Article Text

Abstract
Introduction The elderly population is more vulnerable to traumatic brain injury (TBI) compared with younger adults, and there is an increasing trend in TBI-related hospitalisations and deaths in the elderly due to the ageing global population. This is a thorough update to a previous meta-analysis on the mortality of elderly TBI patients. Our review will include more recent studies and provide a comprehensive analysis of risk factors.
Methods and analysis The protocol of our systematic review and meta-analysis is reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols guidelines. We will search the following databases: PubMed, Cochrane Library and Embase from inception to 1 February 2023 reporting in-hospital mortality and/or risk factors predicting in-hospital mortality among elderly patients with TBI. We will perform a quantitative synthesis for in-hospital mortality data combined with meta-regression and subgroup analysis to determine whether there is a trend or source of heterogeneity. Pooled estimates for risk factors will be presented in the form of ORs and 95% CIs. Examples of risk factors include age, gender, cause of injury, severity of injury, neurosurgical intervention and preinjury antithrombotic therapy. Dose–response meta-analysis for age and risk of in-hospital mortality will be performed if sufficient studies are included. We will perform a narrative analysis if quantitative synthesis is not appropriate.
Ethics and dissemination Ethics approval is not required; we will publish findings from this study in a peer-reviewed journal and present results at national and international conferences. This study will promote a better understanding and management of elderly/geriatric TBI.
PROSPERO registration number CRD42022323231.
- neurosurgery
- geriatric medicine
- trauma management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This is the first study specifically designed to investigate risk factors associated with the outcome of geriatric traumatic brain injury.
The study will introduce various analysis methods such as meta-regression, subgroup analysis and dose–response meta-analysis.
We will use the Newcastle-Ottawa Scale to assess the risk of bias in the included studies.
One possible limitation could be the comprehensiveness in the analysis of all risk factors in the elderly traumatic brain injury population.
Introduction
Background
Traumatic brain injury (TBI) is a significant health burden and one of the leading causes of death worldwide.1–4 It is estimated that there are 54–60 million new TBI cases every year globally,2 5 and in Europe, every TBI death has been associated with an average of 24.3 years of life lost.6
Population ageing has been a major health concern in high-income countries and continues to be a progressive issue in the rest of the world. According to the United Nations, the number of persons aged 65 years or over-reached 703 million in 2019 and is expected to double to 1.5 billion by 2050, accounting for 16% of the global population.7 As the largest developing country in the world, China has a population of 1.4 billion, including 191 million older adults according to the seventh National Census in 2020, however, the United Nations expects this number to reach 366 million by 2050, taking up 26.1% of the total population compared with 13.5% currently.7 8
Similarly, a trend is also observed in annual TBI-related hospitalisations and deaths with the number of elderly/geriatric patients increasing and the number of younger patients decreasing.9–12 Meanwhile, elderly patients are more likely to suffer from TBI. Individuals aged 65 years or over-represented 15.2% of the US population in 2017,13 but they accounted for 43.9% of all TBI-related hospitalisations and 38.4% of all TBI-related deaths in the USA in 2017.14
The major cause of geriatric TBI is falls, followed by road traffic accidents.15–18 Elderly TBI patients tend to have a higher chance of mortality and poorer functional outcomes than younger patients.19–23 Many factors have been reported to be associated with in-hospital mortality in geriatric TBI patients, including older age,16 18 24 25 gender16 25 26 and severity of injury.16 17 25 Some factors remain debatable when it comes to their effects on outcomes of geriatric TBI, such as causes of injury,16 18 27 neurosurgical intervention17 25 28 and preinjury antithrombotic therapy.15 29 30
Previously, there have been several meta-analysis studies on geriatric TBI, with some describing short-term and long-term functional conditions.26 31 32 One study compared the effect of two anticoagulants on geriatric patients with mTBI.33 A meta-analysis published in 2013 examined 22 studies on mortality at 5 time points post-TBI, including 11 studies that focused on mortality at discharge.34 With respect to this previous study by McIntyre et al, we will include a much larger number of recent studies, and introduce new analysis methods such as meta-regression and dose–response meta-analysis as updates that were not used in this previous meta-analysis. Furthermore, the main aim of our study will be to provide a comprehensive analysis of risk factors predicting in-hospital mortality.
Objectives
This systematic review aims to examine the in-hospital mortality rate of TBI in elderly patients and to evaluate the risk factors predicting in-hospital mortality. We seek to answer the following questions:
What is the overall in-hospital mortality rate among elderly patients with TBI, and what is the in-hospital mortality rate when TBI is classified as mild (GCS 13–15), moderate (GCS 9–12), severe (GCS 3–8) or critical (GCS 3–5)?
Is there a trend in the in-hospital mortality rate over time or in different regions of the world?
What are the risk factors for in-hospital mortality among elderly patients with TBI, and to what extent can these predict the in-hospital mortality of our study population?
Methods
Study registration
The protocol of our systematic review and meta-analysis is reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) statement guidelines.35 This protocol was registered on the PROSPERO database (CRD42022323231) on 12 May 2022.
Eligibility criteria
Types of studies
Retrospective or prospective cohort studies, case–control studies and cross-sectional studies will be included.
Study population
This systematic review is focused on elderly patients with TBI. ‘Elderly’ was defined by the United Nations36 and the WHO37 as adults aged ≥60 years, it is also often defined elsewhere as ≥65 years.7 To include more studies, we will use the more inclusive criterion of adults ≥50 years in our study screening process. Due to possible variations in disease diagnosis, the definition of ‘TBI’ will be extracted from included studies.
Exposure
We will investigate risk factors reportedly associated with the in-hospital mortality of our study population, and we will assess to what extent these risk factors can predict our primary outcome. Specific examples of risk factors include age, gender, cause of injury, severity of injury, neurosurgical intervention, preinjury antithrombotic therapy, etc.
Outcomes
The primary outcome is in-hospital mortality (mortality at any time point within 30 days is also considered in-hospital mortality). Additional outcomes are risk factors predicting main outcomes, which will be measured and analysed in the form of ORs.
Search strategies
The searches will be conducted in the following three databases under the guidance of the Cochrane Handbook:38 PubMed, Cochrane Library and Embase from inception to 1 February 2023. We will include studies published in English only. Table 1 presents the initial draft of the search strategy to be used for the PubMed database. The detailed search strategy for all three databases can be found in online supplemental material.
Supplemental material
Search strategy for PubMed
Inclusion criteria
Studies that provide outcome information for elderly patients diagnosed with TBI.
Studies that reported risk factors predicting the main outcome for elderly patients diagnosed with TBI.
Exclusion criteria
Studies in languages other than English.
Studies that use a different outcome measure other than in-hospital mortality or mortality within 30 days, such as 6-month mortality or functional outcome.
Studies that only focused on one specific type of TBI, such as ‘acute subdural haematoma’.
Studies that did not provide specific data for the elderly group or provided data that is hard to extract (eg, provided by line charts).
Studies with a small sample size (elderly group N<100 for overall mortality analysis, or N<20 for severity subgroup analysis).
The study screening process will be conducted by two independent investigators. The first round of screening will be conducted by reviewing the titles and abstracts of all studies obtained through database searches, to evaluate all studies that meet the inclusion criteria. The full-text articles and possible appendixes of available studies will then be reviewed to exclude studies that meet the exclusion criteria. The reasons for exclusion will be recorded. All discrepancies will be resolved by consultation with a third investigator.
For studies that share the same data source, we will only include the study with the larger sample size and longer study period in the mortality analysis, and the study containing more data on risk factors will be included in the analyses of risk factors.
Data extraction
Data extraction will be performed by two investigators and will include the following information: (1) author(s) of the study; (2) research time period and publication year; (3) study design; (4) country and continent of the study; (5) data source; (6) study population and inclusion criteria; (7) definition of ‘elderly’ and diagnostic criteria for ‘TBI’; (8) main outcome; (9) number of patients included in the elderly group; (10) mortality observed in the elderly group; (11) risk factors predicting main outcomes (if reported) and (12) ORs and 95% CIs of the risk factors (data from multivariate regression analyses are preferred).
All disagreements will be resolved by consultation with a third investigator.
Risk of bias and quality assessment
Risk of bias assessment of included studies will be performed by two investigators independently using the Newcastle-Ottawa Quality Assessment tool for cohort studies and case–control studies,39 based on selection, comparability and outcome. A third investigator will be consulted should there be any disagreement. A rate of <20% lost to follow-up is considered as low risk of bias due to incomplete data. Publication bias will be assessed by the funnel plot, Egger’s test and Begger’s test for every synthesis of four studies or more. Sensitivity analysis will be performed for overall mortality by excluding one study at a time or excluding studies with low Newcastle-Ottawa Scale scores. A summary table of study characteristics will be presented, including the study population, study setup, study design and definitions of ‘elderly’ and ‘TBI’.
Strategy for data synthesis
The PRISMA flow chart will be used to present the selection process. Extracted data will be imported into Stata 17.0 (Stata, College Station, TX) for all analyses. For each of the studies included in the mortality analysis, extracted mortality rate values will be either reported by studies or calculated from accessible original data. Figure 1 summarises the study design and main methodological aspects of this study.

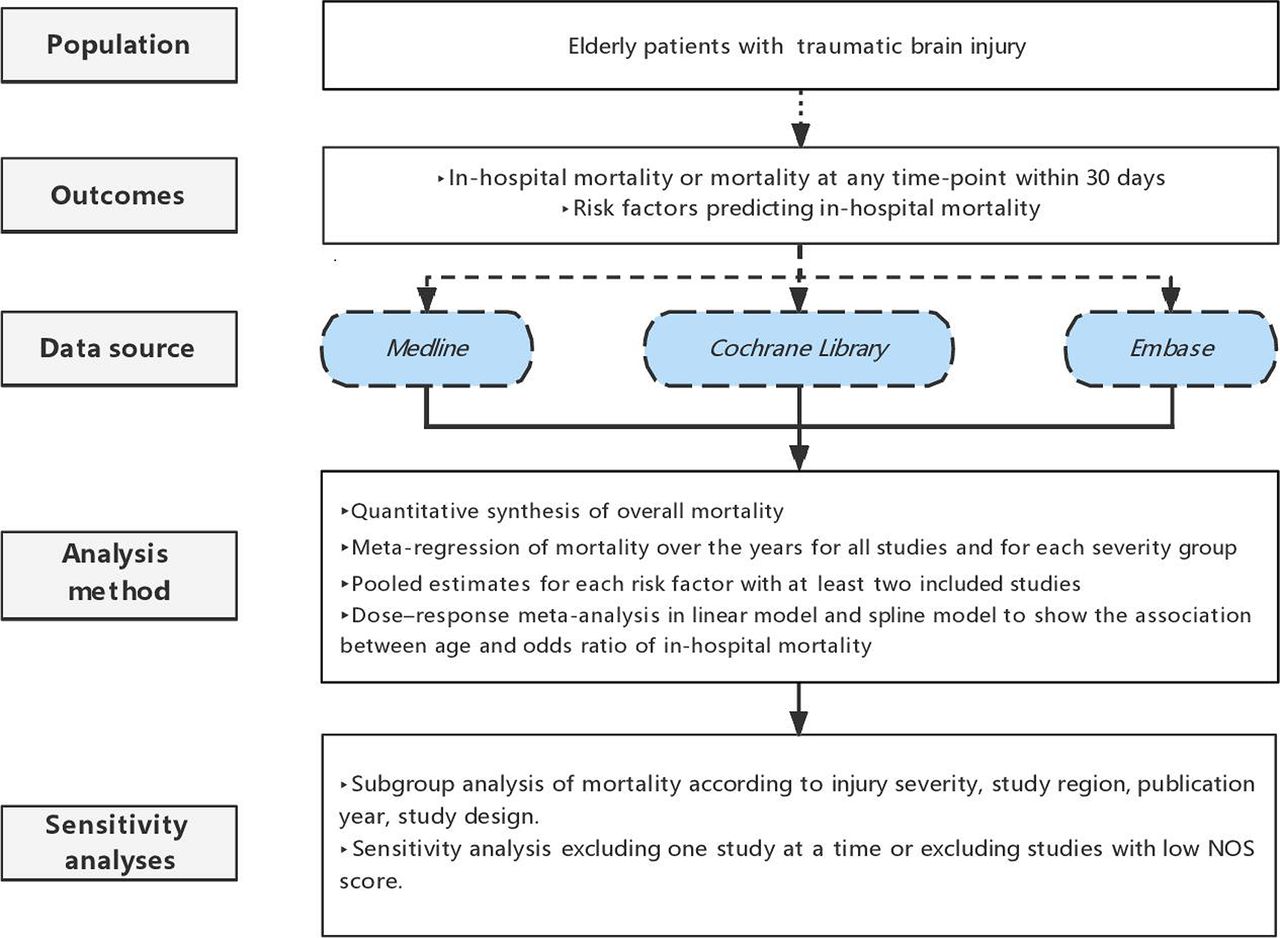{kind=link}
Summary of the study design and main methodological aspects. NOS, Newcastle-Ottawa Scale.
Between-study heterogeneity will be assessed using the I² statistic, and heterogeneity of I²>50% will be considered significant.40 For overall mortality synthesis, we will use a fixed-effect model, and a random-effects model if there is significant between-study heterogeneity. Subgroup analysis will be performed according to injury severity, study region, publication year and study design to determine the potential source of heterogeneity. Meta-regression will be used to assess the trend in mortality over time for all studies and for each severity group.
For risk factors analysis, we will categorise the risk factors predicting the main outcome reported, and if there are more than two eligible studies included for a certain risk factor, synthesis of effect size will be conducted using ORs and 95% CIs reported in these studies or calculated from original data. For the risk factor of age, we will compare the OR of the oldest age group (eg, 90+ years) to that of the youngest age group (eg, 60–69 years). In addition, if there are more than five studies reporting in-hospital mortality rate data for at least three age groups, a dose–response meta-analysis will be conducted in a linear model and spline model to better show the association between age and risk of in-hospital mortality.41
We will perform a narrative analysis when quantitative synthesis is not appropriate.
Grading the quality of evidence
The quality of evidence for all outcomes will be judged using the Grading of Recommendations Assessment, Development and Evaluation working group methodology. The quality of evidence will be assessed across the domains of risk of bias, consistency, directness, precision and publication bias. Additional domains may be considered where appropriate. Quality will be adjudicated as high, moderate, low or very low.
Patient and public involvement
None
Discussion
Despite the health burden associated with geriatric TBIs, there are very few high-quality guidelines on the management of elderly TBI patients.42 This area, therefore, demands more attention and study. With the results of our systematic review and meta-analysis, we will be able to understand the current situation, time-related or region-related trend of geriatric TBI on a large scale.
In the first part of our work, we will reexamine the pooled in-hospital mortality rate of elderly TBI patients, as an update and expand to the previous meta-analysis.31 We will include much more studies published recently through our comprehensive search, and introduce new analysis methods such as meta-regression and subgroup analysis.
The main strength of our study lies in the comprehensive analysis of risk factors and our methodology approaches. We will provide quantified analysis and narrative analysis to identify all the risk factors, and introduce dose–response analysis to show the risk of older age. This has not been conducted by any other meta-analysis, which could strengthen our knowledge of some well-established risk factors, and determine the effect of some previously debatable factors. This part of our work can help identify the high-risk groups among geriatric TBI patients, and provide evidence or direction for developing a prognosis model. The final purpose is the targeted allocation of medical resources to the most beneficial patients.
One of the main possible limitations of our systematic review and meta-analysis could be the scarcity of studies and data on some of the risk factors in the elderly TBI population, for most of the studies focusing on patients of all ages, and our conclusion on these risk factors could be biased by the small sample size.
We hope that our study can answer some important clinical questions and provide useful information for clinicians, researchers, policy makers and eventually promote better understanding and management of geriatric TBI.
As a summary of the highlight, this study will provide comprehensive quantified analysis and narrative analysis to identify in-hospital mortality and the risk factors of geriatric TBI, and introduce dose–response analysis to show the risk of older age.
Ethics and dissemination
Ethics approval is not required. We will publish findings from this study in a peer-reviewed journal and present results at national and international conferences.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
ZM and JH are joint first authors.
ZM and JH contributed equally.
Contributors JF is the guarantor. JH developed the search strategy. CY developed the risk of bias assessment strategy. ZM drafted the manuscript. LX, JF and JJ helped to revise the manuscript. LX provided statistical expertise and developed the meta-analytic strategy. All authors read and approved the final manuscript.
Funding This study is funded by the Program of Shanghai Academic/Technology Research Leader (21XD1422400) and the Project of Shanghai Medical And Health Development Foundation (20224Z0012).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.