Article Text

Abstract
Objective The aim of this study was to investigate the incidence, risk factors and airway management of postoperative haematoma following anterior cervical spine surgery (ACSS).
Design A retrospective nested case-control study.
Setting A tertiary hospital in China.
Participants A total of 13 523 patients within a single-centre longitudinal ACSS cohort were identified from March 2013 to February 2022. Patients with postoperative haematoma after ACSS were enrolled as the haematoma group, and others in the cohort without haematoma were randomly selected as the non-haematoma group by individually matching with the same operator, same gender, same surgery year and similar age (±5 years) at a ratio of 4:1. Subsequently, patients with haematoma were included in a subgroup for analysis.
Primary outcome measures Postoperative haematoma and difficult intubation prior to haematoma evacuation.
Results The incidence of postoperative haematoma out of all ACSS was 0.4% (55/13 523). A total of 275 patients were enrolled in the study, including 55 patients in the haematoma group and 220 patients in the non-haematoma group. Anterior cervical corpectomy and fusion (ACCF) (OR 2.459; 95% CI 1.302 to 4.642; p =0.006) and the maximum mean arterial pressure (MAP) during recovery (OR 1.030; 95% CI 1.003 to 1.058; p =0.028) were identified as independent risk factors for haematoma. In the subgroup analysis, 29% of patients with haematoma experienced difficult intubation, and retropharyngeal haematoma (OR 10.435; 95% CI 1.249 to 87.144; p =0.030) was identified as an independent risk factor for difficult intubation. Patients with haematoma had longer hospitalisation duration (p <0.001) and greater costs associated with their stay (p <0.001).
Conclusion ACCF and elevated maximum MAP during the recovery period were independent risk factors for postoperative haematoma following ACSS. Patients with post-ACSS haematoma are at high risk of a difficult airway, with retropharyngeal haematoma being strongly associated with challenging airway management. Postoperative haematoma was associated with longer hospitalisation duration and greater costs.
Trial registration number China Clinical Trial Registry: ChiCTR2400086263.
- Anaesthesia in neurology
- Spine
- Neurosurgery
Data availability statement
Data are available in a public, open access repository. The data underlying this article are available in Mendeley Data Repository, at https://data.mendeley.com/datasets/6rx5wgp75p/1.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study’s large sample size (13 523 patients) strengthened result reliability through a retrospective nested case-control design that controlled confounders via matching.
The single-centre longitudinal cohort ensured consistent data collection while analysing both postoperative haematoma risks and intubation difficulties comprehensively.
The retrospective design may introduce selection bias and limits the ability to establish causal relationships.
The low postoperative haematoma incidence (0.4%) may limit statistical power for detecting rare risk factors.
Introduction
Haematoma after anterior cervical spine surgery (ACSS) is a rare complication in clinical practice, with an incidence of 0.4%–1.2% reported in the literature.1 2 The location of haematoma occurrence determines its type, which can be divided into three categories: wound haematoma, retropharyngeal haematoma and spinal epidural haematoma.3 Wound haematoma typically manifests as localised swelling and ecchymosis at the injury site. Retropharyngeal haematoma often presents with respiratory symptoms and can potentially progress to acute airway obstruction, a critical and life-threatening condition.4 Spinal epidural haematoma typically presents with progressive neurological deficits. Severe cases of haematoma may potentially result in severe morbidity or mortality.
Timely evacuation of haematoma is an efficacious intervention, notably beneficial for retropharyngeal haematoma and spinal epidural haematoma.5 In the management of airways prior to haematoma evacuation surgery, particular attention must be paid to the occurrence of difficult airways to prevent a ‘can't intubate, can't ventilate’ situation.6 Given the infrequency of haematoma and the potential for severe outcomes, it is imperative to conduct early and systematic assessments of risk factors for haematoma. We report the findings of a retrospective nested case-control study aiming to investigate the incidence and risk factors of postoperative haematoma following ACSS.
Methods
Study population and study design
The present study enrolled patients who underwent ACSS at Peking University Third Hospital between March 2013 and February 2022. The selection of this study period was based on the comprehensive implementation of the electronic health records system in the hospital, which ensured the availability of complete and reliable data. Inclusion criteria were as follows: (1) cervical spondylosis; (2) ACSS; (3) elective surgery. Exclusion criteria were as follows: (1) combined anterior and posterior cervical surgery; (2) transoral approach to C1-C2; (3) cervical spine tumours; (4) cervical spine fractures; (5) incomplete medical records. In the present study, postoperative haematoma following ACSS is defined as a symptomatic haematoma characterised by respiratory distress, neurological deficits or other haematoma-related symptoms, confirmed by imaging findings or surgical evacuation. Patients with postoperative haematoma after ACSS were enrolled as the haematoma group, and others in the cohort without haematoma were randomly selected as the non-haematoma group by individually matching with the same operator, same gender, same surgery year and similar age (±5 years) at a ratio of 4:1.
Variables
The general characteristics of the two groups were collected, including age, gender, body mass index (BMI), medical comorbidities, smoking history, anticoagulant or antiplatelet therapy, preoperative coagulation function tests and platelet counts. Disease-related factors encompassed the classification of cervical spondylosis types, such as myelopathy type, radiculopathy type or other types, as well as preoperative Modified Japanese Orthopaedic Association (m-JOA) scores and Neck Disability Index (NDI) scores. Surgical factors included surgical segments, ossification of the posterior longitudinal ligament (OPLL) within the surgical segments, anterior cervical corpectomy and fusion (ACCF), duration of surgery, estimated blood loss (EBL) and postoperative drainage volume. Anaesthetic factors involved the American Society of Anesthesiologists (ASA) physical status classifications and mean arterial pressure (MAP) during both preoperative and postoperative recovery phases. Data on hospitalisation duration and costs were also gathered.
Anticoagulant therapy is defined as a history of using anticoagulant agents such as warfarin or low-molecular weight heparin. Antiplatelet therapy is defined as a history of using antiplatelet agents such as aspirin or clopidogrel. Preoperative coagulation function tests included prothrombin time (PT), international normalised ratio (INR), fibrinogen levels, activated partial thromboplastin time (APTT), and thrombin time (TT). The preoperative MAP was routinely assessed on the patient’s admission to the ward, and the maximum MAP recorded during the recovery period was obtained from anaesthesia records.
We conducted a subgroup analysis of haematoma patients, with a focus on airway management. Patients were stratified based on the occurrence of difficult intubation prior to haematoma evacuation surgery. A comparative analysis was performed on various parameters between the groups, including sex, age, BMI, hypertension, C3 or C4 involvement, type of haematoma, the interval from symptom onset to airway intervention, time of presentation of haematoma and ASA physical status classifications to assess correlations and statistical differences associated with difficult intubation. Additionally, the occurrence of difficult intubation prior to the initial surgical procedure was systematically assessed. Difficult intubation was defined as a clinical scenario requiring more than three attempts by an experienced anaesthesiologist to achieve endotracheal intubation.7
Statistical analysis
For continuous data that were normally distributed, descriptive statistics were presented as mean±SD. Data that were not normally distributed were described using median and IQR. Differences between the two groups for continuous variables were analysed using an independent samples t-test (for data with a normal distribution) or a Mann-Whitney U test (for data without a normal distribution). Categorical data were expressed as percentages and analysed for differences using the χ2 test or Fisher’s exact test. A binary logistic regression model was applied to identify multivariate variables, using the backward Wald method for variable selection. ORs and 95% CIs were used to quantify the strength of associations. The accuracy of diagnostic tests was assessed using receiver operating characteristic curves and the area under the curve (AUC). Statistical analyses were performed using SPSS V.26.0, with all tests being two-tailed and p value <0.05, indicating statistical significance of differences.
The number of postoperative haematoma cases identified during the study period dictated the overall sample size. In subgroup analyses, the count of difficult intubation cases similarly determined the subgroup sample size. According to the principle that the number of events per variable should be no less than five, which means the number of outcome events corresponding to each independent factor must meet this threshold, an appropriate number of independent variables were included to satisfy the sample size criterion based on the actual occurrences of outcome events.
Results
Incidence and time of presentation of postoperative haematoma
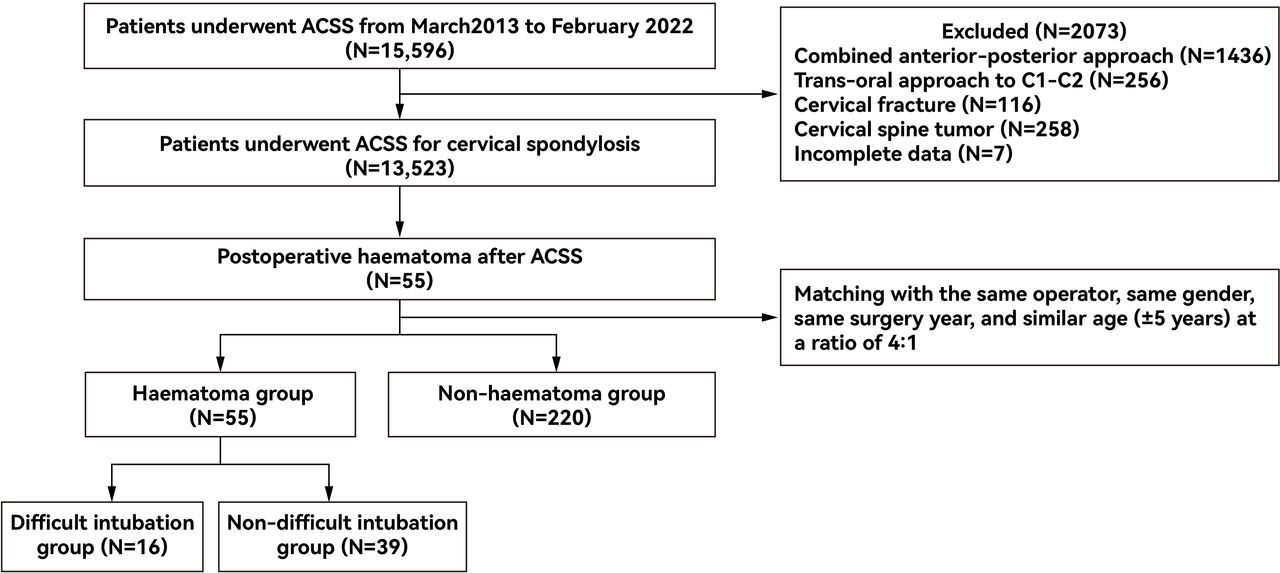
From March 2013 to February 2022, a total of 13 523 patients undergoing ACSS met the inclusion criteria. Of these, 55 patients developed postoperative haematoma, resulting in an incidence rate of 0.4%, with retropharyngeal haematoma occurring at a rate of 0.28% and spinal epidural haematoma at 0.12%. Patients without haematoma were randomly selected as the control group, individually matched for the same surgeon, gender, surgery year and age within a 5-year range, at a ratio of 4:1. Consequently, the haematoma group comprised 55 cases, while the control group included 220 cases (figure 1). The onset of haematoma varied significantly among patients, with the earliest cases presenting as soon as 0.5 hours postoperatively and the latest occurring up to 7 days after surgery. Notably, four of these patients exhibited symptoms shortly after the removal of drainage tubes.

{kind=link}
Flow diagram outlining the selection of the study population. ACSS, anterior cervical spine surgery.
Difference between the haematoma group and the non-haematoma group
The comparative analysis revealed no statistically significant differences between the two groups in demographic characteristics, anticoagulant or antiplatelet therapy, the classification of cervical spondylosis, surgical segments, OPLL within the surgical segments, surgery duration, EBL, drain volume or ASA physical status classifications, as shown in table 1.
Comparison between the haematoma group and non-haematoma group
The two groups exhibited statistically significant differences in ACCF (p =0.011) and the maximum MAP during the recovery period (p =0.031). Patients in the haematoma group had longer hospitalisation duration (p <0.001) and incurred greater costs (p <0.001) (table 1). Analysis of the preoperative blood tests between the two groups showed statistically significant differences in APTT (p =0.011) and PT (p =0.05). In clinical practice, an extension of PT by 3 s and APTT by 10 s is deemed to have clinical significance. However, in the present study, the mean values of PT and APTT for both the haematoma group and the non-haematoma group were within the normal range. Consequently, PT and APTT were not included in the binary logistic regression analysis. Instead, other factors with a p value <0.1 were incorporated into the model. Binary logistic regression analysis revealed that ACCF (OR 2.459; 95% CI 1.302 to 4.642; p=0.006) and the maximum MAP during the recovery period (OR 1.030; 95% CI 1.003 to 1.058; p=0.028) were independent risk factors for haematoma, as detailed in table 2. The AUC for the maximum MAP during the recovery period was calculated to be 0.594 (95% CI 0.510 to 0.679; p=0.031), whereas for ACCF, the AUC was 0.586 (95% CI 0.499 to 0.673; p=0.048). According to the highest Youden’s index, the cut-off value of the maximum MAP during the recovery period was set to 106 mm Hg, with the sensitivity and specificity being 0.727 and 0.473, respectively.
Binary multivariate logistic regression (backward Wald) analysis of the risk factors for haematoma.
Subgroup analysis of airway management in haematoma patients
Prior to the initial surgery, only one case of difficult intubation was observed among 55 patients. All 55 cases of haematoma patients underwent haematoma evacuation surgery following general anaesthesia and tracheal intubation, among which 16 cases exhibited a difficult airway, including four cases where tracheal intubation was not possible requiring urgent tracheostomy (figure 1). In the present study, 54 cases of haematoma were successfully treated, and the patients were subsequently discharged from the hospital. Regrettably, one patient died due to complications 24 days following the evacuation surgery.
In the comparison between difficult intubation patients and non-difficult intubation patients, there were statistically significant differences in retropharyngeal haematoma, the interval between symptom onset and airway intervention and hospitalisation duration (table 3). Binary logistic regression analysis revealed that retropharyngeal haematoma (OR 10.435; 95% CI 1.249 to 87.144; p=0.030) was an independent risk factor for difficult intubation. The AUC for retropharyngeal haematoma was calculated to be 0.674 (95% CI 0.529 to 0.819; p=0.044). To evaluate the strength of the association between retropharyngeal haematoma and difficult intubation, the phi coefficient was used. The analysis revealed a phi value of 0.342 (indicating a moderate positive correlation, as values between 0.3 and 0.5 are generally considered moderate), with a p value of 0.011.
Comparison between the difficult intubation group and the non-difficult intubation group in the haematoma patients
Discussion
Incidence and time of presentation of postoperative haematoma
Postoperative haematoma following ACSS is a rare but potentially high-risk complication. Bovonratwet et al reported that out of a total of 37 261 patients who underwent anterior cervical discectomy and fusion, 148 (0.40%) developed haematoma requiring reoperation.1 In a single-surgeon case series of ACSS, Wang et al documented a 1.0% incidence of postoperative haematoma, affecting 11 individuals out of a total of 1150 patients. Notably, among these haematoma cases, 10 were specifically classified as retropharyngeal haematoma.8 Miao et al presented a cohort of 1258 patients who underwent ACSS, revealing an incidence of postoperative haematoma totalling 1.2%. Specifically, they observed seven cases (0.5%) of retropharyngeal haematoma and eight cases (0.6%) of spinal epidural haematoma.2 Boudissa et al reported that 13 out of 2319 patients (0.56%) undergoing ACSS required reintervention within 72 hours postoperatively, with a distribution of five cases (0.2%) of retropharyngeal haematoma and seven cases (0.3%) of spinal epidural haematoma.9 O’Neill et al reported on a series of 2375 ACSS procedures, documenting 17 occurrences of retropharyngeal haematoma, which corresponded to an incidence of 0.7%.5 In the present study, the overall incidence of haematoma was 0.4%, with retropharyngeal haematoma occurring at a rate of 0.28% and spinal epidural haematoma at 0.12%, which is consistent with previous literature reports.
The common clinical assumption is that the risk of haematoma is most pronounced in the initial hours following surgery. Nevertheless, O’Neill et al noted that approximately 35% of cases presented with a delayed onset, with an average time frame of 6 days, postoperatively.5 In the present study, 31 cases exhibited symptoms within the first 6 hours postoperatively, with the earliest symptom onset occurring immediately after awakening from anaesthesia. Additionally, 8 cases presented symptoms beyond 24 hours postoperatively, with the longest interval being 7 days.
Risk factors for postoperative haematoma
Previously described risk factors for haematoma, including male sex, age older than 65 years, smoking, medical comorbidities, multilevel procedures, OPLL within the surgical segments, therapeutic heparin use, lower BMI and ASA physical status classification grades of III or greater,1 2 5 8 10–13 were not found to show strong associations in our study. The type of cervical spondylosis, as well as preoperative scores on the m-JOA and NDI scales, did not influence the occurrence of postoperative haematoma.
In previous studies, prolonged TT values and INR greater than 1.2 were identified as independent risk factors of haematoma.1 8 Prolonged APTT was associated with an increased risk of haematoma formation after surgery.14 In clinical practice, an extension of APTT by 10 s is considered to have clinical significance. However, in the present study, the mean values of APTT in both the haematoma group and non-haematoma group were within the normal range. Therefore, despite the statistically significant difference in APTT between the two groups, the prolonged APTT in the present study should not be construed as a risk factor for haematoma development.
ACCF surgery exposes at least three vertebral bodies, resecting two intervertebral discs, while also performing partial vertebral body resection, which leads to greater exposure of the epidural space and extensive damage to the venous plexus within the spinal canal, resulting in increased blood loss. Hao et al reported that among a total of 551 patients who underwent anterior cervical discectomy and fusion or ACCF for 2-level cervical spondylotic myelopathy, a significant difference was observed between the two groups in terms of blood loss.15 In the current study, logistic regression analysis suggested that ACCF was an independent risk factor for postoperative haematoma. During the ACCF surgery, special attention should be paid to potential bleeding, including vessels, muscles and exposed cancellous bone.
Hypertension is recognised as a significant risk factor for postoperative haematoma, although the underlying mechanisms are not fully defined.16 Liu et al suggest that arterial bleeding was predominantly the cause of such haematomas.17 However, Yin and Ni present an alternative view, contending that arterial bleeding is an unlikely major source of haematomas due to its detectability during surgical procedures.18 During the initial intraoperative period under anaesthesia, the MAP is low, making small vessel bleeding potentially undetected and inadequately managed with bipolar coagulation. As patients emerge from anaesthesia, the stimulation of the tracheal tube and postoperative pain may precipitate a rise in blood pressure. These small vessels, which have not achieved effective haemostasis, may resume bleeding, leading to the development of haematoma. In the present study, the MAP at admission showed no significant difference between the two groups, yet a statistically significant difference was observed in the maximum MAP during the recovery period. Haematoma commonly occurs within the first few hours postoperatively. Haemodynamic fluctuations, particularly the surge in blood pressure during the anaesthetic recovery period, may play a critical role in the development of haematoma, and thus, close monitoring and management of blood pressure during this period could be essential in reducing the risk of postoperative haematoma.
Optimal timing for evacuation and airway management in haematoma patients
For patients with spinal epidural haematoma accompanied by severe neurological deficits, emergent surgical evacuation of the haematoma is the most appropriate therapeutic approach. The severity of symptoms prior to surgery may significantly impact postoperative recovery. According to the study by Yin et al, there was a significant statistical difference in the degree of neurological recovery based on whether the spinal epidural haematoma was evacuated within 24 hours.18 The research by Hohenberger et al indicated that the key factors influencing recovery were the degree of neurological deficit and the interval between the onset of symptoms and surgery.10 Similarly, Epstein and Agulnick advocated for aggressive treatment of postoperative spinal epidural haematoma.19 In the present study, all 17 patients with spinal epidural haematoma underwent evacuation surgery, and all patients’ symptoms were partially or completely relieved after the procedure.
Song et al reported that patients with retropharyngeal haematoma could be treated with close observation or evacuation surgery, depending on changes in respiratory status, surgical site conditions and patient behaviour.4 However, O’Neill et al believed that whenever a patient presented with an airway complication, the decision was made to reoperate rather than treat the patient with observation and steroids.5 In the management of retropharyngeal haematoma, it was crucial to acknowledge the potential risk of difficult airways.20 In the current study, among the 55 cases of haematoma evacuation, 16 patients encountered difficult intubation conditions, with four ultimately requiring a tracheostomy. In the subgroup analysis, retropharyngeal haematoma was identified as an independent risk factor for difficult intubation. Of the 16 difficult intubation cases, 15 were attributed to patients with retropharyngeal haematoma. The thyroid haematoma management guidelines emphasised the importance of anticipating difficult airway scenarios in patients with cervical haematomas.21 In our study, 29% of haematoma patients experienced difficult intubation, irrespective of the haematoma’s location. Therefore, in the airway management of these patients, anaesthesiologists should adhere to the ASA practice guidelines for management of the difficult airway,6 and the following measures should be considered: (1) awake intubation, (2) use of video laryngoscopy for the first intubation attempt, (3) limitation of tracheal intubation attempts and (4) preparation for emergency front-of-neck airway.
This study presents a substantial clinical series dedicated to investigating haematoma following ACSS and introduces a novel finding by identifying, for the first time, ACCF and maximum MAP during recovery as independent risk factors associated with postoperative haematoma. In this retrospective nested case-control study, matching criteria such as the same surgeon, same year of surgery, same gender and similar age (±5 years) were applied to ensure a high degree of homogeneity and minimise bias. Despite these efforts, this study has its limitations. First, as with any retrospective study, there is an inherent risk of selection and reporting bias. Second, due to the low incidence of haematoma, the sample size is limited. A multicentre, prospective study with a more detailed assessment of risk factors might provide a more comprehensive understanding of the variables associated with postoperative haematoma following ACSS.
Conclusion
ACCF and elevated maximum MAP during the recovery period were independent risk factors for postoperative haematoma following ACSS. Patients with post-ACSS haematoma are at high risk of a difficult airway, with retropharyngeal haematoma being strongly associated with challenging airway management. Postoperative haematoma was associated with longer hospitalisation duration and greater costs.
Data availability statement
Data are available in a public, open access repository. The data underlying this article are available in Mendeley Data Repository, at https://data.mendeley.com/datasets/6rx5wgp75p/1.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by Medical Scientific Research Ethics Committee of Peking University Third Hospital. IRB number: IRB00006761-M2024464, 2022.06.05.
Footnotes
X @alicelj_anes
YT, JL and GZ contributed equally.
Contributors YT, JL and GZ contributed equally to this paper. The corresponding authors are XG (puthmzk@163.com) and YH (hanyongzheng@bjmu.edu.cn). MX, ML, JW, SW and XG designed and coordinated the study. YT, GZ and YQ collected the data. YT, MW and YH drafted the manuscript. YT and JL analysed the data and performed the statistical analysis. All authors have read and approved the manuscript. YT is the guarantor of this study and takes responsibility for the overall content and integrity of the work.
Funding This study was funded by grants from Wu Jieping Medical Foundation (320.6750.2023-08-5), Capital's Funds for Health Improvement and Research (2024-2-40912) and Peking University Third Hospital Innovation and Transformation Fund (BYSYZHKC2022103).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.