Article Text

Abstract
Objective Perinatal loss, which includes miscarriage, stillbirth and neonatal death, is a significant public health problem worldwide. Perinatal loss causes a range of short-term and long-term reactions
in women. Knowing these reactions and coping methods is essential for appropriate support and treatment. This study aims to examine the complex reactions and coping methods experienced by women after perinatal loss.
Design and methods In this study, a qualitative descriptive approach was used, in which indepth interviews were conducted with the data collected using semistructured interviews. 10 women who experienced perinatal loss were included in the study using the snowball sampling method. Analysis was conducted using an inductive content analysis approach.
Results The findings showed that women who experienced perinatal loss exhibited a variety of complex reactions, which could be grouped under five themes. These are emotional reactions, concerns, changes in life, subsequent pregnancy and blame. We also observed that these women used strategies classified under seven different themes to cope, which we expressed as relying on religious or spiritual beliefs, restructuring, the healing power of more challenging experiences, reflecting on worse scenarios, isolating oneself, avoiding remembering and concretising the loss.
Conclusions This study found that women experiencing perinatal loss may react differently and develop different strategies to cope with their loss and reactions. These findings may help to assess the emotional and behavioural states of women after perinatal loss and guide healthcare professionals to provide more individualised care.
- Family
- Maternal medicine
- PERINATOLOGY
- Pregnancy
- PSYCHIATRY
- TRAUMA MANAGEMENT
Data availability statement
Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
It is a study that includes all subgroups of perinatal loss with participants who have experienced miscarriage, stillbirth and neonatal death.
Analysis was conducted using an inductive content analysis approach, which involved coding, theme identification and iterative review to ensure consistency.
This indepth examination provides a critical foundation for understanding the complex emotional processes experienced by women after perinatal loss and how they cope.
Only women were included in this study. Further research could consider the perspectives of fathers who have experienced perinatal loss.
A limitation of this study is that it was conducted in a single country, where cultural factors may have influenced the findings. Future studies could explore cross-cultural differences.
Introduction
The unintentional loss of pregnancy through miscarriage, stillbirth and neonatal death is often examined together under the standard definition of perinatal loss.1 Although there are different definitions, miscarriage is the most common form of perinatal loss, which is defined here as losses occurring before the 24th week of pregnancy.2 Stillbirth includes losses that occur after the 24th week of gestation.3 The death of a baby within the first 28 days of its life is neonatal death.4 Interpretation of data on perinatal loss is hampered by globally varying definitions.5 While miscarriages constitute 10–15% of perinatal losses worldwide,4 approximately 1.9 million stillbirths and 2.3 million neonatal deaths occur each year.6 However, the fact that perinatal losses are not systematically recorded even in developed countries suggests that the rates may be even higher.4 7 For this reason, the experiences of women after perinatal loss may not be fully reflected in the literature. However, perinatal loss can be devastating for women.8
Perinatal loss provokes a range of painful reactions to which bereaved women must respond. Short-term reactions include shock, helplessness, frustration, anger and loneliness; long-term reactions may include anxiety, depression and post-traumatic stress disorder.5 9 Some of these reactions may be exacerbated in subsequent pregnancies following the loss and have significant consequences later in life.10 11 However, women use coping strategies to reduce, manage and live with the symptoms of these reactions.12 These strategies may include adaptive coping strategies as well as maladaptive coping patterns,12 highlighting the importance of professional care and support throughout the entire grief process.13 Adequate clinical care and support provided by trained healthcare professionals can alleviate the psychological effects of reactions to loss and enable the use of adaptive coping strategies.13
Insufficient understanding of postloss reactions and coping strategies may make professional support given to women inadequate.14 What is clear from the existing literature is that the care provided to women experiencing perinatal loss is vital to preventing adverse outcomes and that healthcare professionals may need training to manage the care provided to these women.13 15
This qualitative examination can provide a rich description of responses to loss and coping methods among women who have experienced perinatal loss and consequently a deeper understanding of this complex phenomenon. The findings of this study may provide an evidence base for care provision among healthcare professionals.
Method
This study, which focuses on women’s reactions and coping methods after perinatal loss, was designed as a qualitative descriptive study. Qualitative descriptive studies allow exploring the who, what and where of events or experiences and gaining insights from those who provide information about a phenomenon that is not well understood.16 In this context, ‘reactions after perinatal loss’ and ‘methods of coping with perinatal loss’ of women who have experienced perinatal loss refer to research phenomena. The experiences of women who have experienced perinatal loss were examined in depth through individual interviews. The design and reporting process of the research was based on the Consolidated Criteria for Reporting Qualitative Research criteria,17 which are used in reporting qualitative studies.
Ethical considerations
Study procedures were approved by the İnönü University’s Health Sciences Scientific Research and Publication Ethics Committee (2022/3791).
Participants
Participants of the study were included in the research using the snowball sampling method. Snowball sampling is commonly used in qualitative research. It also allows for reaching a specific group of participants.18 The criteria for inclusion in the study were as follows: (1) participants must be over 18 years of age, (2) the pregnancy was planned or desired, (3) at least 5 months have passed since the last loss, (4) the loss must have occurred after the fifth week of pregnancy or up to 1 month after birth, and (5) participants volunteered to participate in the study. 10 participants who had experienced perinatal loss and met the inclusion criteria were included in the study. Written consent was obtained from each participant prior to data collection. To facilitate the gathering of indepth and rich data, smaller sample sizes are recommended in qualitative descriptive research.19
The characteristics of the participants included in the study are presented in table 1. The age range of the participants was 27–43 years. Among the participants, six participants experienced miscarriage, two participants experienced stillbirth and two participants experienced neonatal death.
Characteristics of the participant
Data collection
Data were collected using semistructured interviews, with the first section identifying demographic characteristics and the second section focusing on exploring the women’s experiences of perinatal loss (online supplemental appendix 1). Before the interviews, the interview guide was piloted, interview questions were revised and process management was reviewed. The interview questions were kept very limited to provide a structured yet flexible framework that allowed participants to share their experiences freely. This approach ensured that key themes were covered while also leaving room for probe and follow-up questions to explore participants’ unique perspectives in greater depth. Probe and follow-up questions were added flexibly according to the flow of the interviews. The interviews were conducted together by researchers, ESB and TU. One researcher’s experience of loss and the other researcher’s experience in the field of midwifery helped the researchers to empathise with the participants and encouraged disclosure among participants. The location of the meetings was decided together with the participants. In this context, three participants were interviewed at their homes and seven participants at their workplaces. The interviews lasted an average of 60 min. All interviews were electronically audio-recorded with the participants’ consent. One of the interviews was repeated because there was a technical problem with one participant’s audio recording. In addition to the audio recording, researchers’ field notes were taken during the interviews. In order to ensure the data reflected what the participants said, the audio recordings were transcribed verbatim, capturing participants’ emotions, for example, crying and signs of distress.
Supplemental material
Data analysis
In data analysis, the content analysis method was used with an inductive approach.20 Content analysis is a method used to analyse data by identifying; however, it is important to acknowledge that qualitative descriptive design stays as near to the data as possible.21–23 The process is to bring together similar data within the framework of certain concepts and themes and organise them in a way that the reader can understand. Accordingly, the data were analysed in four stages: (1) coding the data, (2) determining the themes, (3) organising the codes and themes and (4) defining and interpreting the findings.21 Data analysis was carried out separately by researchers, OTÇ and TU. In this context, the data converted into texts in the first stage were read twice to become familiar with the data. In the second stage, open coding was performed and meaningful parts (codes) suitable for the research purpose were transferred to the Excel table. These codes were placed under themes created by the researchers. While analysing each participant’s data, new codes were coded under previous themes or new themes were created. In the second stage, axial coding was performed. In this context, the relationships between existing codes and themes were evaluated, and some codes were regrouped and revised by creating themes and subthemes. In the final stage of coding, selective coding was performed by re-reading all data to identify codes appropriate to the themes. Themes and codes were reviewed in intermittent meetings during the coding process. After the coding process, the other researcher evaluated the themes and related codes separately. In a joint meeting, the evaluations of all researchers were reviewed and the themes and codes were decided jointly.
Trustworthiness
Lincoln and Guba pointed out the importance of four issues for trustworthiness in qualitative research. These are credibility, transferability, reliability and confirmability.24 Data triangulation, researcher triangulation and methodological triangulation can be used to demonstrate trustworthiness.25 In this study, researcher triangulation was used. Researcher triangulation involves involving more than one researcher in the data collection and analysis process. In addition, peer review and member checking were used for reliability. In this context, support was received from an academic experienced in qualitative research for peer review in all processes. For member checking, participants were asked to comment on whether the raw data, themes, categories and interpretations are realistic and whether that participant believes these findings are reflective of what they said in interview.26 Before finalising the research report, the draft report containing the findings was shared with the participants and member checking was ensured. In addition, within the scope of transferability in the research, data analysis and reporting process were described in detail.
Patient and public involvement
Women who had experienced loss were not involved in the design, conduct, reporting or dissemination plans of this research.
Findings
Theme 1: reactions after perinatal loss
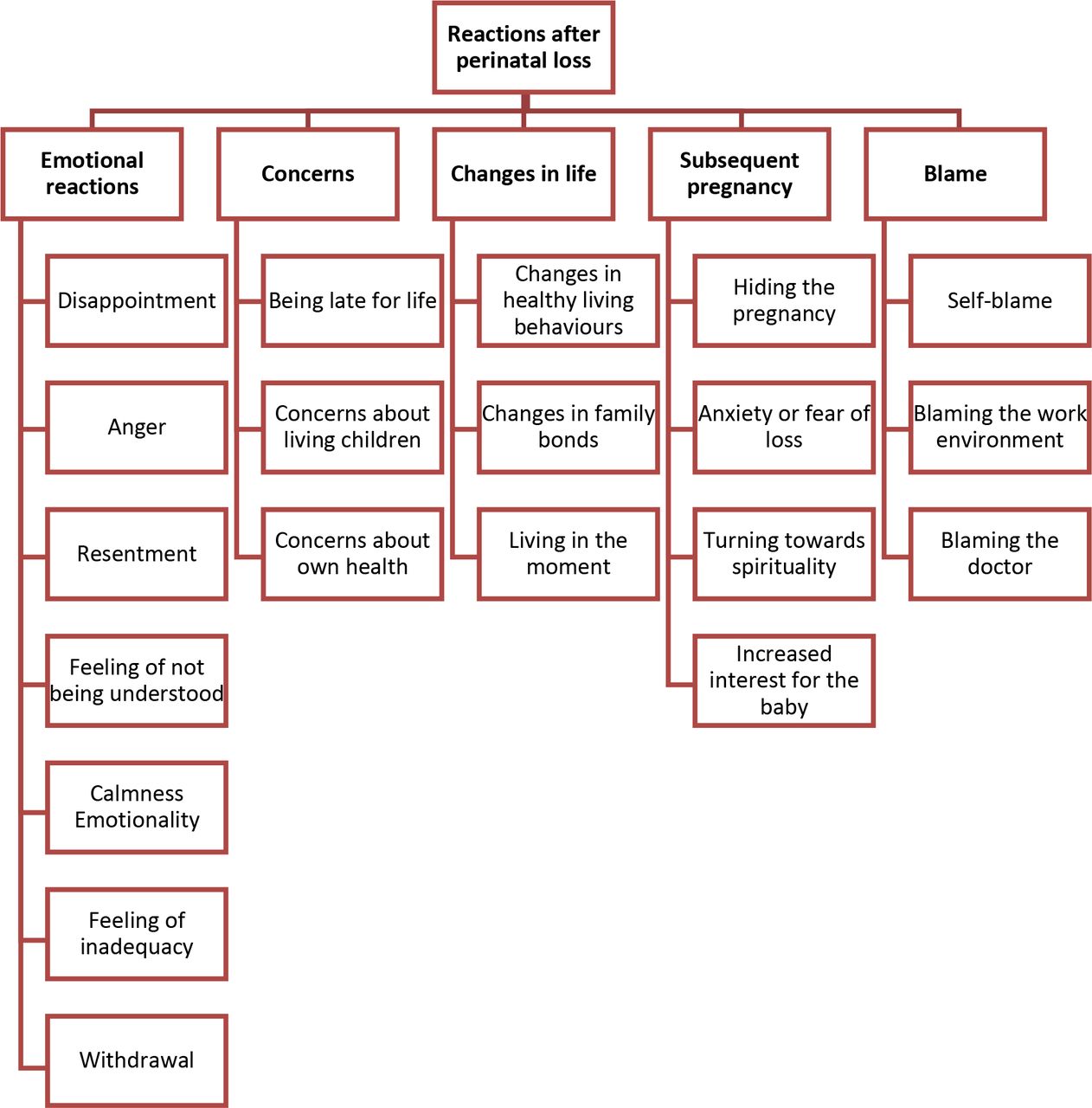
In this study, based on the opinions of participants who experienced perinatal loss, reactions to perinatal loss were examined in depth and five themes and subthemes of these themes were identified. Themes and subthemes for reactions after perinatal loss are presented in figure 1.

Themes related to reactions after perinatal loss.
Emotional reactions
Women’s emotional reactions after perinatal loss were the most dominant theme. The most obvious reaction was disappointment. Participants frequently talked about the emotional bond with their babies and their future plans. Participant M1 expressed her disappointment as follows: “I felt like a woman there for the first time. For the first time in my life, I felt so sad. A huge disappointment for an expectant mother.”
Another emotional reaction was anger. Participants were angry because their loss was unacknowledged within society and in their workplace. Some participants also stated that they felt hurt because they felt that their partners had not provided them with sufficient support and understanding. Women who experienced loss wanted to be understood and their sadness shared, rather than being comforted with words, such as ‘nothing will happen’, ‘something new will happen’ and ‘don’t be sad’. Calmness and withdrawal due to intense complex emotions and lack of understanding were also among the emotional reactions of women. Some participants stated that they started to blame themselves when they saw women with children around them and felt a sense of inadequacy, especially towards their spouses. Here is a comment on this theme:
Participant M3: My feelings of hurt were directed toward my spouse, whom I felt did not understand me and was not there for me as they should have been during that period.
As a result, the most intense emotional reactions of women after perinatal loss were disappointment, anger and hurt, with a strong desire for understanding and sharing their emotions during this challenging process.
Concerns
Three subthemes emerged under the theme of concerns. The theme of being late in life was expressed in two different ways by participants who experienced perinatal loss. Some participants stated that they felt it was too late to fulfil the dreams they had for their lost children, while some participants reported feeling that they were too late to become a mother. Participant M1 expressed her opinion on this issue as follows:
My dream has always been this. Let me catch up with my child. Let me run with my child, go to the cinema, theatre, etc, with my child. I have such a social side. And I always said, “It doesn’t matter if it’s a girl or a boy. I mean, let me grow up with my child.” After experiencing that loss, I said, I would not have it again. It will not happen again, and I will be very late in life. I had a lot of that anxiety.
Concerns about living children were the subtheme frequently mentioned by participants with children. Participants reported intense anxiety about what would happen to their other children or how their children would continue to live if their own physical health was compromised. Participant ND1’s views on this subject are as follows:
In the process, I began to forget my loss. I cried for a long time for my children at home. Oh my God, don’t let anything happen to me. I prayed a lot so that nothing would happen to my children. What would they do if something had happened to me…
Another source of concern for women after perinatal loss was their own health. The participants mostly reported that they were worried about the possible negative effects of the medications administered during the loss intervention process on their health and subsequent pregnancies.
Changes in life
This theme corresponds to changes in family relationships and perspectives on life, especially healthy living behaviours. The reactions to the subtheme of change in healthy lifestyle behaviours are quite complex. Some participants developed a number of healthy lifestyle behaviours such as regular doctor check-ups, paying attention to sleep hours, regular nutrition and exercise. Additionally, one participant stated that she became conscious and sensitive about her own health and that she also started to help those around her. A few participants had a pessimistic attitude. They mentioned that they did not pay attention to their health as they used to, citing the fact that their attention could not affect the results anyway. Participant M4, who started to eat irregularly, expressed her views as follows: “Something in particular happened with my eating and drinking habits. There was a transition to an unhealthy order. While I was a careful person, I started to eat a little unhealthier and irregularly.”
In the context of strengthening family bonds, participants spoke fondly of their spouses who were with them during that period and stated that their interest in their children increased. In addition, the participants spoke highly of the support they received from their close circles such as their mother, brother and aunt. Participant M3, who did not receive sufficient support from her close circle, stated that she chose loneliness. A few participants stated that their perspective on life changed. They started to enjoy the moment and do what they wanted to do without postponing it.
Subsequent pregnancy
Depending on the impact of the loss, there were reactions reflected in the pregnancy process after the loss. The most frequently mentioned issues were hiding the new pregnancy and worrying about losing again. Participants stated that the reason for this was to prevent their close circle from being upset and to relieve the emotional pressure on them in case of a new loss. Regarding this, Participant M6 stated the following: “I didn’t tell anyone until my pregnancy reached 4 months. Because there are people around me who are waiting for me to become a mother and are very happy. When I get sad, they get sadder…”
However, women who became pregnant again after losing their pregnancy stated that they constantly felt uneasy and that their frequency of going to the doctor increased. Increased attention to the baby during the new pregnancy was also a prominent subtheme. Participant ND1’s views on this subject are as follows: “If the baby was moving five times a day when the baby should have been moving ten times, I was suspicious of myself. I was going to the doctor immediately. I wonder what happened? It continued like this until the baby was born.”
Participants stated that they focused more on baby movements during pregnancy and that they sang and talked to their babies. With this interest, some participants felt that they neglected their other children and other responsibilities. Finally, turning to spirituality in the new pregnancy was another subtheme. Some participants mentioned that they read the Quran and prayed more often.
Blame
Participants often blamed themselves, their work environment and their doctors for their loss. Some participants who blamed themselves attributed pregnancy loss to unhealthy eating habits. Some participants attributed their inability to sustain a pregnancy to their own inadequacies. The statement of the M9 participant who blamed herself was as follows: “I blamed myself then. I couldn’t manage it. Well, yes, I could not manage to be a mother either. I couldn’t take care of my baby. I don’t know if I can do it again, ever again. I don’t know if I can protect my baby again. You know, it’s like it’s all my incompetence, my inability to do it.” Regarding working conditions, participants complained about heavy workload and lack of understanding. Participant M4 expressed her disappointment as follows: “I have a job with stressful and difficult working conditions. Even though I was pregnant, I was working the night shift. I continued to work even on the busy days, and my coworkers did not understand me.”
Participants who blamed the doctor talked about the doctor not paying enough attention during the doctors’ checks and not noticing risk symptoms even though they were present.
Theme 2: coping methods after perinatal loss
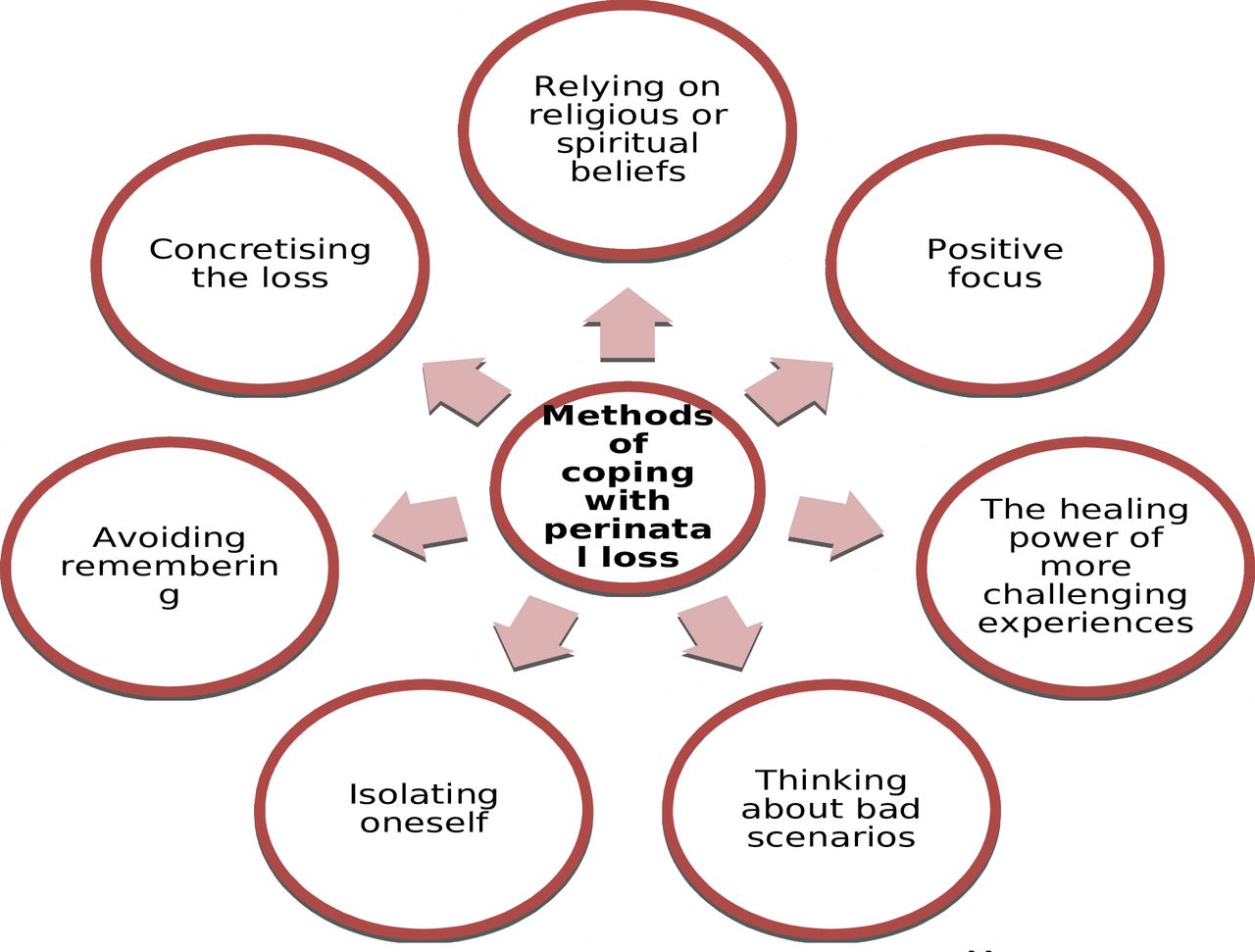
One of the important aims of this research was to gain a deep understanding of the ways women who have experienced perinatal loss deal with loss, based on their experiences. Seven themes were created by bringing together the codes related to this theme. These themes are presented in figure 2.

{kind=link}
{kind=link}
Themes related to coping methods after perinatal loss.
Relying on religious or spiritual beliefs
This subtheme was the most commonly reported coping method by participants. The participants interpreted the loss they experienced as a good thing in accordance with their beliefs and stated that the Creator saw it as appropriate and referred to it as having wisdom. According to Islamic belief, every child is innocent, and if he dies at a young age, he goes to heaven and wants his parents to be with him. In this context, one participant stated that her baby went to heaven and was waiting for her. Participants generally tried to make the loss they experienced meaningful based on their religious beliefs. On this subject, M2 stated the following:
In general, I am a faithful person. Both the giver and the receiver are the Creator. The Creator did not find it appropriate. I have said that if the Creator did not give it, there must be some wisdom. I’ve always said it and I’ll say it again.
Additionally, some participants believe that not accepting the loss or questioning it as if rebelling against God will result in greater punishment. One participant believes that this loss is a test for her and thinks that if she is patient, she will be rewarded and if she is not patient, she will be punished. Participant M5, who has experienced three losses, said the following regarding this subtheme:
I had a hard time accepting it at first. I had a hard time, but every time I had a hard time, I was tested with something else. Every time, every time I had a miscarriage, my child was hurt and I said enough is enough. Every time I got upset, something happened to my son.
In the context of this theme, women often coped with perinatal loss by relying on their religious or spiritual beliefs, interpreting the loss as part of divine wisdom and viewing it as a test requiring patience and faith.
Restructuring
While some participants stated that they were grateful for the existence of their children and that they at least had a healthy child, one of the participants pointed out that she was alive and in good health. Participant M6 expressed this situation as restructuring and transformation. She stated that this experience made her very conscious and even guided the people around her, and she was happy about it. Regarding this subtheme, participant M5 stated the following:
It changed when I fully realised the value of what I had. I saw a few children, they were not healthy, I said ‘Thank goodness’. I was very grateful when I saw them. At least my child is healthy, so long as you have one.
The healing power of more challenging experiences
A participant who experienced an earthquake after the loss emphasised that this difficult experience helped her get rid of the negative emotional state after the loss. While expressing her views, the participant mentioned that there could be worse things in life and said that she actually has valuable things in life, such as a husband who is by her side and a healthy child. Related to this theme, participant M4 stated the following:
When I experienced the earthquake, I said, yes, there are much more important things in life… We are healthy, my husband and child are healthy, I have a child with me, and we are experiencing an event that would end our lives, even if it is momentary… We can have children again. I am healthy and when I faced this, I got out of that emotional state more quickly.
Reflecting on worse scenarios
A few of the participants stated that they accepted the situation and that their pain was alleviated, citing that the child to be born would be unhealthy and that their own health would be in danger if the pregnancy continued.
I swear, people get used to it. May God protect you from the worst. I always say this assuming the worst. Every bad has its worse. What if the baby was born disabled or something happened to me…
Isolating oneself
Two participants stated that they tried to cope with the loss by isolating themselves for different reasons. Participant M5 shared that they constantly saddened themselves, feeling that no one cared about them or their sorrow. As a result, they withdrew into their own world and, after an internal reflection, believed that they needed to overcome this sadness for their own well-being. Participant ND2 said that she did not give anyone, including her husband, the opportunity to support her and that she was trying to heal on her own. Participant ND2 also felt guilty that she had not given her husband a child; consequently, she withdrew from him and was lonely. For this reason, she stated that she felt lonely and wanted to get away from her husband.
Avoiding remembering
Some participants frequently emphasised that they tried to avoid situations that would remind them of the loss. They stated that they gave away the clothes and belongings they bought for the baby, and the more they saw these, the sadder they became, and that is why they tried to get away from the memories. Participant S1 related to this theme stated the following:
I gave away the clothes and stuff. Actually, I kept it for a while. I hid it first. I kept it for about a year or so. After that, I gave them away. I don't know… I thought I wouldn’t see them again. Just in case I see them, I’ll be even more upset… Yes, it’s just like a new pregnancy, a new preparation. I mean, because they would remind me again and again that I had bought these, I had bought this, etc. Yes. Right now I’m trying not to remember as much as I can. Because I feel bad when I remember them.
Concretising the loss
Many of the participants did not want to see the baby after the loss. However, a few participants stated that they visited the baby’s grave after the funeral, which was good for them and eased their pain.
I was not there at the time of the burial. I always blame myself for not being able to go. I thought I’d better go and see. I went and saw. I came home and felt relieved. I said, ‘Okay. Finished.’ (Participant S1)
In addition to the above themes, participant S2, who gave birth in the 26th week of pregnancy, stated that although 1.5 years have passed since the loss, she still cannot accept the loss and has difficulty coping. This participant saw her baby after birth and stated that the baby reacted to her. She shared that she pumped milk to her intubated baby and saw her baby every day for 8 days. The participant’s opportunity to care for her baby and make memories seems to have obstructed the grieving process.
…She turned her head when she heard my voice. She raised her hands and raised her feet. My first feeling actually started after that… the feeling of motherhood. I realised that I was a mother when I saw her… Then I had my son. My husband tried to console me by saying, “If she had been born, maybe, our son wouldn’t have existed.” However, I have not accepted it yet…
Discussion
The purpose of this study is to examine women’s reactions and coping methods after perinatal loss in depth. The findings presented that women who experienced perinatal loss exhibited a variety of complex reactions that we could group under five themes. We also observed that these women used coping strategies classified under seven different themes. This study has helped us better understand the complexity of the experience after perinatal loss and how women respond to this experience.
Our findings suggest that women may experience intense emotional reactions following perinatal loss. One of the most prominent emotional reactions was disappointment. In addition to losing their child, women’s dreams about the baby, role expectations, visions of family life and expected milestones are also lost.27 28 Failure to realise all these expectations with the loss of the baby can cause disappointment. Previous studies reported that mothers who experienced perinatal loss experienced intense hopelessness and disappointment.14 27 Other emotional responses that were particularly notable were anger and hurt. Women expressed anger at the lack of understanding and support from those around them, especially their social circle and workplace. Zhang et al reported negative changes in the social conditions of mothers experiencing perinatal loss. However, social support can reduce feelings of isolation and provide emotional support, information and guidance.29 For social support to be considered useful, it is important that it meets the expectations of the person receiving the support and comes from a trusted person.30 When these conditions do not occur, the person may withdraw instead of seeking support from another source.14 Rather than comforting words, understanding and sharing grief are more important. This can be linked to cultural expectations of men taking on a supportive role for their partners.31 Additionally, in many cultures, social context and religion establish that femininity is synonymous with motherhood.32 Therefore, not being able to have children means that the woman lacks gender identity, and some mothers may contribute to the woman feeling less of a woman and feeling inadequate.14
The concerns experienced by women after perinatal loss may help to better understand the experience and offer support. In our study, in the postloss period, women spoke of increased concern about their own physical and psychological health. The stress and trauma experienced during this period may cause women to become more susceptible to health problems.33 Another major concern for women after perinatal loss was their living children. This concern reflects that mothers have great concern about the future of their living children in the postloss period. This concern is closely related to mothers’ desire to protect the well-being and safety of their children.34 Another important concern was being late for life. The feeling of being late is not only an internal experience of the individual but is also shaped under the influence of social norms. Women often face pressure from the adults around them and society. Cultural norms encourage early reproduction and motherhood and celebrate parenthood.14 35 Families, friends and other social circles can convey the message to women that they need to become mothers before they reach a certain age. This pressure may cause women who have experienced perinatal loss to become more intense with the feeling of, ‘I’m too late to become a mother’.36
Perinatal loss is an experience that also affects lifestyle.37–39 Our findings presented that conscious steps can be taken towards healthy living habits after loss. A metaethnographic study emphasises that after perinatal loss, women abandon risky behaviours, try to adopt a healthier lifestyle and focus on reducing the risk of experiencing a new loss.39 On the other hand, our findings also presented that perinatal loss may lead to a pessimistic attitude towards lifestyle. The basic belief underlying this situation is that the results will not change no matter what happens. This may further increase the negative effects of perinatal loss on individuals. Focusing on healthy lifestyle behaviours in the postloss period can support psychological well-being and help people feel better during this difficult process. Therefore, it is important to be aware of such negative attitudes and try to change these attitudes by getting professional support if necessary.37 Perinatal loss can have profound effects not only on the individual level but also on family relationships.40 In our study, receiving support after perinatal loss had a positive impact on family relationships. In particular, it presented that spousal support further strengthens family bonds. Spousal support can help women alleviate the guilt and sadness they feel about birth failure.41
The perinatal loss process includes trauma that affects the parents and the whole family,32 41–43 and this can cause conflicting emotions in women in subsequent pregnancies.37 44 Pregnancy after loss can provide feelings of hope and excitement to achieve the desired outcome, while also reviving memories of previous losses and pain for the entire family and relatives.37 For this reason, women may choose not to disclose the new pregnancy in order to prevent their close circle from being upset and to relieve the emotional pressure on them.43 Delaying disclosure of a new pregnancy after loss also acts as emotional cushioning.45 However, this can also be associated with the fear of experiencing loss again.43 46 Therefore, women may experience constant anxiety due to this fear and may tend to go for more frequent health checks during their pregnancy and focus more on the health of the baby.47 48 Meredith et al stated that concerns arising from previous perinatal losses may re-emerge in subsequent pregnancies and observed that mothers may be more focused and overprotective towards the next unborn child. A previous study also emphasised that mothers also take into account the concerns and needs of their spouses and other family members.49 These findings help us understand the complexity and emotional impact of pregnancy after perinatal loss.
In our study, we determined that some accusations come to the fore after perinatal loss. In the postperinatal loss period, women’s self-blame may be linked to gender identity and feelings of maternal inadequacy.14 Another accusation after the loss was against doctors. Health professionals are in an ideal position to support women experiencing loss. However, health workers should empathise with women who feel hurt and try to understand women’s emotional needs without taking blame personally.50 Anticipating and identifying pregnancy-related risks, meeting women’s needs through high-quality care, and being aware of the stages of grieving which could include anger and blame can positively impact women’s post-loss experiences.51 Therefore, healthcare professionals’ care for women experiencing perinatal loss should be supported by theory-based models. Another accusation was against the working environment. In the literature, it is stated that women associating their loss with working conditions can lead to decreased job performance, complicated workplace relationships and negatively affected communication with colleagues during the postloss return-to-work process.50 Some women may even consider changing their jobs. All of this can make the emotional recovery process for women more difficult.52 Empathy from colleagues and supervisors can positively affect women’s emotional state.52 53
Our findings suggest that women develop a variety of methods to cope with reactions after perinatal loss. Grief after loss is a universal human response; additionally, social and cultural contexts influence the way grief occurs and the coping strategies used.54 Since all the women in our study have Islamic beliefs, it is not surprising that the most used method of coping is based on religious or spiritual beliefs. Religious beliefs appear to be a source of guidance for women and provide them with strength and motivation during the emotional healing process after loss. Religion may also have a protective effect on mothers in their search for emotional support and meaning during this difficult process.55
In our study, restructuring, the healing power of more challenging experiences, thinking of bad scenarios and concretising the loss stand out as adaptive coping strategies. Some women believe that worse things may happen in life after their loss, and they come to terms with the possibility of having an unhealthy child, choosing instead to focus on their healthy children. These approaches may help alleviate the negative effects of the postloss experience. This may be due to the fact that some of the participants had children living at the time of the loss. A person who becomes aware of the values she has in life after loss understands the value of life more and connects to her values more deeply, and this can positively affect coping after perinatal loss.56 Another step towards developing adaptive coping strategies is to share your own experiences with others and offer them the opportunity to provide guidance.23 Sharing the experience of loss through positive social support and personal interactions may help the process of coping with loss.57
We also determined that maladaptive coping methods such as isolating oneself and avoiding remembering were used after the perinatal loss. Lack of empathy or insensitive/thoughtless comments from peers, partners and close family members after the loss may cause a woman to feel isolated. This type of isolation can complicate coping after loss and leave the woman feeling alone. Therefore, the support and understanding provided to the woman after the loss is important.37 Women who do not receive the necessary support may use avoidance, which is also shown as maladaptive coping in the literature, as a coping method.14 Van and Meleis reported that avoiding situations which remind the bereaved of their loss may obstruct the grieving process. Although avoidance is for the woman’s self-protection, it may not be effective, productive or healthy in the long run.57
Limitations
The strongest aspect of this study is that it includes all subgroups of perinatal loss with participants who have experienced miscarriage, stillbirth and neonatal death. However, only women were sampled in the study which focused on women’s experiences. Considering that men are also affected by perinatal loss in different ways,58 more studies may be conducted in which fathers who have experienced loss are included in the sample. A limitation of this study is that it was conducted in a single country, where cultural factors may influence women’s reactions and coping strategies after perinatal loss. Future research could explore cross-cultural comparisons to provide a broader perspective on this phenomenon.
Conclusion and recommendations
The findings of this study show that women experiencing loss exhibit reactions with high emotional intensity. It was also observed that participants developed various strategies to alleviate their pain and cope with this emotional burden.
This indepth examination provides a critical foundation for understanding the complex emotional processes experienced by women after perinatal loss and how they cope. The study provides important implications for healthcare professionals that may help them develop more effective support and treatment approaches to this issue. Health professionals can offer trust-based counselling to reduce anxiety and provide psychosocial support through open communication, taking an empathic approach to help women express their reactions after perinatal loss. In particular, understanding the differences in coping strategies may be helpful in guiding the design of personalised and goal-oriented interventions.
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the study procedures were approved by the İnönü University’s Health Sciences Scientific Research and Publication Ethics Committee (2022/3791). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the participants who voluntarily participated in this study.
References
Footnotes
Presented at This research will be presented as an oral presentation at the 10th International 7th International Koru Pregnancy, Birth and Postpartum Congress, 25–28 April 2024, Bolu, Türkiye.
Contributors ESB is the guarantor. TU and OTÇ analysed the data and prepared the manuscript. TU and ESB designed the study protocol, and ESB undertook recruitment and data collection. All authors reviewed and contributed to subsequent drafts and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.