Article Text

Abstract
Objectives Congenital anomalies (CAs) are significant contributors to perinatal mortality and morbidity. The epidemiology of CAs in the Gulf Cooperation Council (GCC) countries remains insufficiently explored. This scoping review aims to provide a comprehensive overview of the existing literature on the epidemiology of perinatally diagnosed CAs in the GCC countries.
Design Scoping review.
Data sources We searched MEDLINE, Embase, Scopus and Web of Science for articles published between 1 January 2000 and 1 February 2024.
Eligibility criteria This review included (a) original observational studies such as cross-sectional, cohort or nested case–control studies, which were sourced from general populations, hospital records or registries; (b) published in English between 2000 and 2024; (c) conducted in any of the six GCC countries; and (d) reporting the prevalence or incidence of CAs.
Data extraction and synthesis Two reviewers independently screened titles, abstracts and full texts for inclusion and extracted data using Covidence software.
Results In total, 51 studies reporting the epidemiology of CAs in the GCC countries were eligible and thus summarised. Saudi Arabia dominated with nearly two-thirds of the studies, while Bahrain contributed the least. All studies were hospital based and primarily retrospective. The most researched CAs were cleft lip and cleft palate as well as nervous and circulatory system anomalies, whereas the least researched CAs were chromosomal abnormalities, digestive anomalies and urinary system anomalies. The review reported discrepancies in CA rates across the region, ranging from 2.5 to 68.7 per 1000 live births for multiple anomalies. Few studies explored the association between CAs and risk factors; the main factors reported were advanced maternal age, maternal diabetes and consanguinity.
Conclusions This review summarises the heightened prevalence of CAs in the GCC countries, discrepancies in estimates and gaps in research on specific anomalies. Future research is warranted to explore the association between CAs and various risk factors, thereby enabling the development of targeted preventive strategies.
- Epidemiology
- PERINATOLOGY
- Congenital heart disease
- Prevalence
Data availability statement
All data relevant to the study are included in the article or uploaded as an online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This scoping review maps the available epidemiological data on congenital anomalies (CAs) in the Gulf Cooperation Council countries, following Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews guidelines to ensure a structured approach to literature selection and data extraction.
A narrative synthesis was conducted to summarise the rates of CAs, associated risk factors, and outcomes, using key parameters such as country, study design and diagnostic classification systems.
Non-English-language articles were excluded.
All reviewed articles were hospital based, with emphasis on perinatally diagnosed CAs.
Introduction
Congenital anomalies (CAs) are structural or anatomical abnormalities that develop during intrauterine life, whether detected prenatally, at birth or later in life.1 2 CAs are global contributors to perinatal mortality, morbidity and long-term disability. Despite global progress in survival rates under the age of 5 years, the proportion of child deaths attributed to CAs increased from 4.6% in 2000 to 7.6% in 2019.3 Furthermore, the true burden of CAs might be four times more, since stillbirths and termination of pregnancy due to fetal anomaly are often under-reported.4 CAs are either singular, affecting one system, or show multisystem involvement.5 While genetic influences contribute to 20% of CAs, the majority are of unknown origin and/or shaped by environmental factors that can be partially modifiable. These factors encompass maternal illnesses, infections, medications, substance abuse, radiation and folic acid insufficiency.6
Since the 1960s, global surveys have revealed considerable disparities in CA rates across countries and even within distinct regions of a country. These variations have been attributed to reporting inconsistencies, differences in anomaly types, detection time and socioeconomic factors.7 8 In particular, CAs are the leading cause of neonatal death in the Gulf Cooperation Council (GCC) countries,9 with the United Arab Emirates (UAE) and Qatar ranking 6th and 16th globally, respectively.10 This can be attributed to factors such as multiple pregnancies at advanced maternal age and the high rates of consanguinity.9 However, there has been no systematic assessment of the epidemiology of CAs in the GCC region, and numerous independent studies have shown discrepancies in the rates of CAs. Accurate epidemiological data are crucial for understanding the aetiology of CAs and implementing preventive strategies in this high-risk population. This scoping review aims to provide a comprehensive overview of the epidemiological profile of CAs in the GCC countries.
Methods
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension for scoping reviews guidelines11 (online supplemental table 1).
Supplemental material
Eligibility criteria
This review included original observational studies, such as cross-sectional or cohort studies with a prospective, retrospective or embedded study design (eg, nested case–control), which were sourced from the general population, hospital records or registry based and were published in English; between 1 January 2000 and 1 February 2024. Studies were considered eligible if they were conducted in any of the six GCC countries, namely, Bahrain, Kuwait, Oman, Qatar, Saudi Arabia and the UAE; reported prevalence or incidence rate of CAs. CAs in this study are defined as structural abnormalities diagnosed within the first year of life.
Studies with indeterminate rates or those reporting rates within subpopulations (eg, newborns who have mother with gestational diabetes or were born preterm) or other anomaly groups (eg, the rate of congenital heart defects (CHDs) in newborns with Down syndrome) were excluded. Conference proceedings, reviews, editorials, research letters, commentaries, case–control studies, case reports, case series, clinical trials, genetic and non-human studies were also excluded.
Search strategy
A comprehensive literature search was performed using the MEDLINE-PubMed (National Library of Medicine), Embase, Scopus (Elsevier) and Web of Science-Core Collection (Clarivate) for articles published between 1 January 2000 and 1 February 2024. The search period was extended to the last 24 years in order to capture the latest and the most pertinent research findings in the region, including those from regional registries. To minimise the likelihood of missing evidence, a broad literature search was conducted using a combination of MeSH search terms and keywords (figure 1). All references were imported to Covidence Systematic Review Software.12 The search strategy is detailed in online supplemental table 2. Guided by the inclusion and exclusion criteria, two reviewers (HMHA and RE) independently screened the titles, abstracts and references that were retrieved from the literature search in Covidence. After removing duplicates, studies considered eligible for full-text screening were retrieved for data extraction. Disagreements were resolved by a third, independent reviewer.

The MeSH terms used in the three search domains.
Data charting
A data charting form was designed and piloted on two studies to establish consistency among reviewers. Two independent reviewers (HA and RE) extracted the characteristics from each full-text article. Studies failing to meet the eligibility criteria were excluded at this stage. After independently analysing batches of 20–30 articles, the reviewers convened to resolve disagreements and ensure that all articles were aligned with the research aim and criteria.
Summary measures
CAs were classified by affected body system.13 Studies were grouped into eight categories following the International Classification of Diseases (ICD-10) sequence: ‘CAs of the nervous system (Q00–Q07)’, ‘CAs of the circulatory system (Q20–Q28)’, ‘cleft lip and cleft palate (Q35–Q37)’, ‘CAs of the digestive system (Q38–Q45)’, ‘CAs of the urinary system (Q60–Q64)’, ‘CAs of the musculoskeletal system (Q65–Q79)’, chromosomal abnormalities (Q90–Q99)’ and ‘multiple’ when more than one system was involved. The review involved a narrative synthesis of the included studies, summarising CAs rates, associated risk factors and outcomes using key parameters such as country, study design and diagnostic classification systems. For practicality, studies reporting incidence rates were presented as prevalence, since CAs typically manifest once in a lifetime and are usually evident at birth.14
Patient and public involvement
Patients and the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
Study selection
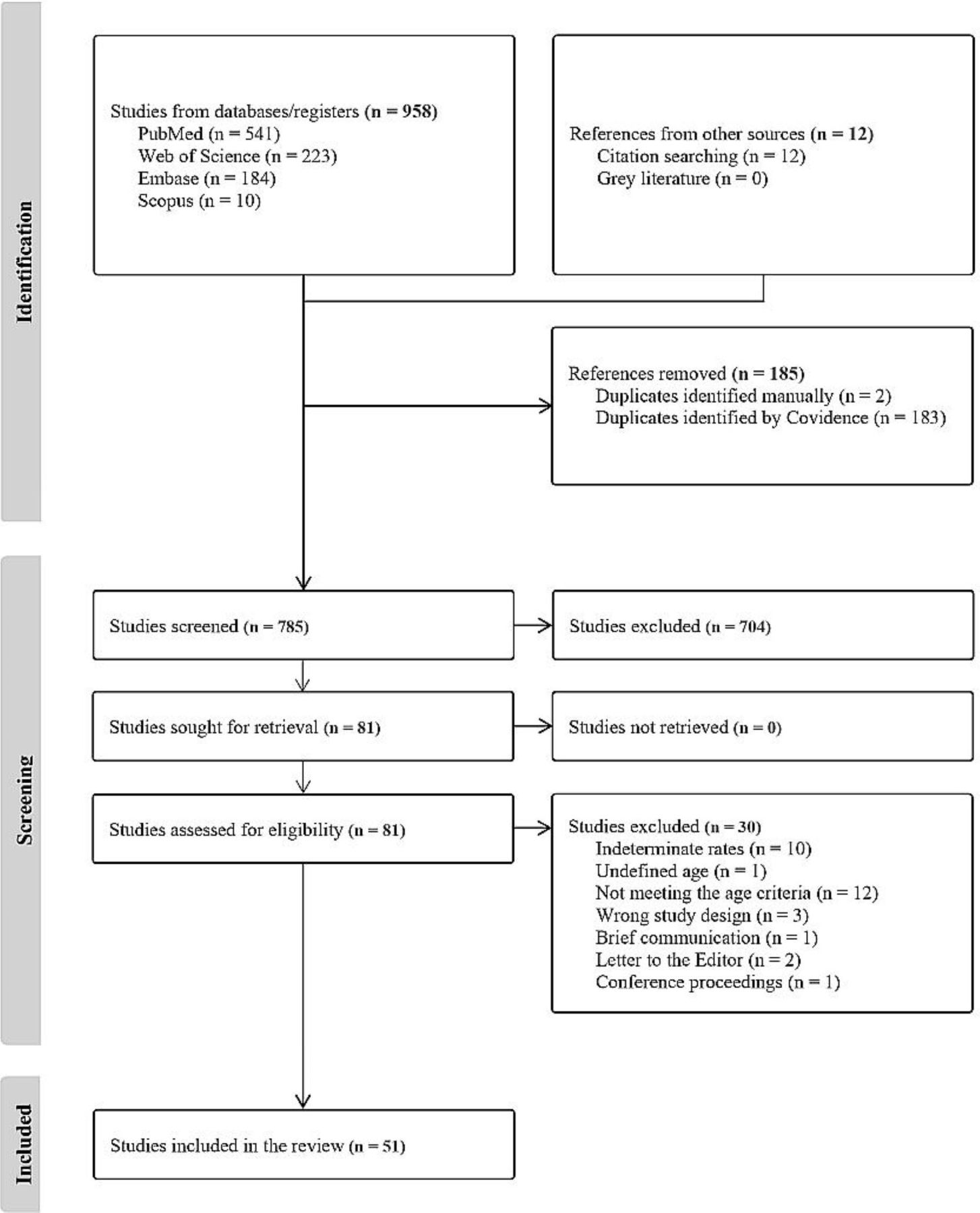
The review process is summarised in the PRISMA flowchart in figure 2. The initial search strategy yielded 958 titles, and citation search yielded additional 12 articles. After removing duplicates, 785 studies were screened, and 704 were excluded as they were not appropriate to this review after assessing their titles and abstracts. After assessing the remaining articles for eligibility, 30 articles were further excluded: 10 had indeterminate prevalence rates, 1 lacked definite participant age, 12 did not meet the age criteria, 3 had faulty study designs, 1 was a brief communication, 2 were letters to the editor and 1 was a conference proceeding (figure 2). Finally, 51 studies fulfilled the eligibility criteria, and their key findings were summarised in online supplemental table 3.

{kind=link}
{kind=link}
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of the search and selection process.
Study characteristics
Online supplemental table 3 displays the characteristics of studies grouped by system (Q00–Q99) and arranged chronologically. The studies were conducted from 2000 to 2023 and all were hospital-based studies. Notably, 32 studies (63%) were conducted in Saudi Arabia, 7 (14%) in Oman, 6 (12%) in the UAE, 3 (6%) in Kuwait, 2 (4%) in Qatar and 1 (2%) in Bahrain. In the majority of studies, the study design was not clearly stated. Nevertheless, 34 studies were determined to be retrospective, 11 were prospective, 4 were cross-sectional and 2 were nested case–control. The sample size varied across studies, ranging from 98 to 375 000 participants. 31 studies exhibited male predominance, 9 showed female predominance, 1 had equal distribution and in 10 studies, neonate sex was unspecified. Diagnostic classifications were reported in 24 studies, whereas 27 studies lacked clear classification. Prevalence rates were reported in 31 studies, whereas incidence rates were reported in 20 studies. The prevalence of multiple anomalies ranged from 2.5 per 1000 live births at the lowest to 68.7 per 1000 live births at the highest.
CAs of the nervous system
This group comprised eight studies: three investigated overall central nervous system (CNS) malformations,15–17 four examined neural tube defects18–21 and one focused on infantile hydrocephalus. All studies were hospital based, with seven conducted in Saudi Arabia15–18 20–22 and one in Qatar.19 The diagnostic classification systems varied, with one study used the ICD-10,19 another employed the Volpe and Barkovich classification16 and the remaining six studies did not employ a classification system.15 17 18 20–22 The rates of CNS malformations among live births ranged from 1.09 to 6 per 1000 live births.18 20–22 Additionally, one study reported a rate of 5.7 per 1000 pregnancies,17 while two studies reportedoverall rates of 1.09 and 3 per 1000 births.15 19 In three Saudi Arabian studies, neural tube defects were the most reported subtype, accounting for 47.7%,15 17.0%17 and 53.3% for spina bifida20 (online supplemental table 3). Risk factors and outcomes were investigated in one study22 including family history of hydrocephalus (OR=9.27, CI: 1.33 to 78.65), low birth weight (<2500 g) (OR=75.75, CI: 15.99 to 418.70), low Apgar score (Apgar<8) (OR=12.38, CI: 4.18 to 37.82), mode of delivery (vaginal/abdominal) (OR=0.13, CI: 0.04 to 0.41) and mortality during the first 6 months of life (OR=10.10, CI: 2.00 to 56.55) (table 1).
Reported risk factors and outcomes
CAs of the circulatory system
Anomalies of the circulatory system were reported in six studies, with three from Saudi Arabia23–25 and one from Oman,26 the UAE27 and Bahrain.28 In three studies, the classification system was unspecified,23 26 28 whereas the remaining three studies, respectively, used the ICD-9,27 ICD-1025 and the International Paediatric and Congenital Cardiac Code.24 Prevalence rates ranged from 5.4 to 10.7 per 1000 live births.23 24 26 28 One study reported a rate of 71 per 1000 pregnancies,27 while another reported an overall rate of 14.8 per 1000 births.25 One study conducted between 2010 and 2013 reported severe CHDs in 7.7% of affected newborns, with an overall prevalence of 3.2 per 1000 total births.25 Among non-critical CHDs, ventricular septal defects were the most prevalent, followed by atrial septal defects (ASDs) (online supplemental table 3). Insulin-dependent diabetes mellitus was identified as a significant risk factor (OR=3.8, CI: 2.44 to 5.79)25 (table 1).
Cleft lip and cleft palate
This group consisted of 10 studies: 2 for cleft and palate,29 30 3 for oral and orofacial clefts,31–33 1 for syndromic cleft lip and palate (SCLP) and non-SCLP34 and 4 for non-syndromic orofacial clefts.35–38 Of these, seven studies were from Saudi Arabia,29 33–38 two from Oman30 31 and one from Kuwait.32 Five studies used the lip, alveolus, hard and soft palates from right to left classification system,32 35–38 one used Davis and Ritchie’s system33 and four did not report any.29–31 34 All rates were reported per 1000 live births, with the highest being 2.6/1000 in Oman,30 while the lowest was 0.57/1000 in Kuwait32 (online supplemental table 3). Consanguinity (OR=2.5, CI: 1 to 6.46) was identified as a risk factor in one study37 (table 1).
CAs of the digestive system
CAs of the digestive system were reported in two studies that examined overall gastrointestinal tract (GIT) anomalies39 and anorectal malformations (ARMs).40 Both studies were hospital based, conducted in Saudi Arabia, and had an unspecified diagnostic classification. All rates were reported per 1000 live births, with 1.3 per 1000 for overall GIT anomalies39 and 1 per 1000 for ARMs specifically40 (online supplemental table 3).
CAs of the urinary system
Two hospital-based studies from Saudi Arabia41 42 examined urinary system anomalies; however, neither specified a diagnostic classification. The rate of congenital anomalies of the kidney and urinary tract was 3.26 per 1000 births,42 while the rate of antenatally detected urinary tract abnormalities (ADUTA) was 17 per 1000 pregnancies.41 Congenital hydronephrosis was the most frequently reported subtype in the two studies, with sample sizes of 18 853 and 43 209, accounting for 95.7%41 and 51.1%42 of cases, respectively (online supplemental table 3).
CAs of the musculoskeletal system
Developmental dysplasia of the hip (DDH) was examined in five hospital-based studies, including three from Saudi Arabia43–45 and two from the UAE.46 47 The diagnostic classification system was unspecified in all studies, except one study that used the Graf classification system.47 All rates were reported per live births, with two studies from Saudi Arabia documenting the highest and the lowest rates at 31/100044 and 3.7/1000,43 respectively (online supplemental table 3). Significant factors and outcomes were reported in two studies.43 44 These include positive family history (p value=0.040), age at diagnosis (months) (p<0.001), age of presentation (OR=0.48, p=0.04) and breech presentation (OR=2.36, p=0.04) (table 1).
Chromosomal abnormalities
Two hospital-based studies examined chromosomal abnormalities in the neonatal period: one from Saudi Arabia used the ICD-10 system,48 while another from the UAE did not specify any classification.49 The overall rate of chromosomal abnormalities was 2.8/1000 live births.48 Trisomy 21 (Down syndrome) was the most prevalent disorder (83.3%); although other trisomies involving chromosome 13 (Patau syndrome) and 18 (Edwards syndrome) also appeared in relatively low frequencies at 3.8% and 2.6%, respectively.48 In the UAE study, the overall prevalence of Down syndrome was 2.2 per 1000 live births49 (online supplemental table 3).
Multiple anomalies
Multiple anomalies were discussed in 16 hospital-based studies, with seven originating from Saudi Arabia,50–56 four from Oman,8 57–59 two from Kuwait,60 61 two from the UAE62 63 and one from Qatar.64 Among these, six studies used the ICD-10 system,8 55–57 63 64 two applied the London Dysmorphology Database,58 59 two employed the European Registration of Congenital Anomalies and Twins (EUROCAT),50 54 one used the ICD-9,62 and in five studies, the diagnostic classification system used was unspecified.51–53 60 61 Three studies reported rates per 1000 pregnancies,51 53 61 while six reported rates per 1000 births51 54 55 58–60 (online supplemental table 3). Four studies54–57 identified the following significant factors and outcomes: consanguinity (OR=1.5, CI: 1.28 to 1.8), (OR=1.5, CI: 1.2 to 1.9), advanced maternal age of more than 35 years (OR=6.224, CI: 3.023 to 12.820) and more than 40 years (OR=2.1, CI: 1.35 to 3.3), advanced paternal age of more than 40 years (OR=13.056, CI: 5.867 to 29.05), maternal illiteracy (OR=1.4, CI: 1.17 to 1.7), maternal diabetes mellitus (OR=1.98, CI: 1.33 to 2.95) or overt diabetes mellitus (OR=2.7, CI: 1.4 to 5.4), preterm birth (RR=1.98, CI: 1.55 to 2.53), (OR=3.949, CI: 0.978 to 15.937), low birth weight of less than 2.5 kg (RR=0.28, CI: 0.23 to 0.35), history of a sibling with an anomaly (OR=1.49, CI: 1.04 to 2.12) and male sex (RR=1.98, CI: 1.72 to 2.27) (table 1).
Discussion
This review summarised the epidemiological profile of CAs in the GCC countries. Saudi Arabia generated the most literature, accounting for 63% of the included studies. Cleft lip and cleft palate, as well as anomalies of the nervous and the circulatory systems, were the most extensively researched CAs. However, research on specific systems, such as the respiratory and genital systems, was lacking. This is worrying given the significant impact of these anomalies on individuals, families and healthcare systems. Our review revealed disparities in CA estimates across the region, with rates of multiple anomalies ranging from 2.53 to 68.7 per 1000 live births. These variations can be attributed to inconsistencies in reporting, including differences in case definition, classification systems, and study designs across various studies. Furthermore, many of the included studies did not account for bias, lacked diagnostic classification or reported rates in a different manner. For instance, some presented incidence rates, whereas others reported prevalence rates inconsistently. Moreover, most studies solely accounted for live births, thus potentially underestimating the true prevalence.65 66
The review documented higher overall rates of CAs compared with international studies such as the EUROCAT ‘23.9/1000’,67 the British Isles Network of Congenital Anomaly Registers ‘20.6/1000’68 and the Bradford study ‘30.5/1000’.69 The rates in the GCC countries were lower than those reported in Sudan ‘82/1000’,10 but higher than the rates in Egypt ‘20/1000’70 and Morocco ‘5.58/1000’.71 These heightened rates may be attributed to the high consanguinity rate in the region.9 Nevertheless, the diversity within EUROCAT supports the aim of this review and provides a valuable benchmark for understanding the variations in CA rates across regions.
Among the known risk factors of CAs, consanguinity, advanced parental age and maternal diabetes were frequently reported. However, quantifying the strength of these associations was challenging due to the limited number of studies reporting these factors. Additionally, several risk factors could have been overlooked in this review as they remained unknown or were not addressed in the included studies. Furthermore, the studies assessing age lacked consensus on a specific threshold, and some reported risk factors without a clear causal mechanism. Moreover, the lack of standardisation in age thresholds for risk factors affected comparability and interpretation across studies.
Consanguinity rates in the GCC countries are up to 60% higher than that of other countries, with the offspring of consanguineous unions being at higher risk of autosomal recessive illnesses caused by recessive genes.72 73 This underscores the significance of implementing screening and premarital counselling programmes.9 Another known risk factor for CAs is advanced parental age,74 with this association shaped by various biological factors such as mutations, aneuploidies and environmental exposures.75 Diabetes mellitus is a well-established risk factor for CAs.76 Studies have shown that hyperglycaemia inhibits cell growth and increases apoptosis due to heightened oxidative stress.77 In the GCC countries, the rates of diabetes mellitus are higher, with obesity, parity and advanced maternal age being major contributors.78
Strengths and limitations
This scoping review addressed a significant research gap by comprehensively assessing CAs in the GCC countries. It highlighted key knowledge deficiencies and urged further research to enhance the understanding of CAs in the region. Nevertheless, the review had some limitations. First, the included studies were predominantly retrospective, potentially introducing bias that was not formally assessed. However, the review aimed to summarise the existing literature rather than assess the quality of studies or the risk of bias. Additionally, meta-analysis was beyond the scope of this review, as scoping reviews are intended to provide a descriptive overview rather than data synthesis, and the substantial heterogeneity in study designs, data collection methods and case definitions among the included studies precluded meaningful quantitative synthesis. Second, instead of being nationwide, most studies had a localised scope, thus limiting comparability and trend identification. Furthermore, the absence of standardised methodologies and the inconsistencies in the included studies’ periods restricted a thorough temporal analysis. Third, all reviewed articles were hospital-based, with a primary emphasis on perinatally diagnosed CAs. However, hospital-based registries only capture anomalies that are evident during hospitalisation,79 which might underestimate the true prevalence of CAs. Moreover, the emphasis on perinatally diagnosed CAs may have overlooked anomalies that manifest later in life. Variations in the age of diagnosis and the potential for false-positive or false-negative diagnoses are other limitations. For instance, one study reported a suspected birth prevalence of DDH at 27 per 1000 live births, which dropped to 3.2 per 1000 in the weeks following birth.46 In addition, a study on ADUTA reported a false-positive rate of 26.7%, since the anomaly disappeared during the first postnatal ultrasound.41 The EUROCAT classifies hydronephrosis with renal pelvis dilation<10 mm as a minor anomaly since over half of the antenatally detected cases show spontaneous resolution after birth. Similarly, ASD is classified as major CA, whereas patent foramen ovale is not.80 This variability highlights the challenges in estimating the actual prevalence of CAs and distinguishing them from normal variants. This also emphasises the need for longitudinal follow-up, cautious interpretation and further research.
Future research must address the gaps that have been highlighted in this review. Unfortunately, none of the included studies provided a comprehensive overview of CAs, emphasising the need for further research to encompass a broader spectrum of CAs. Furthermore, future research must prioritise quality assessment, given the potential variability in the quality of reviewed articles. In addition, researchers should tackle the challenge of diagnosing CAs. More than simply including the initial suspected diagnoses, community-based studies should be further integrated to ensure data accuracy and comprehensiveness. Additionally, future endeavours must adopt a standardised classification of CAs based on organ-specific categories rather than general body systems. Cases involving multiple anomalies should also be further distinguished between chromosomal and non-chromosomal anomalies, a crucial differentiation to ensure data quality and interpretability in any dataset or registry. Prioritising antenatal diagnosis and incorporating a broader spectrum of pregnancy outcomes, such as stillbirths and spontaneous abortions, is essential for accurately estimating the burden of CAs. Moreover, cohort studies should be prioritised to strengthen the robustness of findings, and developing national or regional registries would allow consistent and systematic data collection.
Addressing the burden of CAs necessitates a comprehensive, integrated approach that combines public health initiatives, preventive strategies and policy interventions. Premarital and genetic counselling programmes are critical for raising awareness and promoting informed reproductive choices. Enhanced maternal healthcare initiatives, such as improved diabetes management and folic acid fortification, play a vital role in optimising maternal and fetal health. Strengthening antenatal screening programmes facilitates early detection and timely intervention, which improve perinatal outcomes. Additionally, establishing national surveillance systems is essential for tracking, standardised reporting, trend monitoring and data-driven planning to enhance CAs prevention and management. Finally, quantifying the association between various risk factors and CAs, as well as investigating their causal mechanisms, is imperative for implementing effective prevention strategies centred on modifiable risk factors. Nevertheless, it is important to acknowledge that, despite efforts to mitigate modifiable risk factors, absolute prevention of certain anomalies might not be achievable.
Conclusion
This is the first review of the epidemiology of CAs in the GCC countries. Heightened rates of CAs were reported in the region. Cleft lip and cleft palate were the most researched CAs, with Saudi Arabia being the primary contributor to the literature. Research on specific systems was notably scarce, and the majority of the studies were localised rather than nationwide. Among the known risk factors of CAs, advanced parental age, maternal diabetes and consanguinity were the main reported factors. Implementing standardised national surveys alongside systematic reviews with meta-analyses is crucial to address the knowledge gap and understand the burden of CAs. Investigating the association between CAs and various risk factors is imperative for developing targeted prevention strategies.
Data availability statement
All data relevant to the study are included in the article or uploaded as an online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
X @iffatelbarazi
Contributors HA and LAA conceptualised and designed the review. HA and RE searched the literature, retrieved the eligible studies and extracted the data. HA drafted the manuscript. HA, LAA and RE reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript, and HA acted as guarantor.
Funding This review was supported by the Zayed Centre for Health Sciences, United Arab Emirates University (Grant # 31R239). The funder had no role in the conceptualisation, literature search, selection of studies, interpretation of findings, manuscript preparation or the decision to submit the paper for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.