Article Text

Abstract
Objectives To systematically estimate the prevalence and influencing factors of fear of disease progression (FoP) in patients who had a stroke, with a focus on China.
Design Systematic review and meta-analysis of observational clinical studies.
Data sources Eight databases (China National Knowledge Infrastructure, Wanfang Database, Chinese Scientific Journal Database (VIP), CBM, Web of Science, PubMed, Cochrane Library, Embase) were searched from inception to March 2024, supplemented by manual reference screening.
Eligibility criteria Cross-sectional studies reporting FoP incidence or influencing factors in Chinese stroke patients using the Fear of Progression Questionnaire-Short Form scale were included.
Data extraction and synthesis Two reviewers independently screened studies, extracted data and assessed study quality using the Agency for Healthcare Research and Quality tool (score range: 0–11 points). Random-effects models were applied to address substantial heterogeneity. Stata 17.0 software was used for meta-analysis.
Results A total of 20 studies (15 medium-quality, 5 high-quality) involving 7156 patients were included. The pooled incidence of FoP in Chinese stroke patients was 56% (95% CI=45% to 66%), derived from a random-effects model despite significant between-study heterogeneity (I²= 98.7%), with subgroup analyses and leave-one-out sensitivity analysis confirming result robustness. Subgroup analysis revealed that the incidence was highest in East China (70%, 95% CI=56% to 83%), followed by Central China (55%, 95% CI=36% to 73%) and North China (43%, 95% CI=38% to 47%). The incidence of FoP in haemorrhagic stroke (72%, 95% CI=49% to 95%) was higher than that in ischaemic stroke (45%, 95% CI=27% to 64%). The incidence of FoP after 2020 (59%, 95% CI=48% to 70%) was higher than that before 2020 (40%, 95% CI=32% to 47%). Meta-regression identified publication year (p=0.004) and research region (p=0.001) as key heterogeneity sources. The main influencing factors of FoP in Chinese stroke patients included age (OR=0.94, 95% CI=0.92 to 0.97, p<0.05), education level (OR=0.71, 95% CI=0.67 to 0.76, p<0.05), economic income (OR=0.74, 95% CI=0.69 to 0.78, p<0.05), body mass index (OR=1.22, 95% CI=1.04 to 1.43, p<0.05), social support (OR=0.75, 95% CI=0.63 to 0.90, p<0.05), illness perception (OR=1.41, 95% CI=1.37 to 1.45, p<0.05) and family intimacy (OR=0.80, 95% CI=0.67 to 0.96, p<0.05). No significant publication bias was detected (Egger’s p=0.052, Begg’s p=0.444), though funnel plot asymmetry suggested potential heterogeneity effects.
Conclusion The incidence of FoP in Chinese stroke patients is high (56%), influenced by age, education level, economic income, body mass index, social support, illness perception and family intimacy. Despite high heterogeneity, sensitivity analyses confirmed result robustness. Clinical staff should prioritise psychological screening for FoP and implement targeted interventions, such as cognitive–behavioural therapy for negative illness perception, social support programmes for low-income patients and family-centred education for younger patients.
PROSPERO registration number CRD42024522147.
- Stroke
- Meta-Analysis
- Patients
- Nursing Care
- Systematic Review
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The meta-analysis followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines with a comprehensive search across eight databases and manual reference tracking, minimising selection bias.
Two independent reviewers conducted study screening, data extraction and quality assessment using the Agency for Healthcare Research and Quality tool, enhancing methodological rigour.
Subgroup analyses and sensitivity tests were performed to address heterogeneity.
The small number of studies (n=20) limited subgroup analyses for some influencing factors, reducing statistical power.
Non-Chinese studies were excluded, potentially omitting unpublished data and limiting generalisability to non-Chinese populations.
Introduction
Stroke is currently the second leading cause of death globally and the leading cause of adult death and disability in China. By 2020, there were 17.8 million stroke patients in China over the age of 40,1 2 and the 5-year recurrence rate in this population is as high as 41%.3 Additionally, 70–80% of these patients will experience residual disabilities after treatment.4 Stroke patients often suffer from negative emotions such as anxiety and depression due to the long-term and repeated impacts of the disease on their body and mind. Furthermore, patients may experience fear due to a lack of understanding of the disease and uncertainty about its treatment and prognosis.5 Fear of progression (FoP) is the fear patients experience concerning the disease’s consequences or recurrence,6 and extends beyond transient psychological distress to critically impair treatment adherence, health behaviours and rehabilitation outcomes.7 8 Therefore, understanding the incidence and influencing factors of FoP in stroke patients is crucial for early identification and management of their fears.
Emerging evidence highlights the global prevalence and clinical significance of FoP in stroke populations. A UK qualitative study revealed that 56% of stroke survivors experience clinically significant FoP, primarily driven by uncertainty about functional recovery and social role disruption.9 Crowe et al10 further demonstrated that stroke’s sudden onset and chronicity foster profound self-worth loss and persistent fear of recurrence, severely compromising quality of life. Consistent with these findings, a Korean survey of 180 ischaemic stroke patients11 identified elevated FoP levels associated with inadequate disease knowledge and maladaptive health behaviours (eg, poor dietary habits, exercise avoidance and medication non-adherence).
Despite these insights, critical gaps persist in understanding FoP among Chinese stroke patients. Current research predominantly focuses on Western and other Asian populations, with limited investigation into China’s unique sociocultural context where family-centred care models and stigma surrounding chronic illness may amplify FoP.12 13 No consensus exists regarding FoP incidence or modifiable risk factors in this population, hindering the development of culturally adapted interventions. Thus, this study uses meta-analysis to explore the incidence and influencing factors of FoP in Chinese stroke patients, aiming to provide evidence-based guidance for clinical staff to identify high-risk patients early and develop targeted, individualised intervention programmes.
Methods
Database and search strategies
Computer retrieval of data was conducted using CNKI, Wangfang database, VIP, CBM, Web of Science, PubMed, the Cochrane Library and Embase—eight major databases. The search targeted literature on the incidence of FoP in stroke patients and/or related influencing factors, with a retrieval time limit up to March 2024. A combination of Medical Subject Heading terms and free text words was used: “stroke”, “apoplexy”, “brain embolism”, “brain hemorrhage”, “cerebrovascular”, “accident”, “anxiet*”, “worr*”, “afraid”, “fear*”, “concern”, “relapse”, “recur*”, “progress*”, “return”, “incidence”, “occurrence”, “influence”, “factor*” and “relevant factor*”. Additionally, references within the included literature were tracked to enhance recall. The search strategy was independently conducted by two experienced investigators (ZY and CC) in information retrieval. Complete details of the search strategy are available in online supplemental table 1.
Supplemental material
Protocol and registration
The review protocol is registered with PROSPERO (CRD42024522147).
Inclusion and exclusion criteria
In this review, the inclusion criteria are as follows: (1) studies involving stroke patients aged 18 years or older; (2) cross-sectional studies; (3) outcome indicators for the incidence of FoP in stroke patients and/or influencing factors, with extractable research data presented as OR and 95% CI; and (4) use of the Fear of Progression Questionnaire-Short Form as the research instrument. The exclusion criteria were as follows: (1) conference abstracts, reviews, systematic reviews, case reports, editorials, letters to the editor, comments, conference summaries, chapters in books and animal studies; (2) literature with incomplete data or inaccessible full texts; (3) studies classified as low quality (score 0–3 points based on the US Agency for Healthcare Research and Quality (AHRQ)14 criteria); (4) literature with repeated publication or data reuse and (5) documents available in both Chinese and English.
Data extraction and synthesis
Two researchers (MW and YY) independently identified relevant literature by reviewing the titles, abstracts and full texts of the retrieved studies. Initially, they read the titles and abstracts to exclude obviously irrelevant literature. Then, they conducted a second screening by reading the full texts to determine the final included literature and extract relevant data. Any disagreements were resolved through discussion and consultation with a third investigator. The extracted data primarily included the first author, year of publication, study area, age, total sample size, incidence of FoP, influencing factors, etc. Two researchers independently completed data extraction, and all researchers subsequently reviewed the data for accuracy.
Quality assessment
The quality of the included literature was independently evaluated by two investigators (MW and YY) using the evaluation criteria recommended by AHRQ.14 The criteria include 11 items, with 1 point assigned for each item answered as ‘yes’, ‘no’ or ‘unclear’. The total score ranges from 0 to 11 points, categorising studies as low quality (0–3 points), medium quality (4–7 points) or high quality (8–11 points). Any discrepancies between two investigators were resolved by consulting a third reviewer (LX).
Statistical analysis
Using Stata V.17.0 software, a meta-analysis was conducted to determine the incidence and influencing factors of FoP in stroke patients. I2 was used to test the heterogeneity of the included literature. If I2<50% and p≥0.1, a fixed-effect model was used for analysis; otherwise, a random-effects model was adopted. To further explore sources of heterogeneity, meta-regression analysis was conducted using covariates such as publication years, research area and stroke type. Subgroup analysis and sensitivity analysis were performed to further investigate the source of heterogeneity. Subgroup analysis categories included average age, study area, types of stroke and year of publication. A leave-one-out sensitivity analysis was performed by iteratively excluding each study to assess the robustness of the pooled estimates. Egger’s test and Begg’s test were used to evaluate publication bias, with p<0.05 considered statistically significant. However, a funnel plot was not used to assess the presence of publication bias because the available literature pertaining to each individual risk factor fell below a threshold of 10, rendering the data too fragmented for meaningful comparisons.
Patient and public involvement
None.
Results
Literature search
A total of 994 records were retrieved from the databases: 152 from PubMed, 150 from the Cochrane Library, 173 from CNKI, 139 from Web of Science, 127 from CBM, 63 from VIP, 50 from Wanfang, 140 from Embase and none from additional records identified through other sources. Subsequently, 153 duplicate studies were excluded. A total of 787 articles were excluded following preliminary screening based on titles and abstracts. Following a re-screening of the full texts, 34 articles were excluded, and 20 articles were ultimately included in the meta-analysis.15–34 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram illustrating the search strategy and study selection is depicted in online supplemental figure 1.
Supplemental material
Characteristics and quality of the included studies
A total of 20 articles were included in this study,15–34 all of which were in Chinese. The study involved 156 patients with cerebral apoplexy, among whom 3054 cases of FoP were reported, with an incidence rate ranging from 32.4% to 87.05%. The study covered nine provinces in China: Shanxi, Shandong, Tianjin, Hainan, Sichuan, Henan, Jilin, Hebei and Guangdong. The average age of the patients ranged from 27.45 to 69.42 years. A total of 38 factors influencing FoP in patients with cerebral apoplexy were identified in China. The results of the literature quality evaluation indicated that 15 articles16 17 19 21–29 32–34 were of medium quality, while 5 articles15 18 20 30 31 were of high quality. The complete details of the characteristics and quality of the included studies are available in table 1.
Characteristics and evaluated quality of the included studies
Meta-analysis of the incidence of FoP in Chinese stroke patients
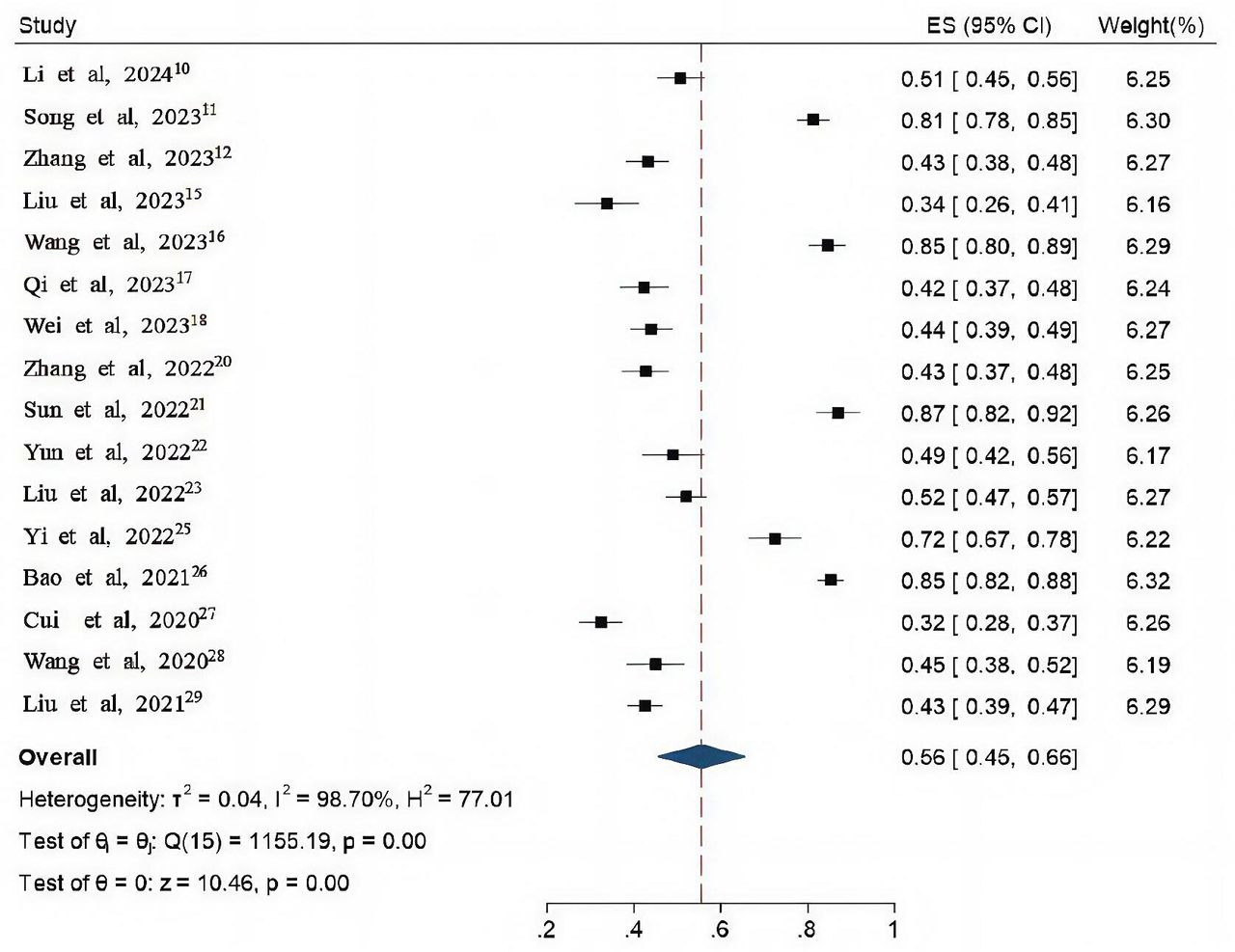
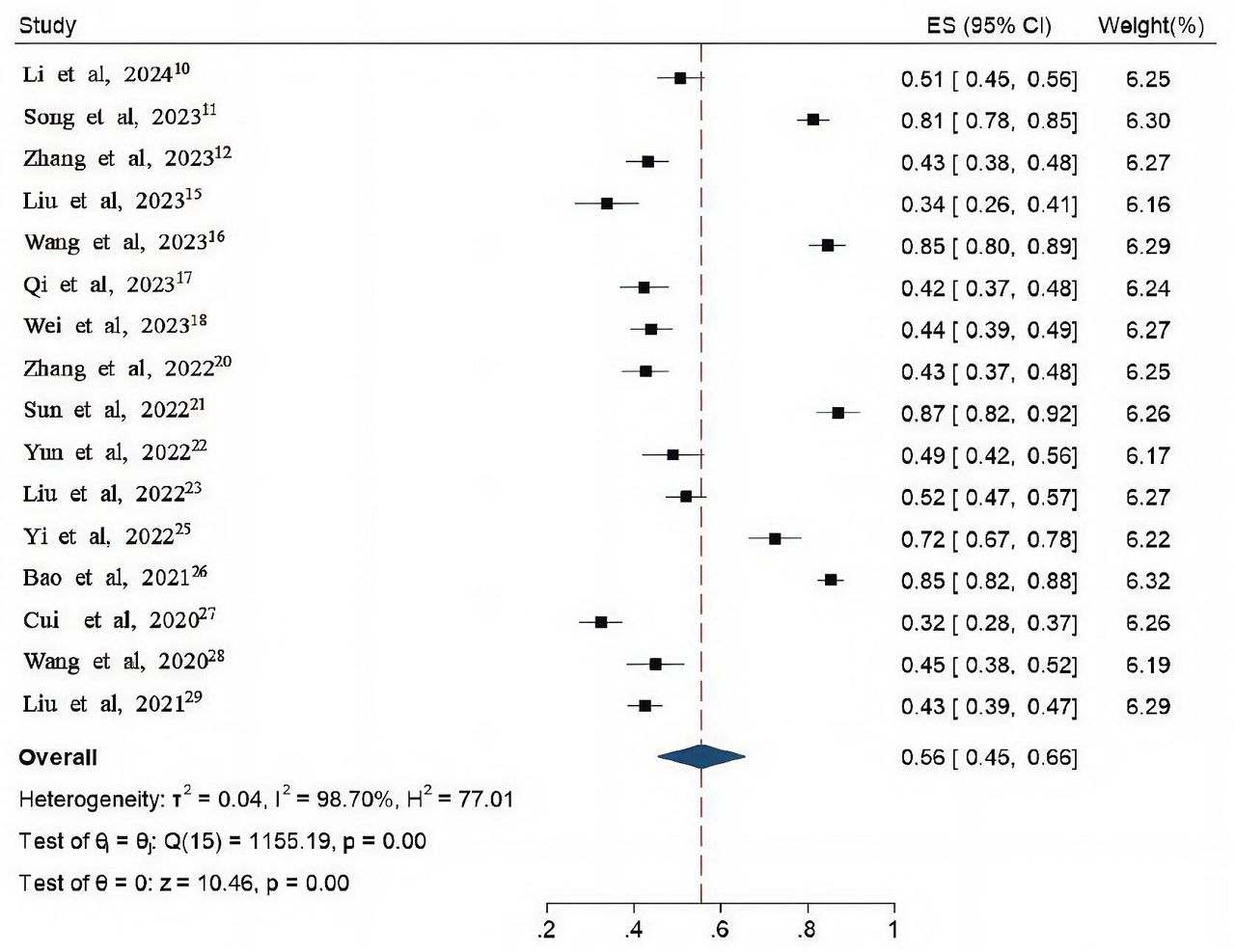
Among the included 20 articles,15–34 16 articles15–17 20–23 25–28 30–34 reported the incidence of FoP in stroke patients. There was significant heterogeneity among the studies (I2=98.7%, p<0.001), so the random-effects model was used for meta-analysis. The results showed that the incidence of FoP in Chinese stroke patients was 56% (95% CI=45% to 66%). The forest plot of FoP incidence in Chinese stroke patients is shown in figure 1.

Forest plot of incidence of fear of disease progression in stroke in China. ES, effect size.
Will be included in the document in accordance with the research area, stroke type, year of publication on subgroup analysis, the results showed: (1) the incidence in North China, East China and Central China was 43% (95% CI=38% to 47%), 70% (95% CI=56% to 83%) and 55% (95% CI=36% to 73%), respectively. (2) The incidence of FoP in ischaemic and haemorrhagic stroke was 45% (95% CI=27% to 64%) and 72% (95% CI=49% to 95%), respectively. (3) Grouped by year of publication, the incidence of FoP before 2020 and after 2020 was 40% (95% CI=32% to 47%) and 59% (95% CI=48% to 70%), respectively. The subgroup analysis of the incidence of FoP in Chinese stroke patients is shown in table 2. To explore potential sources of heterogeneity, we performed meta-regression analyses using publication years, research area and stroke type as covariates. Publication years (B=0.28, 95% CI=0.12 to 0.61, p=0.004) and research area (B=0.41, 95% CI=0.26 to 0.65, p=0.001) were statistically significant predictors of FoP incidence, indicating that more recent studies and studies from specific regions reported higher FoP rates. Stroke type (B=0.30, 95% CI=0.08 to 1.13, p=0.065) showed a marginal association but did not reach statistical significance. Meta-regression results are presented in table 3.
Subgroup analysis of incidence of fear of disease progression in stroke in China
Meta-regression analysis of incidence of fear of disease progression in stroke
Meta-analysis of influencing factors of FoP in Chinese stroke patients
In this study, the influencing factors of FoP were extracted from 15 articles,16 18–20 22–25 27–33 and the studies with ≥2 influencing factors were combined. Meta-analysis results showed that age, education level, income, body mass index (BMI), perception of social support, illness perception and the family intimacy degree are the main factors affecting China’s FoP patients with cerebral apoplexy, with statistically significant difference (p<0.05). Among them, age, education level, economic income, social support and family intimacy were protective factors, as shown in table 4.
Meta-analysis of influencing factors of fear of disease progression in stroke
Sensitivity analysis
The leave-one-out sensitivity analysis demonstrated robust pooled estimates. The amount of total consolidation effect is 0.56 (95% CI=45% to 66%). No single study significantly altered the effect size, confirming the stability of our findings, as shown in figure 2.

{kind=link}
{kind=link}
Sensitivity analysis of the incidence of fear of disease progression in stroke in China.
Test of publication bias
Using Egger’s inspection and Begg’s inspection respectively to evaluate publication bias incidence FoP research, Egger’s inspection (t=2.13, p=0.0517) and Begg’s inspection (Z=0.86, p=0.4440) indicate no significant publication bias. Despite mild asymmetry in the funnel plot (online supplemental figure 2), this pattern is likely attributable to high between-study heterogeneity (I²=98.7%) rather than selective publication. Sensitivity analyses further confirmed the robustness of our findings, as the pooled incidence estimate remained stable when individual studies were sequentially excluded. However, the number of studies included for each influencing factor of stroke patients was relatively small, so no publication bias test was conducted.
Discussion
A total of 16 studies on the incidence of FoP in Chinese stroke patients were included in this study. Meta-analysis results showed that the incidence of FoP in stroke patients in China was 56% (95% CI=45% to 66%), which is considered high and consistent with the research results of Townend et al (56%).9 The significant heterogeneity among the included studies, with an I² of 98.7% as shown in the meta-analysis of FoP incidence in Chinese stroke patients, poses a challenge to the validity of our results. This high degree of heterogeneity can be attributed to multiple factors. First, the studies were conducted in different regions, such as North China, East China and Central China, where there are differences in social and living habits, cultural background, and economic and medical development levels. These regional disparities may lead to variations in the reporting of FoP rates. Second, different types of stroke (haemorrhagic and ischaemic) have distinct prognoses, sequelae, morbidity and mortality, which can influence patients’ psychological states and thus the incidence of FoP. Additionally, the studies were carried out in different time periods, and changes in social environment, such as the faster pace of modern life after 2020, may have affected patients’ mental stress levels and the reporting of FoP. Such diverse influencing factors contribute to the disparate values reported in the included studies and may introduce bias into our overall analysis. Therefore, when interpreting our results, it is crucial to consider the impact of this heterogeneity.
Meta-regression analyses further identified publication years (p=0.004) and research area (p=0.001) as significant predictors of heterogeneity, suggesting that more recent studies and studies from specific regions reported higher FoP rates. The results of the subgroup analysis showed that (1) the incidence of FoP in East China (70%) was higher than that in Central China (55%) and North China (43%). This regional disparity may be driven by variations in healthcare accessibility and socio-economic stressors. For instance, East China’s rapid urbanisation and competitive work environments may exacerbate psychological distress despite better medical infrastructure,35 whereas limited mental health resources in rural Central and North China could delay FoP diagnosis and intervention.36 (2) For different types of stroke, the incidence of FoP in haemorrhagic stroke patients (72%) was significantly higher than that in ischaemic stroke patients (45%), consistent with the findings of Lirong et al.23 This may be because the overall prognosis, sequelae, morbidity and mortality are higher in haemorrhagic stroke patients, leading to lower quality of life and increased psychological distress.37 38 (3) The incidence of FoP after 2020 (59%) was higher than before 2020 (40%), which could be related to the faster pace of modern life and greater mental stress.
Social and demographic factors are significant categories of influencing factors for FoP in stroke patients in China, including age, education level, economic income and BMI. (1) Age: The results of this study showed that age was a protective factor for FoP in stroke patients. This may be because elderly patients usually have rich life experience and most are in the stage of retirement and home care, which grants them stronger psychological tolerance to disease and lower fear of disease progression.39 (2) Education level: The study indicates that a higher level of education is a protective factor for FoP in stroke patients. This is likely because patients with higher education levels have a stronger ability to comprehend disease-related information. After illness, they can independently acquire disease information through books, the internet and other means, and can adopt more effective coping strategies when facing symptoms, thus avoiding excessive fear.40 (3) Economic income: The results of this study showed that economic income was a protective factor for FoP in stroke patients. Stroke has a high morbidity rate, and most patients require long rehabilitation treatment cycles and significant economic support. Patients with low family income have limited medical expenditure, making it difficult to cope with sudden illness and its associated burdens, leading to poor psychological status and more serious fear of the disease.41 (4) BMI: This study suggests that BMI is positively correlated with FoP in stroke patients. Patients with a higher BMI often have insufficient disease cognition or self-management ability,42 leading to a lack of confidence in self-control and management after the onset of the disease. Additionally, overweight and obesity can result in various abnormal health indicators, increasing the risk of stroke recurrence and aggravating patients’ fear of disease progression. Although statistically significant (OR=1.22), the modest effect size indicates BMI should be interpreted cautiously as a predictor of FoP, and clinical interventions should prioritise stronger risk factors. Therefore, clinical medical staff should focus on young patients, those with low education levels, low family income and high BMI. Strengthening the assessment and screening of FoP in these patients, providing predictive nursing care and offering personalised health education and psychological guidance according to patients’ conditions can help improve their confidence in coping with the disease and reduce their fear of disease progression.
Disease-related factors, including illness perception, are a type of influencing factors of FoP in Chinese stroke patients. Illness perception refers to the process by which patients use previous knowledge and experience of the disease to analyse and explain current symptoms or disease, representing the patient’s understanding, recognition and emotional response to the disease.43 This research shows that disease awareness and FoP in stroke patients are positively correlated, meaning the more negative the illness perception, the more severe the FoP. The reason may be that patients with high levels of negative illness perception lack correct understanding of disease-related knowledge and treatment, believe they cannot control disease progression and this sense of losing control over their health contributes to the fear of the disease. Therefore, clinical medical staff should identify patients with high levels of negative illness perception as soon as possible and use acceptance and commitment therapy and cognitive–behavioural therapy to intervene cognitively, correct misconceptions, establish accurate illness perception and enhance patients’ confidence in managing the disease to reduce their fear of disease progression.
Socio-psychological factors, including social support and family intimacy, are major influencing factors for FoP in Chinese stroke patients. (1) Social support: This study showed that social support was a protective factor for FoP in stroke patients. The occurrence of stroke is a negative stress event for patients. During treatment and rehabilitation, patients are very eager to receive help and support from family, friends and other sources. High levels of social support can provide patients with more favourable social resources and emotional care, alleviating their fear to some extent and helping them face life with optimism.44 45 Conversely, low levels of social support can lead to pessimism in patients, which can exacerbate their fear of the disease and its progression. (2) Family intimacy: Family intimacy refers to the closeness, trust, understanding and support between family members. This study shows that family intimacy is a protective factor for FoP in stroke patients. Good family intimacy can provide adequate emotional support, help buffer the discomfort caused by stressful events and encourage positive coping mechanisms, thus reducing psychological pressure and the fear of disease progression.46 Therefore, clinical medical staff should actively mobilise patients’ social support systems, encourage them to express their ideas and seek support from various sources. In addition, caregivers should be encouraged to strengthen communication and care, improve family relationships and positive interactions, jointly cope with the challenges of the disease and reduce patients’ fear of disease progression.
Based on current clinical evidence, psychological interventions such as cognitive–behavioural therapy47 and mindfulness-based approaches48 have demonstrated efficacy in reducing fear of progression in stroke patients. These interventions should be implemented within a multidisciplinary rehabilitation framework, with particular attention to cultural adaptation in the Chinese healthcare context.
However, several limitations of this study should be noted. First, there was significant heterogeneity (I2=98.7%) across the included studies. While subgroup analyses and meta-regression were conducted to explore potential sources of this heterogeneity, the high variability remains a concern and may limit the interpretability of the results. Second, the majority of the included studies were cross-sectional in design, which restricts the ability to establish causal relationships and may introduce recall and selection biases. Third, the quality of the studies varied, with many being of medium quality, which could impact the reliability of the findings. Despite screening the studies using the AHRQ tool, the presence of lower-quality studies may undermine the robustness of the conclusions. Additionally, all studies were conducted in China, which may limit the generalisability of the findings to other countries or cultural contexts. These limitations should be carefully considered when interpreting the results of this meta-analysis. Future research should aim to improve study quality by incorporating longitudinal designs, addressing potential biases and including more high-quality studies with diverse populations. Expanding research to include varied cultural and geographical settings will also help confirm the broader applicability of these results.
Conclusions
The incidence of FoP in Chinese stroke patients is 56%, indicating a high prevalence. Age, education level, economic income, BMI, social support, illness perception and family intimacy are the main influencing factors of FoP in Chinese stroke patients. Clinical attention should be paid to the evaluation and screening of FoP in stroke patients, with a focus on key groups such as those with young age, low education level, low family income, high BMI and low social support. This approach will maximise the supportive role of family and society and reduce negative illness perceptions. Individualised health education and psychological guidance should be tailored to different groups, which is crucial for reducing the occurrence of FoP and improving patients’ quality of life.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We thank the researchers and study participants for their contributions.
References
Footnotes
ZY and CC are joint first authors.
Contributors ZY and CC contributed equally. All authors contributed to the study conception and design; and
approved the final draft of the manuscript. Literature retrieval and study selection: ZY and CC. Data extraction and collection: MW and YY. Analysis and interpretation of data: CC and MW. Supervision and validation: LX. Drafting of the original manuscript: ZY and YY. ZY is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.