Article Text

Abstract
Objectives Obesity and overweight significantly impact public health. The benefits of water aerobics (WAs) have been shown in obesity and overweight people, but the effects of WAs on body composition improvement are still unclear.
Design Systematic review and meta-analysis.
Data sources A systematic literature search was conducted on 16 November 2024, across the PubMed MEDLINE, Ovid MEDLINE, Embase, Scopus, Web of Science and the Cochrane Library.
Eligibility criteria for selecting studies Only randomised controlled trials (RCTs) were included, which were independently screened by two researchers. All RCTs on WAs that evaluated the anthropometric and body composition parameters of overweight and obesity subjects were included. Eligible studies were reported following the Reporting Items for Systematic Reviews and Meta-Analysis statement.
Data extraction and synthesis All process were independently screened by two researchers (ZD, HZ). A fixed-effects or random-effects model was chosen based on the heterogeneity of the studies. The risk of bias in the included studies was assessed using the Risk of Bias V.2.0 tool, and sensitivity and subgroup analyses were conducted for outcome indicators. The quality of evidence for each outcome was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system.
Results A total of 10 studies involving 286 participants were included. Sensitivity analyses were performed for percent body fat (PBF) with high heterogeneity, and the results were robust. WAs were able to reduce body weight (BW) (weighted mean differences (WMD)=−2.69, 95% CI −4.10 to −1.27, p<0.05, I2=0.0%) and waist circumference (WC) (WMD=−2.75, 95% CI −4.41 to −1.09, p<0.05, I2=27.0%), but the effect on other body indicators was not significant. The GRADE assessment revealed that the certainty of evidence was low for body mass index, lean mass, fat mass, waist-hip ratio and hip circumference and very low for PBF. In contrast, the certainty of evidence for BW and WC was moderate.
Conclusion For the obesity and overweight people, WAs interventions over 10 weeks (ie, 12 weeks) reduced BW and WC, with more significant effects in women and greater improvements in body composition in middle-aged and older adults (average age ≥45 years). The moderate certainty of evidence for BW and WC, as assessed using the GRADE framework, indicates that these findings are robust.
PROSPERO registration number CRD42023466969.
- Meta-Analysis
- Obesity
- Overweight
- SPORTS MEDICINE
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study systematically reviewed and meta-analysed randomised controlled trials (RCTs), the gold standard in clinical research, ensuring a high level of methodological rigor.
Studies of registered or ongoing RCTs were not included in the search for articles, and only studies published in English were considered.
Judgements made by persons were more subjective when using Risk of Bias tools and the Grading of Recommendations Assessment, Development, and Evaluation system for literature and outcome quality assessment.
There were certain limitations to the articles included in the study: (1) some studies had short durations (eg, 6 weeks), small sample sizes and limited data; (2) a small number of participants in the study dropped out of the trial halfway through; (3) differences in the age, sex ratio and location of the trial participants in three aspects.
Introduction
The global prevalence of obesity has increased significantly over the past 40 years.1–3 In 2022, more than 43% of adults worldwide were estimated to be overweight, while 504 million women and 374 million men were estimated to be obese.4 Obesity is a chronic disease that raises the risk of various complications and contributes to an estimated 2.8 million deaths annually.5–7 Exercise is a highly effective method for weight management,8–10 but individuals with obesity and overweight are prone to severe bone and joint injuries during physical activity due to their weight.11 Traditional land-based aerobic exercise methods increase musculoskeletal damage in obese patients.12 The American College of Sports Medicine recommends water aerobics (WAs) for people with obesity to reduce the risk of injury and enhance exercise adherence.13 WAs interventions are increasingly recognised as a beneficial and effective approach to treating obesity.14 15 The buoyant effect of water helps reduce joint injuries commonly associated with exercise in overweight and obese individuals.16 17 Studies have shown that WAs have a better effect on improving body composition in obesity and overweight people. For example, young obese adults (mean age 18–25 years) lost weight and improved their body mass index (BMI) after 12 weeks of WAs.18 Middle-aged adults (mean age 47–70 years) also demonstrated significant reductions in body weight (BW) and percent body fat (PBF) after participating in 6 weeks of WAs.19 Additionally, WAs led to significant improvements in body composition (eg, PBF, BW, BMI and waist-to-hip ratio (WHR)) in overweight older men (mean age 62–70 years).20 Overweight older adults (mean age 72 years) who participated in a 28-week WAs programme showed reductions in body fat mass (FM) and both leg and waist circumference (WC).21 Therefore, WAs is a valuable exercise method and can be an important strategy for weight loss in individuals with obesity and overweight.19 21
However, fewer studies have been reported on the effects of WAs on physical indicators in obesity and overweight people. Previous literature reviews have provided broad overviews of the relevant evidence, but none have specifically focused on obesity and overweight people.14 22 23 For example, Zhu et al 24 summarise the physical effects of aquatic exercise on adults. However, this study only included randomised controlled trials (RCTs) on healthy adults and did not consider those with obesity or overweight.24
Thus, the systematic review and meta-analysis presented in this study aims to fill this research gap by specifically examining the effects of WAs on physical indicators in obesity and overweight people. The primary focus of this study is to determine whether WAs significantly improve physical indicators in obesity and overweight people.
Methods
Registration
This meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement.25 26 The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (registration number: CRD42023466969). Minor changes were made to the initial PROSPERO protocol submitted in October 2023 (online supplemental table S1).
Supplemental material
Supplemental material
Search strategy
Six databases were searched: PubMed MEDLINE, Ovid MEDLINE, Embase, Scopus, Web of Science and the Cochrane Library. The search covered the period from the inception of the database up to 16 November 2024. Retrieval strategy based on PICOS tool:27 (P) Population: adults with overweight and obesity; (I) Intervention: WAs; (C) Comparator: other exercise modalities or no exercise control; (O) Outcome: body composition; (S) Study type: RCTs. Search using core terms: water aerobics (eg, aquatic fitness, aqua aerobics), obesity or overweight (eg, fat, obese), and RCTs (eg, randomised controlled study, controlled clinical trials). The core terms for the searches were identified in the MeSH Database in the PubMed database, respectively, to ensure the scientific validity and accuracy of the search vocabulary, and the comprehensiveness of the search scope (details of the search strategy are in online supplemental table S2). In addition to the database search, the reference lists of included articles were screened for studies that met the inclusion criteria.
Eligibility criteria
Inclusion criteria: (1) RCTs; (2) participants were adults (18 years) with obesity (BMI≥30 kg/m²) or overweight (BMI≥25 kg/m2), including older adults;28 (3) the intervention group participated in WAs for at least 4 weeks, and the control group did not participate in exercise or chose other ways of exercising; (4) the study reported results on changes in body composition; (5) the full text of the study was available in English (ie, not a review, letter, case series or conference proceedings). Grey literature (ie, dissertations, conference abstracts) was excluded, as it has been shown that these represent only a small percentage of the studies included in the systematic review and rarely affect the statistical or clinical significance of the results.29
Exclusion criteria: (1) trials that did not satisfy all inclusion criteria; (2) studies that included participants diagnosed with other diseases; (3) exercise interventions combined with dietary control, medication or other lifestyle changes; (4) there was no exercise of any form, just a trial of being immersed in water or receiving a massage.
Study selection
The study used EndNote (V.21) to manage the articles. First, duplicate articles were removed. Second, the titles and abstracts of the articles were read and qualified articles were selected. Finally, full-text review was performed. The process was independently screened by two researchers (ZD, HZ). Disagreements were adjudicated by a third researcher (ZG).
Data extraction
Data from the included studies were recorded using an adapted Cochrane Collaboration standardised data extraction form.30 The following study characteristics were extracted: year of publication, authors, region, study period, study design, sample size, participants and mean age.
BW, measured in kilograms (kg), serves as a direct indicator of overall weight loss and is a key measure of intervention effectiveness in obesity management.31 BMI, a widely used but indirect measure of body fatness, is calculated as weight in kilograms divided by height in metres squared (kg/m2).32 PBF is an important metric for distinguishing between lean mass (LM) and FM.33 FM and LM were assessed using bioelectrical impedance analysis or dual-energy X-ray absorptiometry, with PBF calculated using the formula: PBF = (FM (kg)/BW (kg))×100.34 WC reflects abdominal fat distribution and is a validated marker of central obesity and metabolic risk.35 Risk thresholds for WC are ≥102 cm for men and≥88 cm for women.36 Both WC and hip circumference (HC) were measured in centimetres (cm) using an inelastic tape. WC was defined as the minimum circumference between the rib margins and iliac crests, while HC was defined as the maximum circumference between the waist and thighs. The WHR was calculated as WC/HC.34 WHR is a measure of upper and lower body fat distribution, with higher values indicating a greater risk of obesity-related health problems. Risk thresholds for WHR are men ≥1.0 and women ≥0.85.36 Therefore, the primary outcomes were BW, BMI, PBF, WHR, WC and HC, while the secondary outcomes were FM and LM.
Two researchers (ZD, HZ) independently extracted this information from each study, and any disagreements were resolved through discussion.
Risk of bias
Two researchers (ZD and HZ) independently assessed the risk of bias in the included RCTs using the Cochrane Risk of Bias (RoB) V.2 tool, following the evaluation criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (V.6.4).37 Any disagreements during the review process were discussed and resolved through consultation with a third researcher (ZG) from the review team.
Data analysis
Meta-analysis was conducted using Stata V.18.0 software. Heterogeneity among studies was assessed using Cochran’s Q and I2 tests.38 When p>0.1, I2≤50%, there was homogeneity, and a fixed-effects model was used for the meta-analysis; when p≤0.1, I2>50%, there was heterogeneity, and a random-effects model was used.39 40 Therefore, this study uses a fixed-effects model for the meta-analysis, which was changed to a random-effects model when I2>50%.
To further test the stability of the results, a sensitivity analysis was performed using the leave-one-out method.41 This method involves excluding one study at a time, combining the remaining studies in a meta-analysis and assessing whether the results of the original meta-analysis were significantly altered by the influence of certain studies by observing the changes in the combined results.42 Publication bias was assessed using funnel plots, with asymmetric distribution indicating potential bias.43 Quantitative analysis of funnel plot asymmetry was conducted using the Egger regression test.44
Differences were considered significant at p<0.05.45
The SEM of the extracted data was converted to SD,46 using the formula in the Cochrane Handbook47 (N represents the number of trial participants):

Quality of GRADE evidence
The quality of evidence for each outcome was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology.48 Two researchers (ZD and HZ) independently conducted the assessments. Any disagreements were resolved through discussion and, when necessary, consultation with a third researcher (ZG) to reach a consensus. As all included studies were RCTs, the initial evidence quality was rated as high. However, the confidence in the evidence could be downgraded based on specific limitations in the original studies, including risk of bias, inconsistency, indirectness, imprecision and publication bias.49 Following GRADE guidelines, the final quality of evidence was categorised into one of four levels: high, moderate, low and very low.50
Results
Study search results
A total of 4517 studies were searched. Of these, 1185 were removed due to duplication, leaving 3332 studies for further screening. After reviewing the titles and abstracts, 3267 studies were excluded. 65 articles were eligible for full-text screening, of which 55 were deleted. Ultimately, 10 studies were included in the meta-analysis (figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Study characteristics
The 10 RCTs included in this study involved a total of 286 participants.51–60 Publication dates range from 2009 to 2021 (note: this refers to the publication date of articles analysed that met the inclusion criteria; the search strategy was from database construction to 16 November 2024). The studies included trials conducted in Malaysia, Brazil, India, the USA and the Netherlands. The participants’ ages ranged from 20 to 70 years.
A small number of subjects from five trials51 53 55 58 59 dropped out of the experiment for various reasons, and trial data from those who dropped out were not used. One study51 included two distinct intervention groups: aqua zumba (Yusof-1) and aqua jogging (Yusof-2). Due to the differing exercise programmes, these groups were treated as separate studies (Yusof-1 and Yusof-2) in the analysis.
The types of WAs included in this review were diverse and encompassed activities such as water aerobics, aqua zumba, water yoga and aqua jogging. The intervention periods ranged from 6 to 12 weeks across all included trials. One of the trials55 had an exercise frequency of two times a week; others were three times a week. The exercise time varied according to the needs of the trials, with most being 60 min each.
The units for BW, LM and FM are kg; for BMI, kilograms per square metre (kg/m²); and for WC and HC, cm. The basic characteristics of each study are shown in table 1.
Experimental details
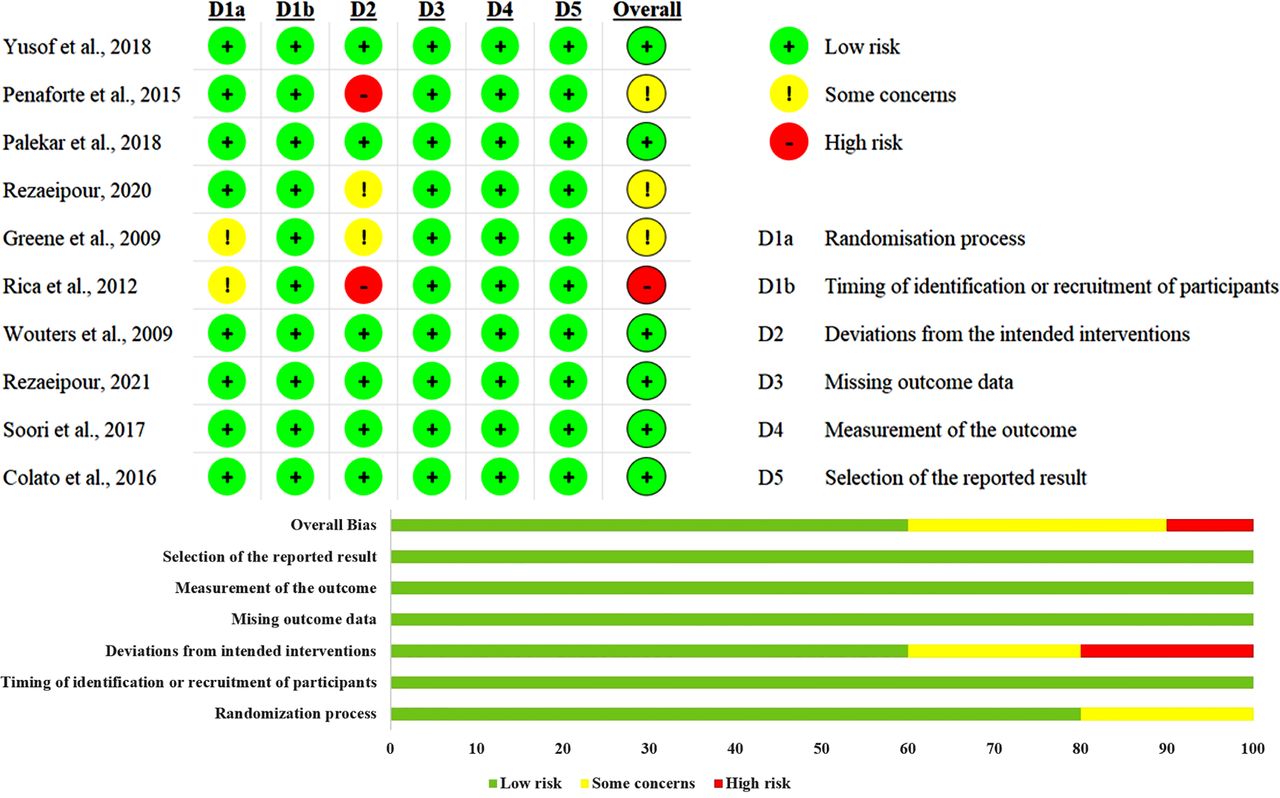
Results of RoB assessment
Following the risk of bias assessment, the 10 included studies were rated as follows: 6 studies had a low risk of bias, 3 studies had some concerns and 1 study had a high risk (figure 2).

Risk of bias.
Physical outcome
WAs proved to be an effective intervention for reducing BW (WMD=−2.69, 95% CI −4.10 to −1.27, p<0.05, I2=0.0%) and WC (WMD=−2.75, 95% CI −4.41 to −1.09, p<0.05, I2=27.0%) in obesity and overweight people (online supplemental figures S1 and S2). However, other physical indicators, such as BMI (WMD=−0.55, 95% CI −1.29 to 0.19, p>0.05, I2=0.0%) (online supplemental figure S3), PBF (WMD=−4.83, 95% CI −10.32 to 0.66, p>0.05, I2=93.6%) (online supplemental figure S4), LM (WMD=−0.19, 95% CI −2.75 to 2.37, p>0.05, I2=0.0%) (online supplemental figure S5), FM (WMD=−0.92, 95% CI −3.20 to 1.36, p>0.05, I2=0.0%) (online supplemental figure S6), WHR (WMD=−0.02, 95% CI −0.05 to 0.01, p>0.05, I2=0.0%) (online supplemental figure S7) and HC (WMD=−1.05, 95% CI −3.64 to 1.55, p>0.05, I2=0.0%) (online supplemental figure S8), did not show significant improvements (table 2).
Subgroup analysis of water aerobics on anthropometric measures
Subgroup analysis of outcomes
Subgroup analyses of WAs were performed on the included studies to identify appropriate WAs regularity and to explore sources of heterogeneity. Due to the number of subgroups, the results of the subgroup analyses of WAs are summarised in table 2 (table 2).
As shown by the subgroup analyses of BW, WAs with a trial duration greater than 10 weeks (ie, 12 weeks) significantly reduced BW (WMD=−3.31, 95% CI −5.23 to −1.40, p<0.05, I2=0.0%). Additionally, WAs significantly reduced BW in the female population (WMD=−2.90, 95% CI −4.37 to −1.43, p<0.05, I2=0.0%) and in the population with a mean age of ≥45 years (WMD=−2.85, 95% CI −4.31 to −1.40, p<0.05, I2=0.0%).
From the subgroup analysis of WC, it is shown that WAs with a trial duration >10 weeks significantly reduced WC (WMD=−2.88, 95% CI −4.63 to −1.12, p<0.05, I2=56.3%). Among them, WAs were mainly able to significantly reduce WC in the female population (WMD=−2.89, 95% CI −4.65 to −1.13, p<0.05, I2=56.1%) and in the population (WMD=−3.03, 95% CI −4.85 to −1.22, p<0.05, I2=65.5%) with a mean age ≥45 years.
Other subgroup analyses found that BMI (p=0.146, I2=0.0%), LM (p=0.883, I2=0.0%), FM (p=0.429, I2=0.0%), WHR (p=0.256, I2=0.0%) and HC (p=0.429, I2=0.0%) were neither heterogeneous nor significant. In contrast, PBF (I2=93.6%) and WC (I2=27.0%) were heterogeneous. However, separate subgroup analyses revealed multiple sources of heterogeneity, which could not be adequately explained by only one pair of subgroup analyses.
Sensitivity analysis of PBF
PBF exhibited high heterogeneity. Therefore, the robustness of the results was assessed through sensitivity analyses to identify potential sources of heterogeneity. A leave-one-out sensitivity analysis was performed, revealing that the direction of the combined estimates did not change significantly with the removal of any individual study. This finding suggests that the meta-analysis was robust and not unduly influenced by any single study.61 The results show that the 95% CI excludes 0 (figure 3). This means that the results are robust, the sensitivity is small and the original meta-analysis results are statistically significant.

Sensitivity analysis of percentage body fat.
Publication bias
Publication bias was evaluated for the inclusion of more than 10 studies.62 The risk of bias for the BW outcome measures was assessed using funnel plots and Egger’s regression test.30 Based on Egger’s regression test (p=0.841 > 0.05), no significant publication bias was detected. The visual inspection of the funnel plot (figure 4) further supports this conclusion.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot for body weight.
GRADE assessment
The quality of evidence for each outcome was evaluated using the GRADE system. The results indicated that the quality of evidence was moderate for BW and WC; low for BMI, LM, FM, WHR and HC; and very low for PBF (table 3). Primary reasons for downgrading included small sample sizes in the included studies, 95% CI crossing equivalence thresholds and high heterogeneity.
GRADE quality of evidence
Discussion
This study systematically reviewed the effects of WAs on body composition in obesity and overweight people. The results showed that WAs had a positive impact on body composition,63 with significant effects on reducing BW and WC.18 64 Specifically, the findings were as follows: (1) WAs significantly reduced BW and WC in women; (2) WAs with a trial duration of 10 weeks or more (ie, 12 weeks) showed significant reduction in BW and WC; (3) continuous WAs in middle-aged and older individuals (average age ≥45 years) led to better reductions in BW and WC.65 66
The results of the subgroup analyses provide more detailed insights into the factors influencing the effects of WAs on obesity and overweight people. According to the subgroup analysis of BW, WAs with a trial duration greater than 10 weeks (ie, 12 weeks) resulted in a more significant reduction in BW, while those with a duration of 10 weeks or less showed no significant effect. This suggests that short-term WAs (eg, 6 weeks) had a limited impact on BW and body composition,52 67 whereas longer interventions (12 weeks or more) were more effective.22 68 It has been suggested that WAs are effective for reducing BW in overweight older men.20 However, the present study found that WAs reduced BW significantly in women and not in men, probably due to the small number of males included in the study, resulting in non-significant differences. WAs were more effective in reducing BW in middle-aged and older adults (average age ≥45 years). Aerobic exercise in water is beneficial for middle-aged and elderly people, improving body composition while easing the joint loads associated with land-based exercise.69
In addition, subgroup analyses based on WC revealed that the WAs intervention significantly reduced WC in obesity and overweight people. WC is a key indicator of abdominal obesity,70 71 and 12 weeks of WAs was particularly effective in reducing WC in obese and overweight women.64 Further subgroup analysis showed that WAs with a trial duration greater than 10 weeks (ie, 12 weeks) had a more significant impact on WC, while trials lasting 10 weeks or less had no significant effect on WC. Due to the small number of male participants in the included studies, the effect of WAs on male WC requires further confirmation. WAs also had a greater effect on reducing WC in middle-aged and older individuals (average age ≥45 years), while no significant effect was observed in other (average age <45 years) people.
Obesity and overweight people can receive many health benefits through exercise. However, the subgroup analyses showed that the effect of WAs on BMI and PBF was not significant in obesity and overweight people. Previous studies have suggested that 8 weeks of continuous training may be insufficient to observe significant benefits and that beneficial effects on anthropometric parameters typically become evident after training periods of 12 to 32 weeks.72 If subgroups were divided according to trial period, sex and age for several other body components (LM, FM, WHR, HC), the number of studies in each subgroup would be small, producing results with less confidence. Therefore, several other body components were not analysed in this study.
The GRADE assessment revealed that the certainty of evidence was low for BMI, LM, FM, WHR and HC and very low for PBF. The downgrading of evidence was primarily due to small sample sizes, which reduced statistical power and the precision of effect estimates. In addition, high heterogeneity among studies, particularly in PBF outcomes, indicated variability in study populations, methodologies and intervention effects. Imprecision, as evidenced by wide CIs crossing equivalence thresholds, further contributed to the reduced quality of evidence.
These findings have significant implications for clinical practice. However, there are several limitations to this study. Studies of registered or ongoing RCTs were not included in the search for articles, and only studies published in English were considered. Judgements made using the RoB tools for literature quality assessment are inherently subjective. Some of the studies had short (6 weeks) duration of trials, small sample sizes and less research data. A small number of participants in the study dropped out of the trial halfway through. There were differences in the age, sex ratio and geographic location of participants across the studies. The low certainty of evidence for BMI, WHR, HC and other secondary outcomes and very low certainty for PBF suggest that current evidence was insufficient to reliably inform clinical guidelines for using WAs to improve these parameters. Health professionals should approach these results with caution and prioritise interventions with stronger evidence when aiming to target these specific outcomes. However, the moderate certainty of evidence for BW and WC supports the use of WAs as an effective interventions for reducing overall body weight and central obesity, which were critical factors in managing obesity-related health risks.73 74
Conclusions
The results of this systematic review and meta-analysis suggest that WAs is an effective intervention for reducing BW and WC in overweight and obesity adults. Specifically, WAs interventions lasting over 10 weeks significantly reduced BW and WC, with a more pronounced effect observed in females. Middle-aged and elderly individuals also showed better improvements in body composition following WAs interventions. The certainty of evidence, as assessed using the GRADE framework, was moderate for both BW and WC, indicating that these findings are robust but would benefit from further research to enhance confidence. In contrast, the certainty of evidence for other outcomes was rated as low or very low, primarily due to small sample sizes, high heterogeneity and imprecision in the included studies. Future research should aim to address these limitations by conducting larger, well-designed RCTs with standardised methodologies and diverse populations. Additionally, investigating the long-term effects of WAs and comparing its efficacy with other exercise modalities will provide valuable insights. In conclusion, WAs is an important form of exercise for overweight and obesity people, offering significant benefits in improving body composition and overall health.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Thanks to all those who helped with this paper.
References
Footnotes
Contributors Study conception and design: ZD, JP. Acquisition, analysis or interpretation of data: ZD, ZG, HZ. Drafting the manuscript: ZD, HZ, ZG. Critical revision of the manuscript for important intellectual content: JP. Statistical analysis: ZD, ZG, HZ. Supervision: JP. ZD is responsible for the overall content as a guarantor. All authors have read and agreed to the published version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.