Article Text

Abstract
Introduction Multiple sclerosis (MS) is a chronic disease of the central nervous system that impacts millions worldwide, including individuals in Iran. It primarily affects young people, leading to biopsychosocial challenges with unpredictable symptoms. Self-management is crucial but challenging due to the lack of definitive treatment. New approaches, such as mHealth interventions, particularly gamification, aim to engage patients more effectively. Well-designed gamification may positively impact health behaviours and enhance collaborative care. However, its implementation in the field of MS in Iran is currently limited. So far, some mobile applications have been designed that do not incorporate gamification principles and only focus on one issue. These applications also fail to consider the family caregivers' understanding of the patient’s condition. Therefore, this study aims to investigate the impact of family-oriented gamification on the self-management of Iranian patients with MS.
Methods and analysis We propose a mixed-methods study with an exploratory sequential design consisting of a qualitative phase, gamification development and a dual-centre, prospective, single-blinded, parallel-group randomised controlled superiority trial. In the qualitative phase, data will be collected through purposive sampling via semistructured interviews with patients until data saturation is reached. Concurrently, the data will be analysed using conventional content analysis to provide insights into the patients’ self-management challenges. Next, web-based and card gamification will be developed for patients and their families based on the findings of the qualitative phase. Ultimately, the effectiveness of these interventions will be evaluated through a randomised controlled trial. The preliminary literature suggests an initial sample size of 25–30 participants per group for this phase. After enrolling approximately 10 participants, the exact sample size will be recalibrated using G-Power software based on data analysis. Participants will then be randomly assigned to either the intervention or control group in a 1:1 ratio. Allocation concealment will be ensured using mixed block sizes of 2 and 4. The primary outcome, self-management, and the secondary outcome, self-efficacy, will be assessed both before and immediately after the intervention. Furthermore, the usability of the two gamification strategies will be evaluated following the intervention.
Ethics and dissemination This study is part of a doctoral thesis approved by the Tehran University of Medical Sciences Research Ethics Board (IR.TUMS.FNM.REC.1401.185, 23 February 2023). Dissemination of findings will occur at the local, national and international levels.
Trial registration number IRCT20240116060708N1.
- Multiple sclerosis
- Self-Management
- eHealth
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study is centred around developing gamification for patients with multiple sclerosis and their families by using patients’ data and their expected outcomes, specifically tailored to the social context of these patients.
A randomised design is incorporated into this study to guarantee that both intervention and control groups are given equal opportunities.
Weekly phone call follow-ups may be conducted to promote the use of gamification and potentially improve adherence to the interventions.
Due to the financial limitations, the two-dimensional animations in patients’ gamification may affect the program’s appeal.
Internet access is a requirement for users of the web-based gamification program.
Background
Multiple sclerosis (MS) is a chronic and degenerative disease of the central nervous system. According to the latest MS disease atlas report in 2023, nearly 2.9 million people worldwide1 and 75 000 in Iran have this disease.2 MS typically occurs in young individuals and is relatively associated with a normal lifespan. The disease can cause physical, mental and emotional problems. The occurrence and worsening of these symptoms are unpredictable, and if not controlled properly, they can lead to more severe complications.3–5
Since there is no definitive treatment for this disease yet, the affected person must take measures to promote self-management throughout the disease.6 Self-management involves actively adapting to the disease by adhering to treatment, practising self-care, seeking information about the disease and treatment, and maintaining social connections.7 Promoting self-management is closely tied to self-efficacy, which is an individual’s belief in their ability to perform behaviours that lead to specific outcomes. When patients engage in self-management, they improve their understanding of disease symptoms and learn effective lifestyle modification strategies. This empowerment enhances their self-efficacy as they realise their ability to influence their health. As patients experience improved physical and emotional well-being, their confidence in managing their condition grows, creating a positive feedback loop that encourages ongoing self-management.8 9
Regardless of the level of dependence of the patients on their families, self-management of the disease is a two-way street that requires the support of family members as well.7 It is important to note that promoting health behaviours begins with the patient’s efforts and is further enhanced by family support.10 Studies have shown that family-based interventions have been more effective in improving health outcomes.11 12
Various methods are used to enhance patients' self-management. These methods include offering support programs, counselling, encouraging patients to make lifestyle modifications, maintaining ongoing communication and teaching life skills.13 Various educational strategies have been employed to foster patients' self-management, such as in-person training, distributing booklets and pamphlets, and group training.14 15 However, these approaches have limitations such as lack of easy access and high workload for health workers. Additionally, challenges like lack of time, patients’ unfamiliarity with educational concepts, disruptions by patients’ companions, boring content and non-compliance with care plans have been reported.16 Conventional educational approaches often have a one-dimensional structure, limited to face-to-face or written communication, which may struggle to effectively motivate self-management behaviours.17
Recently, health promotion interventions using new approaches such as mHealth have been able to achieve positive results.18 One of the most commonly used methods in this field is the development of mobile phone applications. Available statistics show that more than 85% of patients with MS are smartphone users who use their devices to manage their disease.19 According to available statistics, at the beginning of 2024, there were over 73 million internet users in Iran, with mobile phone connections equivalent to 163.7% of the total population.20 This means there is, on average, more than one mobile connection per person, suggesting that many may own multiple lines. These statistics highlight the widespread use of smartphones among the general population of Iran, including individuals with MS. However, many of the smartphone programs have failed to effectively meet the needs of patients and care requirements, as well as to attract active patient participation. This is often because they are focused on the perspective of health providers and do not take into account the perspective of patients.21 Regardless of the progress made in providing care to patients and educating them, programs that do not engage patients and families actively will likely yield inappropriate outcomes and waste resources.22
Effective gamification implementation begins with identifying goals and understanding the target audience.23 Engaging game elements should be selected, and user experiences designed to incorporate feedback that motivates participation.24 25 Appropriate technology must be chosen, whether using existing platforms or developing custom solutions. Regular testing and small-scale pilots are essential for refining the experience.26
By using a patient-centred approach, gamification has the potential to incentivise individuals to engage in disease management and adopt healthier behaviours, particularly for chronic conditions.27–32 This method involves incorporating game elements into non-game settings, and transforming routine health tasks into interactive activities.33 Such an approach addresses common challenges faced by traditional programs by generating motivation and encouraging participation.34 35
For instance, by understanding the target audience and employing game mechanics like points, badges and leaderboards, gamification can encourage patients to participate more actively in their health management. Moreover, this approach may foster meaningful challenges that resonate with users and promote a sense of achievement. Patients may find themselves more motivated to engage in health-related activities, such as medication adherence and tracking symptoms while gaining autonomy and accountability over their health outcomes.36
Additionally, gamification has been shown to improve individuals' retention and application of information.37 The effectiveness of gamification is influenced by its psychological context; therefore, it is essential for researchers to familiarise themselves with the informal and personal contexts of participants to design suitable gamification strategies.38 Since patients with the same diagnosis and treatment may have entirely different experiences, examining these experiences before designing an intervention is crucial.39
However, empirical evidence regarding the effectiveness of gamification is conflicting. A systematic review suggests that gamification may be ineffective,36 while a separate meta-analysis indicates that gamification interventions can effectively change health behaviours and outperform other behaviour change methods.40 Given the current limited knowledge about family-centred gamification in patients with MS, conducting only quantitative research is insufficient for a deep understanding of the phenomenon. This methodology often lacks a strong grasp of the research context and does not capture the voices of the participants directly.10 41 42 In contrast, qualitative research allows for a better understanding of the phenomenon by focusing on natural events in participants' environments, offering a scientific approach to describing life experiences from their perspectives.43 Therefore, the most appropriate method for designing gamification is to conduct studies using a combination of quantitative and qualitative methodologies.
In the existing literature, a lack of evidence regarding the effects of different types of gamification on health behaviours in MS, especially in Iran, has been identified. Considering the increasing number of individuals suffering from MS, there is a significant need for self-management promotion interventions and support for these patients from their families.
Methods and analysis
Study aim
The present study is designed to investigate the impact of family-oriented gamification on the self-management of people with MS. More specifically, this mixed-method study aims to (1) explain the experiences of people with MS from the challenges of self-management of this disease (qualitative), (2) design and develop web-based gamification for patients based on the challenges raised (intervention development), (3) design and develop card gamification for families based on patients' expectations (intervention development) and (4) investigate the effect of the gamifications on patients' self-management and self-efficacy compared with usual care (quantitative). Also, this study addresses the following research questions:
What challenges do patients with MS experience in self-management?
Are there differences in self-management behaviour between patients with MS who receive gamification and those who receive usual care?
Are there differences in self-efficacy between patients with MS who receive gamification and those who receive usual care?
It is hypothesised that the health-related behaviours of people with MS who participated in the developed gamification will differ from those of patients who received usual care. Specifically, we will examine variations in areas such as disease knowledge, peer support engagement, family support, communication with healthcare providers, medication adherence, physical activity levels, fatigue management and dietary choices.
Study design
According to the aim of this study, an exploratory sequential mixed-methods design with connected integration is being used. The study includes a qualitative phase to identify self-management challenges faced by patients with MS to develop gamification, followed by a randomised controlled trial (RCT). A flow diagram of the study procedures is shown in figure 1 according to Creswell.42 The methods for the qualitative and quantitative components are described here separately. The protocol for this mixed study is reported based on the Good Reporting of A Mixed Methods Study checklist (online supplemental file 1).44
Supplemental material

Design of this exploratory sequential mixed-method study. The figure illustrates a sequential mixed-method study design, beginning with qualitative data collection through purposive sampling and semistructured interviews. Findings from this phase guide the development of gamification strategies, which are further refined based on expert panel feedback. The study then advances to the creation of web-based and card-based gamification tools tailored for patients and their families. Finally, a randomised controlled trial (RCT) is conducted to collect and analyse quantitative data, assessing the interventions' effectiveness in improving self-management and self-efficacy among patients with multiple sclerosis (MS).
Qualitative component: conventional content analysis
According to the purpose of this stage, which is to explain the experiences of people with MS from the challenges of self-management of this disease, the approach of qualitative conventional content analysis will be used without imposing predetermined categories.45
Participants and setting
Individuals with MS who meet the inclusion criteria—being diagnosed with any type of MS (Relapsing-Remitting, Primary Progressive, Secondary Progressive, or Progressive-Relapsing), aged between 18 and 60, receiving treatment at an MS clinic, being able to read and speak Persian, and willing to share their experiences—will be selected through purposive sampling. Participants will represent diverse demographics, including variations in gender, education level, disease duration, and complications, and will be recruited from MS clinics located in Tehran and Ardabil, Iran.
Data collection and analysis
Data collection will be done through in-depth interviews with open-ended questions in an unstructured manner, followed by a semistructured approach by the primary author under the supervision of the research team. The interview questions are developed based on relevant literature that highlights the specific challenges patients face in coping—a crucial factor in both quality of life and self-management46–48—as well as the professional insights of the researchers. Participants will be asked to ‘Share their experience with MS disease’, ‘What challenges have they faced since being diagnosed’ and ‘How do they address them?’ Throughout the interviews, participants will be prompted with probing questions. After each interview, participants will be allowed to share any additional information they feel is important. The interviews will take place face-to-face in a quiet environment, with no other individuals present.
The conventional content analysis method was used by following the five steps proposed by Graneheim et al 49 for data analysis: (1) transcribing the entire interview immediately after each interview, (2) reading the entire text several times to gain an overall understanding of its content, (3) determining semantic units and basic codes, (4) classifying primary codes into more comprehensive categories and (5) determining the main theme of categories. The data collection will continue until data saturation is reached. MAXQDA10 software will be used to handle the large volume of data. It is noteworthy that data collection and analysis will be done concurrently.
Trustworthiness
Lincoln and Goba criteria will be used to ensure the quality of the study.50 Study credibility will be established through prolonged engagement with participants and data, allocating sufficient time for data collection, building trust-based relationships with participants and incorporating their feedback. Dependability will be ensured through research auditing and data control by independent authors, and the extracted codes will be reviewed by the research team. Then, the categories will be compared with each other, and any disagreement will be resolved through discussion. Moreover, several interviews will be randomly selected and given to some external researchers to review the data and share their comments and feedback. Confirmability and authenticity will be guaranteed by presenting quotes extracted from each interview. Transferability will be enhanced by detailing the entire research process, all participants’ characteristics, and research context, and by selecting participants with maximum diversity from two distinct cities, which will also help other researchers to follow the research procedure.
Data integration
The data obtained from this phase will connected with the gamification development phase of the study. In exploratory sequential studies, data integration is when the next stage of research is based on the data obtained from the previous stage.42
In this phase of the research, a panel of experts will be formed, consisting of gamification specialists, medical education and nursing professors, specialists in neurological diseases and nurses working in the neurology department. By examining the categories extracted from the analysis of the interviews, a decision will be made regarding the dependent variables involved in the self-management of the disease that can be manipulated through gamification in the next phase of the study. The prioritisation of the main categories extracted from the interviews will be based on the opinions of experts and research participants. Additionally, decisions will be made about how to design gamifications and their characteristics based on the findings of the qualitative stage.
At this stage, two types of gamifications will be designed and their validity will be checked.
Study interventions
The intervention in this research includes both web-based gamification for patients and card-based one for their families. The co-design element will involve input from patients to ensure that the designs are user-friendly and relevant to their experiences (figure 2).

Theoretical model of the gamification Intervention for patients with multiple sclerosis (MS) and their families. This figure illustrates a conceptual framework for a gamification-based intervention designed to support patients with MS and their families. The framework integrates two distinct gamification strategies: web-based and card-based approaches. These strategies aim to enhance patients’ understanding of MS, address their specific needs and facilitate effective care. The model highlights three targeted domains—cognitive, affective and psychomotor—focusing on areas such as disease knowledge, emotional engagement and self-management skills. In essence, this framework provides a holistic structure for implementing gamification interventions to empower patients with MS and their families.
Web-based gamification for patients
The planned intervention for patients will be a web-based gamification reported based on the Consolidated Standards of Reporting Trials of Electronic and Mobile Health Applications and Online Telehealth (online supplemental file 2). Building on the findings from the prior qualitative phase of the study and the personal life stories of individuals living with MS, these narratives will be integrated into a gamified format. This approach aims to highlight the challenges of self-managing the disease while fostering behaviour change across the cognitive, affective and psychomotor domains of Bloom’s taxonomy.51
Supplemental material
Following the analysis of qualitative data and the identification of main categories, their alignment with Bloom’s learning domains will be evaluated. Each category will be mapped to its corresponding domain, and engaging challenges will be developed in the form of games. Gamification will address various challenges faced by participants, including physical issues like fatigue, mobility limitations and pain; psychological factors such as cognitive impairments and emotional instability; as well as social issues like isolation and alienation associated with MS.
Participants will face cognitive challenges aimed at enhancing critical thinking by deepening their understanding of autoimmune diseases, recognising relapse symptoms, identifying risk factors and developing problem-solving skills to adapt to life with MS. In the affective domain, engaging emotional narratives will immerse participants, fostering empathy for those living with MS, building emotional resilience and inspiring hope while promoting a positive lifestyle. For the psychomotor domain, hands-on, interactive activities simulating real-life scenarios will help participants develop effective self-management strategies, such as maintaining a proper diet, adhering to medication schedules and managing fatigue. Additionally, they will strengthen their communication skills by sharing experiences and discussing disease-related topics with others.
The gamification is being developed by a licensed game company. Patients who provide informed consent (online supplemental file 3) will receive a Short Message Service containing a username and password to access a secure online portal. Through this portal, they will complete interactive, game-based assessments designed to address the challenges of their illness and self-management. By incorporating gamification, the initiative aims to foster active engagement and encourage the sharing of personal experiences. These assessments will focus on topics such as understanding their condition and the impact of lifestyle choices on overall health.
Supplemental material
On entering the program, users will be guided to the main menu. Selecting the ‘Start’ option will initiate animated life stories in Persian. During the animations, challenges will arise based on variables identified during the integration phase by the research team. Completing each challenge will earn users points and provide educational content. Advancing through the stages will lead users to the game’s conclusion. As points accumulate, users will level up and unlock special badges. Additionally, members of the intervention group can access a forum and chat room within the program to connect with other patients or health service providers. Due to the nature of the study, product design has not yet begun, and demo pages have not been created.
Face and content validity of the web-based gamification
To assess face validity, five patients52 53 will be asked to participate in the gamification daily for 2 weeks.54 Follow-up phone interviews will be conducted 2 weeks after their initial participation to collect feedback on the program’s clarity, motivational aspects and overall satisfaction. This method enables us to directly determine whether the program is relevant and understandable to users—key components of face validity. By integrating their feedback and suggestions, we aim to enhance the program further, ensuring it aligns with the expectations and needs of our target population.
The content validity of the program will be assessed in terms of relevance, clarity and essentiality by presenting it to nursing professors, gamification specialists, neurologists, psychologists and nurses from the neurology department. It is suggested that essentiality be assessed using the content validity ratio (CVR), with a minimum CVR of 0.90 calculated from five experts required to retain each item.55 After all amendments have been applied, the final version will be prepared.
According to a similar study,56 patients will participate in this game for nine sessions lasting 30 min each, spread out over 3 weeks (three times a week). To ensure that the number of game sessions does not decrease, a 4-week period will be considered to guarantee that patients complete all nine sessions. The frequency and duration of patient use of gamification will be detectable. If a patient misses a session, the research team will follow up with them by phone to ensure compliance with the intervention.
Card gamification for families
The family intervention will be delivered through a card-based gamification approach, designed to narrate patients’ stories while empowering family members to provide optimal care. Through this interactive format, family members will gain insights into the challenges faced by patients and their own caregiving responsibilities, all while engaging in a competitive and educational experience. Drawing from patient expectations for home caregivers identified during the qualitative phase, the research team will select key variables and create educational content in the form of questions and answers. The gamification package will include a game board with designated role-specific fields, two pawns, a bell, a die, question cards, chance cards, a gold card, coins, a medal and a comprehensive guide. All components will be neatly housed in a specially designed box.
Two family members will compete in this interactive game. The game board, along with all cards and a bell, will be set up on the table. Players will begin at the designated starting point and progress along the path based on dice rolls, stopping at each space to complete the assigned task. Tasks may include answering questions, drawing chance cards or taking a rest. Each question card will display a question on the front and its answer on the back. On landing on a question space, a player will draw a card and read the question aloud. The first player to ring the bell gets the chance to answer. A correct answer earns coins, while an incorrect answer results in losing a turn. The first player to reach the finish line wins the game.
In family gamification, participants will boost their critical thinking and knowledge retention on vital topics related to caring for patients with MS. Its competitive nature will promote teamwork and communication skills, while also strengthening family bonds and enhancing overall interaction.
Face and content validity of the card gamification
Gamification will be evaluated by participants for face validity. A preliminary sample of the gamification will be presented to 10 family members of patients over 2 weeks. Feedback will be collected and summarised at the end of each week. The feasibility of the gamification will be determined based on the absence of reported issues during participation, its clarity, ability to motivate and overall participant satisfaction.
To ensure the content validity of the gamification in terms of relevance, clarity and essentiality, it will be presented to nursing professors, gamification specialists, neurologists, psychologists and nurses from the neurology department. It is recommended that essentiality be evaluated using the CVR, with a minimum CVR of 0.90 calculated from five experts needed to keep each question.55 After all amendments have been applied, the final version will be prepared.
The gamification package will be provided to the families in the intervention group, and they will be asked to play it at home by forming a team of two with fixed members. Based on a similar study,52 families will play up to six sessions lasting at least half an hour over 3 weeks (twice a week on Mondays and Fridays). Family members will be followed up with phone calls on Tuesdays and Saturdays to ensure their compliance.
Quantitative component: RCT
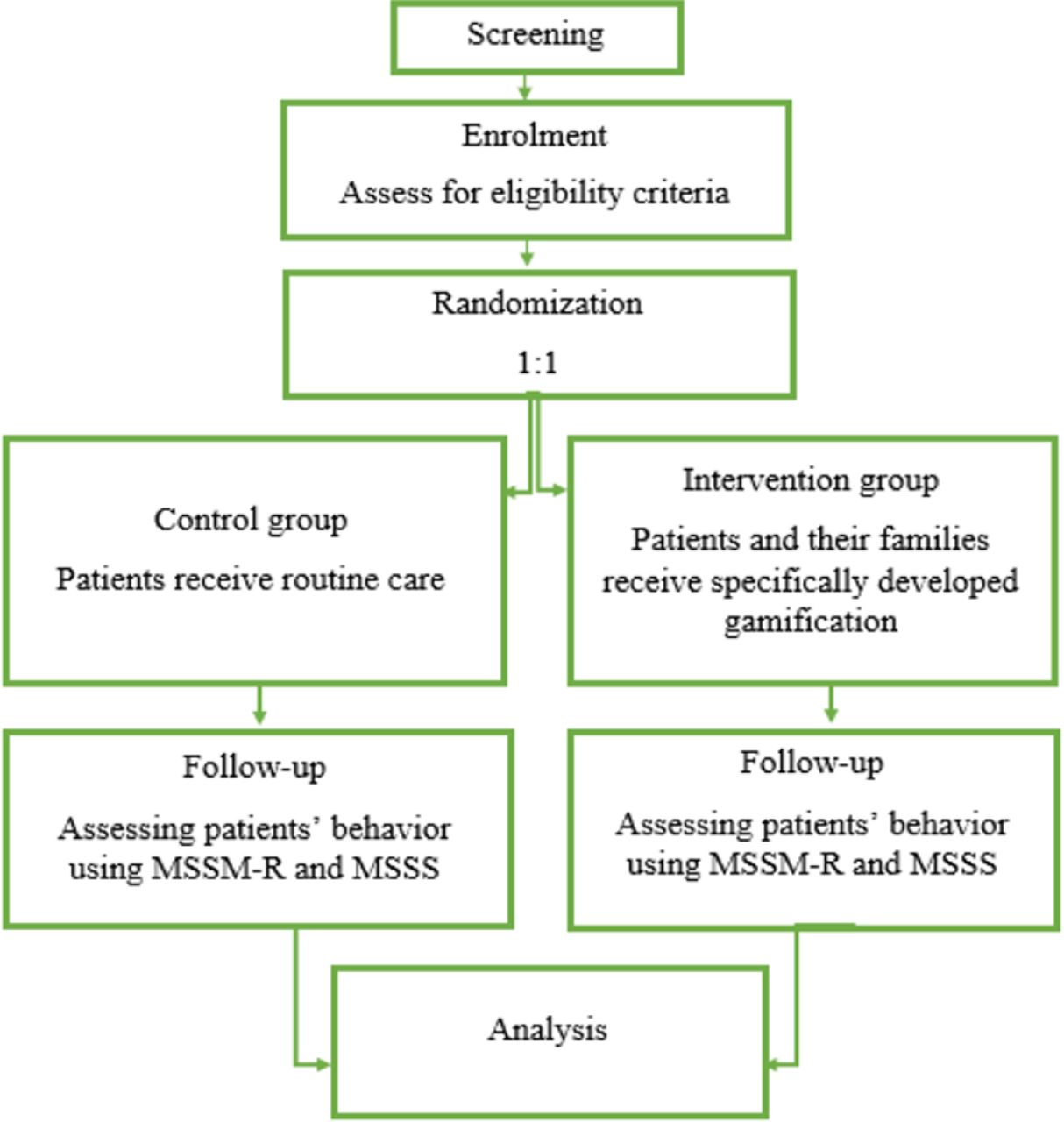
This will be conducted as a dual-centre, parallel-group, randomised controlled superiority trial (figure 3). The protocol for this trial was written in accordance with the Standard Protocol Items: Recommendations for Interventional Trials reporting guidelines (online supplemental file 4). 80 eligible participants will be selected from patients referred to the MS clinic or a physician’s office in Tehran and Ardabil city (Iran). The criteria for patient inclusion in the study are as follows: individuals aged 18–60, diagnosed with one of the MS types, owning a smartphone/tablet, able to read and write in Persian and demonstrating the willingness to participate in the study.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Flowchart of randomised controlled trial phase. The flowchart outlines the essential steps in the randomised controlled trial phase of the study. The process begins with participant screening, followed by enrolment and evaluation of eligibility criteria. Eligible participants are then randomly allocated to either the control group, where patients receive standard care, or the intervention group, where patients and their families engage with a specially designed gamification program. Post-intervention, both groups complete follow-up assessments to measure patient behaviour using the MS-revised self-management tool (MSSM-R) and Multiple Sclerosis Self-Efficacy Scale (MSSS). The collected data are subsequently analysed to assess the effectiveness of the gamification intervention.
Family members will be eligible for inclusion if they serve as caregivers for the patient, are aged 18–60, can read and write in Persian, and are willing to take part in the study.
Patients will be excluded from the study if they have visual, hearing or speech impairments that hinder the use of gamification, health issues that impede communication, and lack a caregiver.
The primary author of the study will obtain informed consent from eligible patients. Individuals will then be randomly assigned to either the control or intervention group in a 1:1 allocation ratio. Baseline data will be collected before exposing the intervention group to gamification. Post-test data will be collected afterwards.
In the intervention group, patients and their families will receive the developed gamifications simultaneously for a period of 3 weeks. Participants, including patients and their families, are strongly advised not to use other educational programs available on the internet or information sources such as books related to the disease while taking part in this research.
The control group, on the other hand, will receive routine care during this same time frame. Routine care includes both oral and written education that is provided to patients and their families in both the clinic and inpatient department as well as on-line materials.
Risks and consent
This trial is deemed to be safe as it is exclusively educational in nature, involving no physical interventions. The benefits and potential risks associated with the study are clearly outlined in the informed consent document. Participants will be thoroughly informed about the study’s objectives, the nature of the intervention, the anticipated benefits and any possible risks involved. Additionally, participants will receive contact information for the research team, enabling them to report any concerns or issues that may arise during their participation in the program.
Sample size
The estimated sample size, based on prior literature due to the lack of a directly related study,57–59 is projected to range from 25 to 30 participants per group. Following the enrolment of approximately 10 participants, G-Power software will be used to refine the sample size calculation, informed by the preliminary results. This approach ensures a precise and well-founded determination of the study’s required sample size.
Potential participants who are being referred to the MS clinic or a physician’s office will be selected and contacted based on the inclusion criteria. They will receive a letter via one of the social messengers that explains the purpose of the study, time commitments, risks, potential benefits and contact information for the study staff. Within the next 3 days, the potential participant will be contacted and asked about their decision. If the patient and their family decide to participate in the study, the location and time of the meeting will be coordinated to provide training on how to use both gamifications.
Randomisation, allocation concealment and blinding
Participants will be randomly assigned to receive gamification interventions in a 1:1 ratio. To ensure a balanced distribution of participants across groups, patients will be classified based on key variables that significantly impact MS, such as gender, age and type of MS. This approach will help ensure that there are no significant demographic differences between groups. Specifically, participants of the same gender, and type of MS, and within a similar age range will be randomised together.
The randomisation and allocation of treatments were centralised, using randomly mixed block sizes of 2 and 4. The primary investigator will generate blocks of 4, designated by letters A and B, representing the intervention and control groups, respectively. Six possible sequences—AABB, ABAB, ABBA, BAAB, BABA, and BBAA—will be created and securely stored in a closed container under the supervision of the primary investigator. To further ensure concealment, block sizes of 2 will also be employed. For instance, a block may be structured as ABAB, indicating that the first participant will be assigned to the intervention group, the second to the control group, the third to the intervention group, and the fourth to the control group.
Due to the nature of the intervention, blinding participants is not possible.60 Since gamification is observable and does not include a placebo, patients will be informed of their group assignment (control or intervention). To minimise bias, an independent individual, not involved in administering the intervention, will manage data collection and analysis. This single-blind approach ensures that investigators responsible for data handling and statistical evaluation remain unaware of group assignments.
Outcome measure and data collection
Primary and secondary outcomes will be measured for all participants in person at the study’s outset just after randomisation (for baseline data) and again immediately after the finishing of the exposure period for the last person in the intervention group. The primary outcome will be the differences between the two groups in their self-management behaviour. The secondary outcome will be group differences in self-efficacy. In addition, usability of these gamifications will be measured after intervention.
Patients’ data for self-management will be collected using the MS-revised self-management tool (MSSM-R), consisting of 24 items and 5 subscales, designed by Bishop and Frain.61 The subscales include communication and relationship with healthcare providers (items 9, 12, 14, 16, 18 and 20), treatment adherence/overcoming obstacles (items 11, 15, 17, 21, 22, 23 and 24), social/family support (items 6, 10 and 13), information and knowledge about MS (items 1, 2, 3 and 4) and health maintenance behaviour (items 5, 7, 8 and 19). The questionnaire is scored on a 5-point Likert scale (1=completely disagree to 5=completely agree). A higher score indicates a higher level of self-management, except for questions 21, 23 and 24 which are reverse-scored. The total score range on this tool is between 24 and 120. Saadat et al demonstrated in their study that the internal consistency of all subscales of the MSSM-R in Iran, as measured by Cronbach’s alpha and test-retest reliability, ranged between 0.71 and 0.89.62
Data for patients’ self-efficacy will be collected using Multiple Sclerosis Self-Efficacy Scale (MSSS). It was developed by Rigby and colleagues63 and consists of 11 items and 3 subscales: independence and activity (items 5, 6, 10 and 11), self-control (items 1, 4 and 9) and concern and interest (items 2, 3, 7 and 8). Each item is scored on a 6-point Likert scale (strongly disagree=1 to strongly agree=6). Items 2, 3, 7, 8 and 11 are reverse-scored. The total score of the scale is calculated by summing the scores of the three subscales. Higher scores in each subscale indicate a better status in that area. In a study by Tanhaye Reshvanlo and Soleimanian,64 Cronbach’s alpha with a range of 0.78–0.90 for the MSSS dimensions indicated the positive reliability of the scale in the Iranian population.
The GAMEX, a self-report scale developed by Eppmann et al, 65 will be used to measure participants’ gameful experiences. It consists of 27 items scored on a 7-point Likert scale (1= ‘strongly disagree’ to 7= ‘strongly agree’). It is divided into six variables: enjoyment (six items), absorption (six items), creative thinking (four items), activation (four items), absence of negative affect (three items) and dominance (fiyr items). Three items of the absence of negative affect are reverse-scored.
Statistical analysis and data management
Each participant will be assigned a unique study identifier and initial, ensuring anonymity and confidentiality. A password-protected electronic document will be established to store all relevant information for statistical analysis. The analysis will be conducted by the primary investigator in collaboration with a designated experienced team member. Statistical analysis will be conducted using IBM SPSS V.21, with a two-sided significance level set at 5%. Data entry will be performed in duplicate and validated through range checks to ensure accuracy. Outcome measures will be analysed following the intention-to-treat principle. Additionally, outcomes such as program adherence, session completion rates, and dropout rates will be assessed.
Participants' gameful experiences will be summarised using descriptive statistics. Comparisons of participant characteristics between the two groups will be conducted using two-sample independent t-tests, χ² tests, or Fisher’s exact tests, as appropriate.
The Data Monitoring Committee, consisting of both internal and external reviewers, will evaluate the data to ensure compliance with ethical and scientific standards. The collected data will be submitted to these reviewers at various stages of the research process for continuous assessment and feedback.
Patient and public involvement
We will actively involve individuals with MS and their families in shaping and validating gamification strategies to better understand the challenges they face in self-management. Members of the MS community will work closely with us to co-design the gamification elements, ensuring the intervention is practical, culturally sensitive and meaningful. Throughout the study, we will maintain consistent communication with our patient partners, providing regular updates and seeking their feedback at key milestones.
Trial status
We have recently registered the RCT with the Iranian Registry of Clinical Trials. The sampling for the RCT has not yet begun. Sampling for the qualitative phase of the study started in early 2024 and is currently ongoing. It is expected to be completed by 1 October 2024, at which point the intervention will be designed. Sampling for the clinical trial phase will begin on 15 February 2025 and is scheduled to continue until 19 April 2025.
Discussion
This study aims to elucidate the role of gamification in assisting individuals with MS in better managing their daily lives. If successful, our interventions, which incorporate engaging activities, are expected to enhance patients' awareness and understanding of the disease and its effective management strategies. Additionally, these interventions will likely boost their motivation to adhere to treatment plans and health regimens. As known so far, by reducing stress and anxiety, disease management strategies may foster a greater sense of control over their condition. Involving families in the care process will also equip them with the necessary skills to serve as effective supporters in the treatment and care of patients.66 67
A systematic review has highlighted the scarcity of experimental research examining the impact of gamification on the self-management of chronic diseases among young individuals.68 Consequently, the present research seeks to provide a more comprehensive understanding of this issue by employing a mixed-methods approach that combines qualitative and quantitative research methodologies.
Moreover, previous studies have indicated that patients with MS express a desire for self-management programs with web-based capabilities.69 Therefore, our gamification application for patients will be designed to be accessible on any Internet-connected device. It is also essential that an integrated eHealth application addresses the specific needs of patients with MS, incorporating family involvement to enhance patient engagement in self-management.11 This consideration will be integral to our study during the design phase.
Ethics and dissemination
This study is part of a doctoral thesis that has received approval from the Research Ethics Board of Tehran University of Medical Sciences, with the number IR.TUMS.FNM.REC.1401.185. The protocol for the quantitative component of this study was prospectively registered on the Iranian Registry of Clinical Trials (IRCT20240116060708N1 on 30 July 2024). Before commencing the research, comprehensive explanations regarding the purpose and methods of the study will be given, and informed consent from all participants either qualitative or quantitative will be obtained. All personal and collected data were treated as confidential at all stages of the study and were stored separately in locked files. The control group in this study will be the waiting group, and if the intervention’s effectiveness is confirmed on completion of the study, it will also be offered to them. Findings will be disseminated at the local, national and international levels to ensure accessibility for all. In publications, the recommendations of the International Committee of Medical Journal Editors for authorship eligibility will be followed.70
Ethics statements
Patient consent for publication
Acknowledgments
This study is part of a Nursing PhD dissertation at Tehran University of Medical Sciences. The researchers would like to express their gratitude to the Tehran University of Medical Sciences.
References
Footnotes
Contributors All the authors have made intellectual contributions to the manuscript; contributed to the conception and design; involved in revising the document critically; agreed to be personally accountable for the author’s contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved and the resolution documented in the literature; and read and approved the final manuscript. LZ was involved in drafting the manuscript, is the guarantor of this work and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.