS is the leading cause of non-traumatic disability in young adults,2 3 impacting physical, cognitive and emotional functioning, as well as the ability to engage in daily activities, overall quality of life (QoL) and employment.4 Growing evidence suggests that exercise serves as a beneficial rehabilitation strategy for people with MS (pwMS).5 Through systematic reviews and meta-analyses, it has been concluded that exercise can improve physical fitness and walking ability,6 7 balance,8 cognition,9 fatigue and QoL in pwMS.10 11 Despite the overall benefits that exercise can offer, a majority of people with disabilities, including pwMS, are not sufficiently physically active.12 Significant external barriers include bodily limitations, challenges accessing services and limited transportation options.13 Fatigue and a linked lack of motivation are significant internal factors hindering exercise in pwMS.14 Consequently, ensuring exercise interventions are enjoyable is a crucial aspect to promote long-term adherence.15 Incorporating music into exercise programmes may enhance exercise enjoyment and effectiveness.16 In pwMS, music-assisted training has shown promising results in improving fatigue, walking ability,17–19 balance, reducing falls19 and enhancing overall QoL.18 Dancing, for instance, has shown promise in improving physical functions in various conditions like Parkinson’s disease (PD),20 stroke21 and MS.22 Research has demonstrated the effectiveness of a 12-week movement-to-music programme for pwMS, which focused on improving strength, cardiorespiratory endurance and balance.23 While the expert-designed intervention addressed relevant aspects, it did not target pwMS with severe disability.
Comprehensive guidance on intervention development recommends starting by identifying the problem, gathering evidence and theory, understanding the problem, determining needs, evaluating the context and considering stakeholder perspectives. The process should then be modelled and the intervention designed.24 25 Employing qualitative methods, leveraging existing evidence and theories, understanding the context, focusing on future real-world implementation and incorporating stakeholder input throughout the design and refinement process26 increases the likelihood of creating effective, well-adopted and context-suitable interventions.24 This patient and public involvement (PPI) approach emphasises collaboration and co-production, with patients and researchers working together as equal partners.27 28
So far, a co-produced music-supported exercise programme for pwMS is missing. Therefore, this study aimed to (1) collaboratively develop, evaluate and refine a music-supported exercise programme for pwMS and (2) evaluate stakeholders’ level of involvement in collaboratively designing, assessing and modifying a music-supported exercise programme for pwMS with varying levels of disability.
Methods
Design and setting
For this participatory study, an embedded mixed methods design was used, featuring a primary qualitative component within a constructivist research paradigm, focused on reflexive thematic analysis.29 Research team members and stakeholders conducted 12 semi-structured focus groups and 38 individual interviews, 14 of which were peer-to-peer (figure 1). In peer-to-peer focus groups, stakeholders conducted interviews while participants with MS contributed to the discussions, with a researcher always moderating. Six neurologists and six physiotherapists (healthcare professionals), each with >5 years of experience in treating pwMS were also interviewed. The research team comprised both female and male neurologists and physiotherapists with PhD, MD or MSc degrees, all of whom received training in qualitative and mixed methods research. A music-supported exercise programme was co-created using an iterative process, guided by relevant systematic reviews30 31 and MS rehabilitation guidelines.32 The music selection for the intervention adhered to the British Association of Sport and Exercise Sciences guidelines,33 incorporating both theoretical and practical insights from pertinent publications in the field.34–36 The quantitative component was used to evaluate stakeholders’ level of involvement, self-efficacy and emotional states. The study was carried out from 15 March 2022 to 22 July 2023 at the Departments of Neurology, Clinic for Rehabilitation Muenster (RZM) and Medical University of Vienna (MUW), Austria. The trial registration number is DRKS00027979.

Overview of study activities. MS, multiple sclerosis; pwMS, people with multiple sclerosis.
Public and patient involvement
The study followed a partnership-focused approach using the framework of good practice for public involvement in research (INVOLVE: promoting public involvement in National Health Service, public health, and social care research).37 38 Essential values in public involvement include mutual respect, support, transparency, responsiveness, equitable opportunity and accountability.38 The research team comprised stakeholders and experienced healthcare professionals from the neurology departments of two medical centres. PwMS, including MS support group leaders/members and patient representatives, and their family members actively participated as stakeholders in study steering and advisory boards (online supplemental figure 1). The stakeholder team included musicians, physiotherapists and music therapists. These context factors were chosen to facilitate the PPI process. Methods employed included co-creation workshops, interviews, exercise programme co-development and co-evaluation, data co-analysis, co-video production and co-dissemination (online supplemental table 1). Building trust and facilitating knowledge sharing was central to the study, achieved by connecting all participants. Stakeholders were compensated through a PPI funding scheme with financial reimbursement or equivalent vouchers.39 Stakeholders shared study results, social media content and patient magazine articles with participants and the public and contributed to a youth culture radio station report to ensure findings aligned with their priorities, experiences and preferences.
Supplemental material
Supplemental material
Study population
The study was advertised via flyers in social media and homepage posts. Purposeful sampling was used to select the stakeholders, and word of mouth was employed for recruiting participants. PwMS treated at the study centres were screened by neurologists regarding their eligibility for study participation. To obtain diverse and in-depth insights into experiences, needs, perceptions and preferences, we included 67 pwMS and three family members in the study, increasing the initial sample size from 58 to ensure data saturation. Among the 67 participants, 18 pwMS and an additional three family members served as stakeholders. Of the 18 pwMS stakeholders, two were patient representatives and five were leaders (two) or members (three) of MS support groups.
Men and women diagnosed with MS according to the 2017 revised McDonald criteria,40 aged ≥18 years, with any MS disease course (relapsing-remitting MS, primary progressive MS, secondary progressive MS41), intact cognition assessed by a neurological examination and combined oral and written symbol digit modalities test (SDMT)42 z-scores > −1.543 and German speaking were included. PwMS with comorbidities (such as malignancies, other neurological disorders like dementia or epilepsy or psychiatric disorders such as depression or bipolar disorder), or any other impairment or condition that, in the investigators’ judgement, would prevent meaningful participation in the study (eg, cardiovascular impairment classified as New York Heart Association III and IV, or within the 3-month phase after MS relapse), were excluded. Additionally, 12 healthcare professionals, each with over 5 years of experience in treating pwMS, were individually interviewed about the primary requirements of exercise programmes for pwMS.
Co-creation process and data collection
Demographic and disease-specific data were collected from pwMS either directly or extracted from recent medical records at the study centres. The data included age, sex, years of education, cognitive function (SDMT),42 MS phenotype, disease duration and level of disability assessed through the Expanded Disability Status Scale44 scores categorised as 0–3.5 (mild), 4.0–6.0 (moderate) and 6.5–8.0 (severe)45). For family members, data collected included age, sex, years of education and their relationship to the pwMS.
The co-design process involved 38 semi-structured individual interviews, 14 of which were peer-to-peer and researcher-supported. Nineteen participants were interviewed both individually and in focus groups on two occasions, and 13 were interviewed on three occasions to ensure knowledge transfer and obtain repeated feedback during the intervention development stages. Experienced members guiding newer ones, while feedback was gathered from both original and new participants to enhance the co-design process and encourage diverse perspectives. Furthermore, 12 focus group sessions were carried out in various formats—such as in-person, online and hybrid—based on the preferences of pwMS, with group sizes ranging from three to five people (one group of three, two groups of four and nine groups of five). Severely affected pwMS were offered home visits. The interviews served as the basis for developing (stage 1) and evaluating the music-supported exercise programme (stage 2) and videos (stage 3) (see online supplemental tables 2-4 for interview guides). Discussions explored patients’ lived experiences, needs, preferences and barriers to exercising.46 Stage 1 collected data on music and exercise preferences to co-create the intervention. In stage 2, the programme was presented, discussed and adapted as needed. In stage 3, the completed videos were evaluated. Focus groups and individual interviews lasted 90–120 min. Interview duration with healthcare professionals ranged between 30 and 60 min. All interviews were audio-recorded, and field notes were taken. Online supplemental table 5 provides detailed information on the stakeholders and participants at centres RZM and MUW during visits 1–8, focus groups and interviews.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Integrating the qualitative and quantitative components, the predetermined success criteria for PPI activities were evaluated as follows: (a) co-created music-supported exercise videos, (b) videos containing general information and exercise instructions in appropriate language, (c) patient ratings of the videos as relevant, feasible and usable, (d) predefined exercises being performable by severely affected people with MS and (e) stakeholders feeling included, respected and listened to.47
Quantitative data were gathered at the end of each visit in the clinic using paper questionnaires. For online stakeholders, the survey was emailed or mailed to them for return by mail. Levels of involvement were assessed throughout the project using the German-language Participation Check (PC) to identify and address potential barriers. The PC evaluated participants’ comfort with the event, implementation quality and satisfaction with the takeaways, rated on a scale from 1 (‘not at all satisfied’) to 5 (‘very satisfied’).48 Additionally, the involvement of pwMS at the final co-creation meeting was assessed using the PPI Assessment Survey (PAS).49 The nine-item PAS is a validated, co-designed and user-friendly questionnaire designed to help researchers minimise or avoid risks during the PPI process. On a scale from 0 (‘very dissatisfied’) to 10 (‘very satisfied’), the PAS assesses informational, procedural and quality value categories, providing an overall satisfaction score.49 A preformatted Excel file with embedded analysis formulas is available for use with the PAS. Responses for each question are flagged as ‘immediate attention required’ (0–3), ‘some attention required’ (4–6) or ‘no attention required’ (7–10). If the Global Assessment Score is within the mean±2 SDs (as determined in the PAS pilot), a ‘PASS’ flag is generated; otherwise, a ‘FAIL’ flag is issued, indicating the data should be interpreted with caution.49
MS-related self-efficacy was assessed using the validated German version50 of the Unidimensional Self-Efficacy Scale for Multiple Sclerosis (USE-MS).51 The self-report USE-MS has demonstrated reliability and validity for assessing self-efficacy in pwMS.51 52 Scoring involves summing all 12 items, with items 5, 7–9 and 11 being reverse scored. The USE-MS uses a 4-point Likert scale (0=strongly disagree to 3=strongly agree), where a higher total score indicates stronger self-efficacy.
Emotional states of pleasure, arousal and dominance were assessed using the pictorial Self-Assessment Manikin (SAM).53 54 This tool features graphic characters arranged horizontally on a 9-point scale, with pleasure represented by figures from frowning to smiling, arousal depicted from sleepy to wide awake (with an incremental explosion at the centre) and dominance ranging from a very small character to a very large one.53 Due to its concise format, SAM effectively captures emotional responses across various elicitation methods and has been widely used in numerous studies.55
Data analysis
Focus groups and interviews were audio-recorded, transcribed according to content-semantic transcription system by Dresing and Pehl56 (BF, SM, NL, IH, FF). To ensure objectivity and analytical integrity, interview data from each study site were independently analysed by researchers who were not involved in the interviews. For example, interviews conducted by BF were analysed by IH and SM and the final analysis was independently checked by another researcher (BS). Data analysis used MAXQDA (2022) and f4 (Dresing & Pehl, Germany) qualitative analysis software, employing inductive reflexive thematic analysis.57 German language quotes were translated into English by the researchers and the translation checked and refined by a bilingual English native speaker. The dataset underwent iterative review by six stakeholders and six researchers, employing a mixed coding approach for attributes based on the research questions. Codes were refined iteratively, ensuring coherence and distinctiveness, following principles outlined by Braun and Clarke.57–59 Themes were created and reorganised iteratively based on Patton’s internal homogeneity and external heterogeneity criteria.60 Initial coding framework was discussed by the research team, leading to identification, refinement and naming of themes, described with quotes in the final analysis.
The statistical data analysis was conducted using IBM SPSS software, V.28.0 (IBM, Armonk, New York, USA). Descriptive statistics were employed as appropriate, with continuous data subject to normal distribution assessment through the Shapiro-Wilk test. Absolute and relative frequencies were used for count and nominal data, while normally distributed continuous data were presented as the mean (SD). Continuous data that did not conform to a normal distribution and ordinal survey data were presented as the median (minimum–maximum).
Reporting
Reporting of this participatory mixed methods study adheres to the Good Reporting of A Mixed Methods Study checklist61 (online supplemental file 1), the Consolidated criteria for Reporting Qualitative research62 for the primary qualitative component (online supplemental file 2) and the Guidance for Reporting Involvement of Patients and the Public63 (online supplemental file 3).
Supplemental material
Supplemental material
Supplemental material
Results
A total of 18 stakeholders with MS, three family members of pwMS and 49 pwMS were included. All stakeholders and participants completed the study. Baseline data are presented in table 1.
Participants’ baseline characteristics
Table 2 presents the stakeholders and participants in visits 1–8, focus groups and interviews, along with a summary of the findings.
Stakeholders and participants in visits 1–8, FGs and interviews
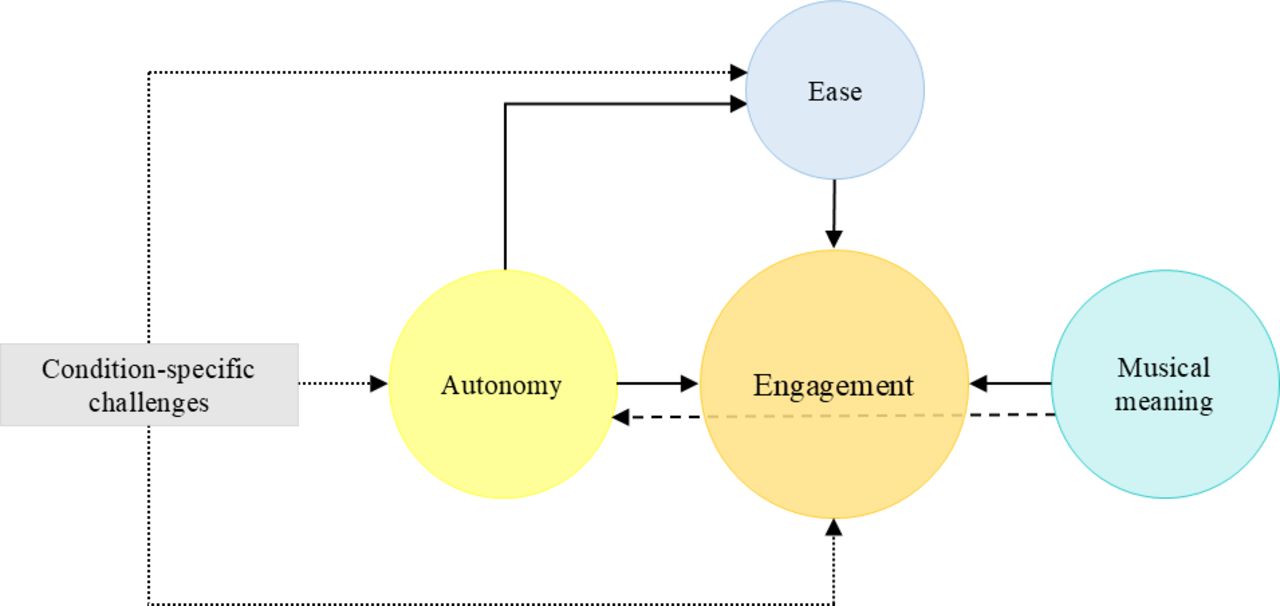
The following four themes were identified through thematic analysis, each accompanied by subthemes: (1) engagement; (2) ease; (3) autonomy; (4) musical meaning. See figure 2 for a thematic map, table 3 and online supplemental tables 6 and 7 for a coding tree and unifying themes, subthemes and additional example quotes, respectively.
Supplemental material
Supplemental material

{kind=link}
{kind=link}
Thematic map. Engagement serves as the central theme, closely linked with musical meaning, autonomy and ease. Within the broader context of condition-specific challenges, ease and autonomy themes are intertwined. Strong relationships among themes are represented by solid lines, moderate connections by dashed lines and contextual influences by dotted lines. A strong relationship between themes was observed when quotations within those themes exhibited frequent and substantive content-related linkages. Moderate connections were characterised by less pronounced associations and relationships between codes across different themes. Contextual influences refer to factors that subtly shape a theme.
Themes, subthemes and example quotes
Theme 1: engagement
Enhancing emotional well-being and resilience
Participants emphasised the exercise programme’s role in enhancing physical ability and emotional well-being. The positive impacts of regular exercise on mental health—such as stress reduction, improved mood and enhanced cognitive function—were also highlighted. They agreed that a co-designed, music-supported exercise programme should ensure enjoyment and contribute to long-term commitment and adherence. Gamification elements were seen as effective in increasing appeal and promoting long-term commitment to physical activity. Participants viewed the motivational speech as vital for inspiring pwMS, given the disease’s progressive nature. Achieving physical activity goals, regardless of difficulty, fosters a sense of accomplishment that boosts self-confidence and motivation for continued engagement.
Desired exercise types
Participants emphasised the need to tailor exercises to address the specific challenges associated with MS. They valued group-based exercise for the social interactions, consistency, shared learning and enjoyment it provides. Participants expressed a desire for activities that develop coordination, balance, strength, endurance, fine motor skills, flexibility, breathing, mobility and dance. They also requested sensory perception training and guidance for resuming exercise after a relapse. Furthermore, participants highlighted the importance of practical exercises that relate to daily life, such as those mimicking household tasks like vacuuming and cooking.
Preferred exercise programme design
Participants noted that a successful exercise programme requires clear communication and gradual progression to maintain motivation while preventing fatigue and injury. They appreciated consistent routines with challenges appropriate for various performance levels, emphasising the need for adaptability to individual needs and goals. The inclusion of different difficulty levels and progression encouraged their engagement, allowing them to adjust for changes in physical abilities. Participants valued a simple structure with brief explanations that facilitated easy implementation into daily routines, along with exercises designed to improve adherence. Clear, effective instructions, communication and guidance were also preferred by participants to enhance engagement and motivation. Participants stressed the importance of proper execution and preventive guidance, appreciating the ability to select exercises that matched their capabilities. Knowing the difficulty of exercises in advance and receiving initial information on duration helped them manage their time and energy efficiently, while short instructional videos facilitated understanding and execution.
Expert-led and personalised evaluation and exercises
Participants preferred exercise video presenters who are friendly and positive, as this fosters a supportive and motivating environment. They value expert guidance from specialists, such as neurologists and physiotherapists, for precise recommendations. Real-time interaction and personalised feedback from physiotherapists during sessions are also desired to enhance engagement. Participants emphasised the importance of presenters with expert knowledge for accurate demonstrations. Some suggested that presenters with MS could offer relatable guidance and inspiration, fostering a sense of community.
Theme 3: autonomy
Exercise environment and regimen parameters
Participants emphasised the importance of accessible exercise spaces, highlighting good lighting, uncluttered areas and supportive furnishings. They stressed the need for readily available equipment and using common objects like water bottles instead of traditional dumbbells to enhance practicality. Participants preferred a comfortable home environment with a neutral background to maintain focus during sessions. They discussed the significance of visual design elements, such as subtitles, close-up movements and consistent camera angles, to improve accessibility. To determine the length of the planned programme, participants were asked about their current exercise intensity and frequency. Reported session durations varied widely, ranging from 10 to 60 min, depending on individual endurance and health status. Participants suggested a programme of around 1–5 hours per week, tailored to the effectiveness and endurance of pwMS. They also noted the need for a balance between exercise intensity and necessary recovery time to optimise results. Additionally, participants advocated for incorporating visual timers and clear instructions to facilitate effective time management based on individual physical capabilities.
Adressing diverse symptoms and needs in pwMS
Participants emphasised the need for an inclusive and adaptable exercise programme that accommodates the diverse needs of pwMS, including those with significant mobility limitations such as wheelchair users. They highlighted the importance of consulting neurologists and specialised physiotherapists for specific needs, such as pelvic floor exercises, to ensure exercises are effective. They stressed the importance of support for individuals who may need assistance with starting positions, reaching objects and engaging with exercise videos. Additionally, participants suggested accounting for specific symptoms like heat sensitivity and fatigue, advocating for fatigue management techniques such as fatigue diaries and activity planning to help maintain energy levels during exercise. Addressing additional symptoms, such as incontinence and eye movement disorders, was perceived as crucial for effective exercise planning and implementation. Participants also underscored the significance of monitoring individual responses to exercise, allowing for adjustments based on symptoms like fatigue, dizziness or pain.
Theme 3: autonomy
Utilisation and accessibility of technology and digital resources for exercise
Participants emphasised the necessity of universally accessible exercise programmes to reach a diverse MS community effectively. The programme should integrate technical solutions, effective visual design, subtitles and clear communication to enhance accessibility for pwMS. They highlighted the importance of accessing exercise videos on various devices—such as TV, laptop, tablet and phone—to integrate physical activity into their daily routines seamlessly. Digital resources, including apps and online videos, play a vital role in personalising exercise programmes for pwMS. They noted that integrating apps into physiotherapy facilitates the creation of tailored plans based on individual health status and progress. Many valued fitness apps that offer clear structure, search functions and the flexibility to exercise in various locations. However, they expressed a strong preference for a mobile application specifically designed for pwMS, citing its potential as a personalised and convenient tool for engaging with tailored exercise programmes. Participants also appreciated YouTube as an accessible platform for exercise programmes, allowing pwMS to engage with content from home. While YouTube is a valuable resource for discovering exercises, some were concerned that certain content may not meet their specific needs.
Ensuring safety in exercise
Health professionals recommended regular health assessments, such as cardiovascular screenings before starting exercise, to confirm the medical suitability of workout routines. Participants stressed that safety is crucial, highlighting the need for exercise videos to provide clear instructions to ensure safe practices, including risk articulation and demonstrations with assistive devices such as wheelchairs or walking aids. They also underscored the importance of safe, obstacle-free environments with secure support options. Practical safety tips included using stable furniture for balance or wearing appropriate footwear.
Empowering personal choice and self-directed participation in exercise
Participants emphasised the importance of autonomy in their exercise routines, with maintaining or regaining workability as a key motivator for engaging in music-based exercise. Exercising in a safe environment while pushing beyond their comfort zone helped them maintain independence. Participants stressed that understanding safety risks and taking personal responsibility for recognising limits are crucial for preventing falls and ensuring safety. They valued instructional videos that reinforced these principles, considering them essential for promoting safe, effective exercising and supporting independence and self-efficacy. They preferred to exercise at their own pace, with personal music choices enhancing their sense of control and autonomy.
Theme 4: musical meaning
Integration of music in exercise
Participants’ enjoyment and engagement in music-assisted exercise programmes were influenced by their preferences for specific genres and elements such as beat, instruments and melodies. Energetic music was favoured for strength training to enhance motivation and focus, while calming music was preferred for relaxation exercises to facilitate recovery. They recommended including a variety of music styles to cater to different tastes and providing playlists or music libraries to enhance the experience and personalisation. Additionally, they suggested specifying beats per minute to align their favourite songs with the programme’s timing. Some participants emphasised the need for a balanced acoustic environment in exercise videos to ensure that instructions are not overshadowed by background music. They noted that changes in music volume could impact exercise performance, emotions and the ability to accurately follow cues.
Cultural and individual influences on exercise music
Participants emphasised the importance of considering cultural backgrounds in music selection to accommodate diverse preferences and rhythmic abilities. While some prefer exercising without music based on their daily conditions, others face challenges with impaired rhythm perception, complicating the synchronisation of movements to music. There was a strong desire among participants to link physical movements to cognitive aspects of music, such as rhythm and lyrics, to enhance their engagement with the exercise. Music therapists noted the stimulating effect of pitch and tempo, particularly for those with impairments, for example, different sound frequencies for pwMS with hearing loss. For relaxation activities, nature sounds and diverse auditory elements beyond traditional music were suggested.
Musical elements in exercise
Participants highlighted that music volume significantly affects their bodily movements and emotions, with soft and loud music creating different experiences. They found that the beat serves as an essential temporal structure, providing rhythmic-auditory cues that aid in movement synchronisation. Most participants reported that songs with a steady, consistent rhythm are easier to follow, enhancing their ability to align physical activity with the music. The instrumentation was also deemed important, as it should complement exercise movements. Additionally, tempo impacts the flow of movement and synchronisation. Some participants reported improved exercise routines by syncing their movements with the music’s rhythm, leveraging cognitive aspects like rhythm perception. This synchronisation enhanced motor coordination and exercise effectiveness, with therapists noting the influence of tempo on movement flow. Specifically, tailored chords or rhythmic elements for exercises targeting the feet, arms or core allowed participants to anticipate subsequent movements, improving recall and engagement.
The motivational impact of music on exercise
Participants valued the benefits of music in exercise, including motivation, pacing and support for relaxation. They recognised the emotional impact of music during workouts, emphasising the personal connections individuals form with it. Participants stressed the importance of enjoyable music for increasing adherence to therapeutic exercises, noting that it enhances the overall experience by making movement easier and more engaging. They acknowledged that musical taste is subjective and can vary with mood, highlighting the dynamic nature of individual preferences. The tempo and rhythm of music were noted to influence exercise pace and help maintain a steady rhythm, which is especially beneficial for coordination and balance. Music also served as a distraction from fatigue or discomfort, enabling people with MS to exercise longer or with greater intensity. Overall, participants reported a positive synergy between exercise and music, enriching their routines.
Integration of findings
Integration of qualitative and quantitative data was performed by four researchers (BF, IH, SM, BS) and was understood as a specific interaction between two or more methods, where each method maintains its own paradigmatic characteristics but is interwoven with others to enhance understanding.64 This integration involved qualitative and quantitative methods and data types, which were aligned with common research questions for their implementation. Consequently, they became necessarily interdependent while preserving their unique paradigmatic forms. confirming the success of PPI activities: (a) 144 co-created music-supported exercise videos for pwMS with mild to severe disability are freely available and feature GEMA-free music on the Tyrolean MS Society homepage (https://msgt.at/index.php/uebungen.html); (b) four of the 148 videos include general information presented in an expert interview format, and 144 of them contain exercise instructions in appropriate language; (c) using interviews and focus groups, participants evaluated the videos as relevant, feasible and usable; (d) additionally, predefined exercises in the ‘easy’ category (seated or lying body position) are suitable for severely affected pwMS; (e) stakeholders expressed that they felt included, respected and listened to, as reflected by the quantitative PPI assessments conducted during visits 1–8, which involved stakeholders only, presented in table 4.
Stakeholders’ ratings of levels of involvement, MS-related self-efficacy and emotional states of pleasure, arousal and dominance across visits 1–8
Impact of PPI
Early involvement of pwMS and family members as stakeholders elevated project quality, addressing errors and providing innovative ideas. Their lived experience challenged our traditional views, identifying essential elements, preferences and constraints early on. They corrected inappropriate language and influenced exercise selection for severely impaired pwMS. Feedback on music and exercises shaped the project, with most pwMS finding music motivating. Stakeholders felt respected as individuals, transforming our perspective on our work. Context factors that facilitated the PPI process included the involvement of pwMS, including MS support group leaders/members and patient representatives and their family members, as well as MS medical and rehabilitation specialists, and the neurology departments at two medical centres.
Discussion
This participatory mixed methods study involved pwMS in developing a music-supported exercise programme. Factors that facilitated the PPI process included the participation of pwMS, comprising MS support group leaders/members and patient representatives, and their family members, as well as MS medical and rehabilitation specialists, working at the neurology departments of two medical centres. Involving pwMS early as stakeholders enhanced the project’s quality, corroborating findings from a recent study.65 Stakeholders’ experiences brought valuable insights, challenging our perspectives and shaping our approach. This led to a transformative focus on tailored solutions for different needs, fostering mutual support and emphasising shared decision-making and face-to-face discussions, aligning with key PPI principles.66
Stakeholders’ feedback on combining music with exercise had a significant impact on the project. PwMS found the music motivating, seeing it as inspiring rather than just functional. This perspective shift emphasised valuing individuals beyond their condition, transforming our outlook on the project. Research shows most pwMS do not exercise sufficiently for health benefit.12 13 Maintaining mobility, managing external perceptions, mitigating potential employer impacts and preserving family functionality amid responsibilities and financial pressures were common motivators. These findings align with similar studies.67 There is limited literature on mixed methods intervention development using participatory design in pwMS. One study developed a digital toolkit for an evidence-based fatigue management programme to reduce fatigue and enhance QoL, emphasising pwMS’ participation throughout the development cycle for MS-centred solutions.68 Our study’s findings also align with a systematic review that highlighted the benefits of co-design methodologies, especially those based on lived experiences, for researchers designing interventions for patients after stroke. Involving patients and clinicians helped researchers understand their needs and prioritise solutions.69
Theme 1 (engagement) highlights the critical role of music-supported exercise programmes in improving physical ability and emotional well-being. Participants in our study perceived that music-supported exercises designed for pwMS were highly motivating. These findings align with research showing that music in exercise enhances enjoyment, improves quality of life and lowers perceived exertion in neurological conditions.70–72 Gamification and goal-setting were identified as key motivators, reflecting research demonstrating their effectiveness in enhancing engagement and self-efficacy in rehabilitation settings.73 74 Participants also valued adaptable programmes and expert guidance from physiotherapists, emphasising the need for professional demonstrations, which aligns with findings from systematic reviews that knowledgeable guidance supports effective exercise in pwMS.70
Theme 2 (ease) emphasises the importance of accessibility and adaptability in exercise programmes for pwMS. Participants highlighted the need for accessible, flexible and symptom-responsive programmes, including provisions for wheelchair users, ensuring usability for those who are more severely affected. They also preferred using common objects, such as water bottles, instead of traditional dumbbells to enhance practicality. This aligns with studies showing a preference for challenging, enjoyable exercises that require minimal equipment.72 Participants stressed the importance of practical spaces with good lighting and neutral backgrounds to improve focus and engagement, consistent with evidence that well-designed environments enhance adherence and reduce barriers to participation.75 76 Additionally, they emphasised the need to monitor individual responses, such as fatigue and pain, and to adjust programmes accordingly. Recent findings further suggest that transitioning from staff-supported to self-guided exercises will be key to future interventions.70 71 76
Theme 3 (autonomy) highlights the importance of autonomy and safety in exercise programmes for pwMS. Participants emphasised the need for accessible digital tools, such as apps and videos, which can be used across multiple devices. They valued apps specifically designed for pwMS, which supports evidence that increased autonomy improves motivation and adherence to physical activity.77 The participants’ preference for personalised, self-directed exercises is consistent with evidence that such programmes can improve adherence and motivation in pwMS.77 Personalised features, including tailored exercises for different mobility levels and the ability to adjust intensity and duration, were regarded as crucial for maintaining autonomy. Safety was a key concern, with both participants and health professionals stressing the importance of health assessments, professional guidance during relapses and safe exercise environments to prevent injury. These findings align with previous research on the necessity of disability-specific content in exercise programmes.72
Theme 4 (musical meaning) explores the integration of music into exercise programmes for pwMS, highlighting its role in enhancing enjoyment, motivation and engagement in exercise. Participants and music therapists emphasised the importance of personalised music options, recommending a variety of genres and the ability to customise beats per minute to align with their workout routines. Cultural and individual influences were significant, with participants stressing the need for music that accommodates diverse preferences and rhythmic abilities. Some participants reported challenges with rhythm perception, which complicated movement synchronisation, while others highlighted the cognitive benefits of linking musical elements, such as rhythm and lyrics, to physical movements. The latter is supported by research demonstrating the efficacy of rhythm and tempo in improving motor control in patients with neurological conditions.78 Various studies have shown the effectiveness of music-based exercises in pwMS,23 patients after stroke79 and with PD.80 In our study, the emotional connections participants formed with music were described as crucial for enhancing the overall exercise experience. These findings correspond with a study involving people with PD, showing music’s benefits for cognition, mood, motivation and movement synchronisation.81
Integration of the qualitative and quantitative components showed that the PPI activities were successful, resulting in the creation of 148 freely available music-supported exercise and information videos suitable for pwMS with mild to severe disability. These videos were evaluated as relevant, feasible and usable by pwMS. Importantly, stakeholders felt included, respected, listened to and reported high levels of pleasure and increasing dominance throughout the process, with high levels of involvement. We find it essential to regularly gather feedback from stakeholders about their involvement levels. As supported by a systematic review,69 assessing the effectiveness of co-production processes is crucial for making necessary adjustments.
Future development suggestions for the music-supported exercise programme include integrating it into a dedicated mobile app for pwMS and incorporating group exercise activities. Additionally, it is recommended to provide options for personalised music selection and improve accessibility for pwMS with visual, hearing or cognitive impairments. The programme should offer customisable exercises and remote supervisory support from physiotherapists for enhanced personalisation. After these enhancements, conducting a rigorous evaluation through a randomised controlled trial is crucial.
While our study has strengths, it is important to acknowledge its limitations. First, due to the limited study timeframe, safety, feasibility and effectiveness of the co-created music-supported exercise programme were not assessed. Second, the programme, while diverse, can be expanded for comprehensiveness. Third, to improve long-term adherence, offering personalised music selection is crucial. Budget constraints allowed us to provide the programme for free with GEMA-free music, limiting memorability and emotional connections. Fourth, co-researchers who conducted the interviews also performed the initial data analysis, while researchers responsible for the thematic analysis were involved in the study design, potentially introducing bias in data interpretation. Fifth, while focus groups typically consist of five to eight participants, the unpredictable nature of MS symptoms led to short-term cancellations, and in our study, three focus groups consisted of only three or four participants to maintain participant engagement. However, ‘mini focus groups’ (two to four participants) are increasingly used in qualitative research due to their advantages in accommodating specific needs, aligning with the principles of PPI.82–84 Sixth, participants’ quotes in German could not be directly included in this article. However, the researchers translated the quotes into English, and a bilingual native English speaker reviewed and refined the translations.
Conclusions
This participatory mixed methods study involved pwMS in developing a music-supported exercise programme, enhancing project quality. Stakeholders’ experiences shaped our focus on specific needs like intensity, cognition and preferences for severely affected individuals. Key PPI principles of sharing, listening, responding and partnership were emphasised, fostering trust and transparency. The successful PPI activities led to the creation of 148 accessible videos suitable for pwMS, positively received and enjoyable, with stakeholders feeling respected and involved throughout.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the research ethics committees of the Medical Universities of Innsbruck (ref. 1424/2021; 10 February 2022) and Vienna, Austria (ref. 2210/2021; 4 February 2022; amendment 8 September 2024). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to warmly thank our stakeholders Marina Trixl, DI Brigitte Zauner, Karin Kollmaier, Eva Ehrenleitner, Martin Gabl, DI Harald Spicka, Margit Kiesler, Michaela Bauer, Eva Csida, Beatrix Waltner, Elisabeth Bauhofer, Mag. Nadja Hofer, Julia Thummerer, Mag. Melanie Hie, Natascha Eder, Mag. Barbara Fröwis, Carmen Eder, the MS support groups Kitzbühel and Kunterbunt Vienna, the Multiple Sclerosis Societies Tyrol, Vienna and Austria and all pwMS who participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors BF and BS obtained funding. BF and BS conceived and designed the study. BF, TM, SM, FF, IH, NL, FL, CB and BS were involved in co-researcher and participant recruitment. Co-researcher workshops and the co-creation process were facilitated by BF, SM, FF, IH, NL and BS. Data collection was performed by BF, SM, FF, IH, NL, TM, FL, CB and BS. Data analysis was conducted in collaboration with stakeholders by BF, SM, IH, NL, FF and BS. BF and BS drafted the initial manuscript. All other authors provided input to subsequent manuscript drafts and critically revised the article for important intellectual content. All authors approved the final version of the article to be published. BS accepts full responsibility for the finished work and/or the conduct of the study, had access to the data and controlled the decision to publish. BS is the guarantor.
Funding This study was funded by the Ludwig Boltzmann Gesellschaft, Open Innovation in Science Center, Vienna, Austrian MS Research Society and ÖMSG gemeinnützige Privatstiftung.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the 'Methods' section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.