Article Text

Abstract
Objective A systematic analysis was conducted to investigate the association between tinnitus incidence and daily dietary patterns.
Design We conducted a systematic review and meta-analysis of observational studies.
Data sources The PubMed, Embase, Web of Science and Cochrane Library databases were searched from their inception to 25 May 2024.
Eligibility criteria for selecting studies We included observational studies from peer-reviewed English-language journals that examined tinnitus presence or severity in adults aged 18 years or older, including associated prevalence estimates.
Data extraction and synthesis Data extraction was independently conducted by two evaluators, who assessed research bias using the Agency for Newcastle-Ottawa Scale and applied evidence classification criteria for aggregate grade strength assessment. This study adhered to the guidelines of the Preferred Reporting Project (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and Meta-Analysis of Epidemiological Observational Studies, as well as the PROSPERO Registry protocols. A mixed-effect model combined maximum adjusted estimates, with heterogeneity measured using the I2 statistic. Sensitivity analysis validated the robustness of the analysis, and publication bias was assessed qualitatively and quantitatively.
Results A total of 10 retrospective studies were identified and included in this analysis, with the last eight studies incorporated into the meta-analysis. Fifteen dietary factors were examined. Fruit intake, dietary fibre, caffeine and dairy product consumption were negatively correlated with tinnitus incidence (OR=0.649 (95% CI 0.532, 0.793), p<0.0001), (OR=0.918 (95% CI 0.851, 0.990), p=0.03), (OR=0.898 (95% CI 0.862, 0.935), p<0.00001), (OR=0.827 (95% CI 0.766, 0.892), p<0.00001), respectively. A sensitivity analysis confirmed the robustness of the findings.
Conclusions This systematic review and meta-analysis suggest a link between particular dietary elements and a lower incidence of tinnitus.
PROSPERO registration number CRD42023493856.
- OTOLARYNGOLOGY
- NUTRITION & DIETETICS
- Meta-Analysis
- Neurotology
Data availability statement
Data are available upon reasonable request. The data used to support the findings of this study are available from the corresponding author upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study conducted a thorough literature screening, assessed the quality of the literature based on international standards, and excluded articles with a high risk of bias.
This review involved a large population base, improving its representation of fundamental population characteristics, and the heterogeneity among the studies regarding the main observations was minimal, ensuring the solidity of the findings.
The relatively small number of included articles may have led to certain conventionally accepted beneficial dietary factors (such as vegetables and eggs) not demonstrating significant differences. In addition, owing to the limited data in the original literature, a dose–effect meta-analysis cannot be supported.
The majority of the included articles were cross-sectional studies, underscoring the necessity for further cohort studies or Mendelian randomisation studies to investigate causal relationships and provide additional clinical evidence for the dietary prevention of tinnitus.
Introduction
Tinnitus, characterised by perceived sounds such as buzzing, cicadas, or electric currents, occurs without external auditory stimuli.1 It is associated with distress, depression, anxiety, stress and, in severe cases, suicide, significantly affecting overall quality of life.2 3 Recent epidemiological data suggest a global pooled prevalence of about 14.4% in adults and 13.6% in children and adolescents.4 The notable prevalence of tinnitus and its substantial impact on life and mental well-being have increasingly become significant medical and societal concerns.5
The origins of tinnitus remain elusive and involve a range of factors. Some researchers have suggested neural dysfunction or circulatory issues in the inner ear, abnormal neuronal activity in central auditory pathways and irregular activity in non-auditory brain regions such as the anterior insula, anterior cingulate cortex and thalamus.6 In clinical practice, treatments for tinnitus management include psychological counselling, cognitive–behavioural therapy, tinnitus retraining therapy, sound therapy, surgery, pharmacological interventions and non-pharmacological interventions (including electrical stimulation, repetitive transcranial magnetic stimulation, nerve block, bimodal neuromodulation, tinnitus retraining therapy, etc), as well as hearing aids and cochlear implants for patients with relevant hearing loss.7 8 Owing to an incomplete understanding of central neuropathological mechanisms, no single treatment universally meets the needs of all patients.9 10
Diet can have a significant impact on tinnitus, but it remains uncertain which specific foods worsen or relieve tinnitus symptoms. Diet is an uncertain factor for tinnitus, as mentioned in the James Lind Alliance prioritisation statement. Optimising nutritional intake is an essential part of multidimensional efforts to prevent and treat chronic diseases. In recent years, there has been an increase in interest and need for nutritional treatment programmes for tinnitus,11 as evidenced by various population-based studies found in recent publications.12–15 A population study investigating the correlation between diet and tinnitus among UK adults revealed a decrease in tinnitus incidence with increased fruit and vegetable consumption. Conversely, avoiding dairy was linked to a greater risk of tinnitus. On the other hand, abstaining from eggs, adding fish to the diet and consuming caffeinated beverages are suggested to potentially lower the risk of tinnitus.2 Another study in British adults revealed that greater fat intake was associated with a greater likelihood of experiencing tinnitus.16 Similarly, Lee and Kim identified risk factors for tinnitus, including low water, protein, riboflavin and niacin intake, although this was unrelated to fruit and vegetable consumption.17 It is thought that the intake of high-quality nutrients through food can have a positive effect on the hearing system by improving blood flow to the cochlea, reducing oxidative damage and reducing inflammation. In contrast, high saturated fat intake may increase the risk of tinnitus through cardiovascular pathways.11 16 Tang et al 18 reported that inadequate fruit fibre (<3.6 g/day) and grain fibre (<4.2 g/day) intake were linked to a 65% and 54% increased risk of developing tinnitus over the next decade, respectively. Conflicting results have hindered researchers’ ability to understand the potential benefits of diet; hence, a systematic review on the relationship between diet and tinnitus is needed.
To date, there has not been a comprehensive examination through systematic reviews or meta-analyses regarding the link between typical dietary patterns and tinnitus. Our objective was to systematically explore this association while accounting for potential confounding variables. This study aimed to provide clinical evidence to inform the development of dietary prevention approaches for tinnitus.
Method
According to the guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA), a set of evidence-based standards for the research quality of systematic reviews, which apply to published reviews of literature that contain primary data sources and aim to improve the scientific rigour of systematic reviews,19 the protocol for this study was appropriately registered on PROSPERO under the registration number CRD42023493856. Additionally, our reporting is guided by the Meta-analysis of Observational Studies in Epidemiology (MOOSE) standards for epidemiological observational studies, which were developed by a group of experts to improve the quality and transparency of meta-analysis and systematic evaluation of observational studies, contributing to the scientific validity and credibility of such studies, as referenced.20 The MOOSE listings is presented in online supplemental file 1 etable 1.
Supplemental material
Search strategy
We developed an inclusive search strategy covering diet-related and tinnitus-related subjects to capture pertinent literature from the PubMed, Embase, Web of Science and Cochrane Library databases. The research design was limited to systematic evaluation. There were no language restrictions imposed on the search, and we considered articles published before May 25, 2024. We used special translation software for publications in unknown languages.
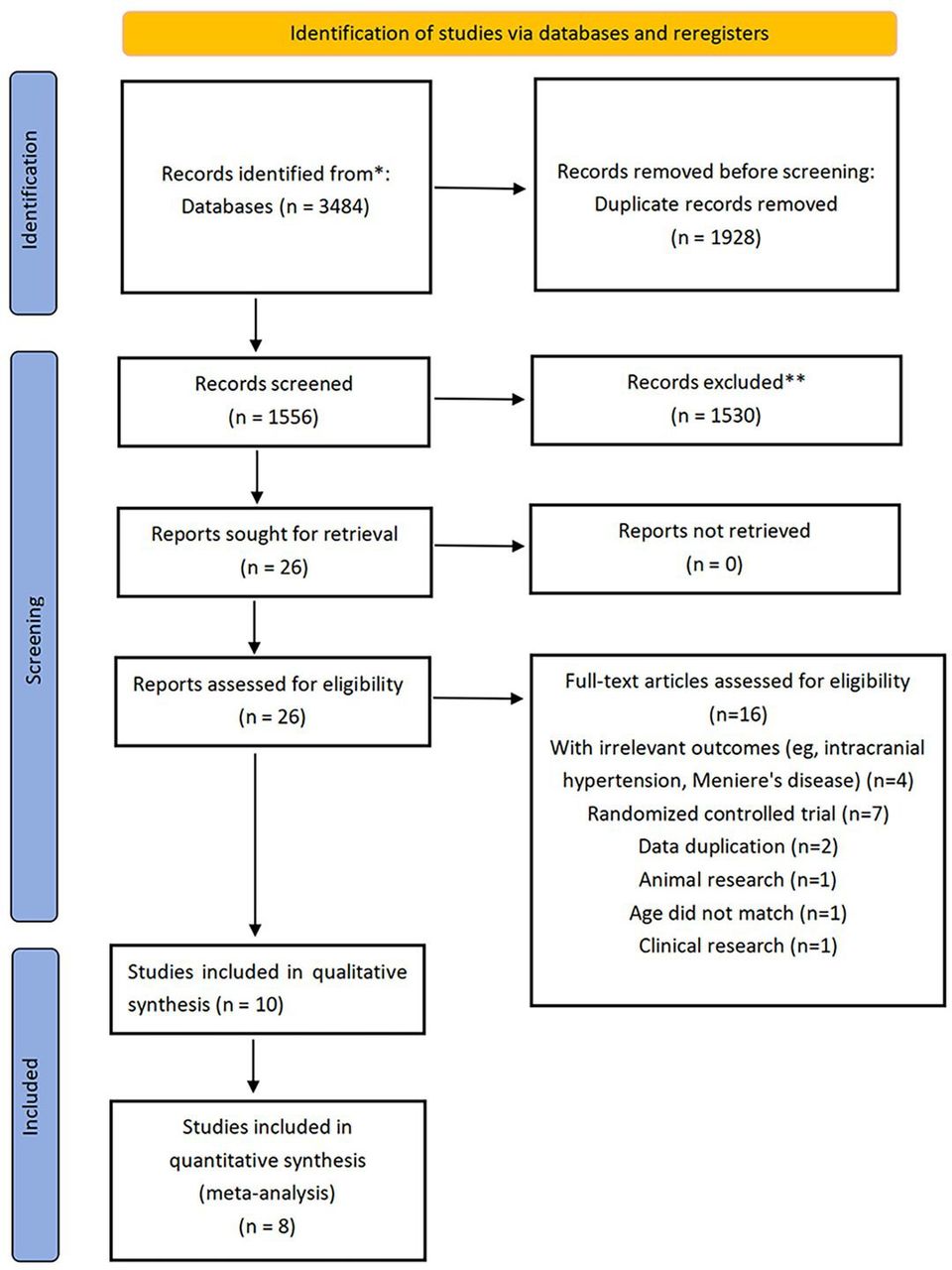
The search strategy was designed to identify studies linking tinnitus and diet, and two specific terms, ‘Tinnitus’ and ‘Diet’, from the Medical Subject Headings (MeSH) Major Topic were identified. The databases were systematically explored via a blend of MeSH terms, keywords and various text word variations related to diet, following the guidance outlined by the Scottish Intercollegiate Guidelines Network: ((tinnitus OR Ringing-Buzzing) AND (diet OR food OR water OR milk OR fish OR fruit OR vegetable OR fiber OR sugar OR meat OR margarine OR fat OR egg OR variety OR caffeine OR carbohydrate OR protein). The search strategy for each database is described in online supplemental file 1 Search Strategy. The screening process is depicted in figure 1.

Flow chart. *Means: the search results of the four databases according to the prespecified database search strategy. **Means: the process of selecting articles for title and abstract based on inclusion exclusion criteria.
The following inclusion criteria were applied: (1) inclusion of cohort, case-control, or cross-sectional studies; (2) inclusion of all individuals in the study population; (3) consideration of various dietary intakes; and (4) investigation of tinnitus as a study outcome provided effect sizes or other data on the association between dietary intake and tinnitus as an outcome. The exclusion criteria were as follows: (1) studies involving therapeutic interventions; (2) randomised controlled trials, animal experiments, cell studies, case reports, literature and incomplete or invalid sources, and the original literature lacked sufficient data to calculate the risk ratio for tinnitus (some publications do not report effect sizes but instead allow the raw data to be used to calculate them. In these cases, RevMan (V.5.3) was used to calculate the OR).
Data collection
In table 1, data compilation was conducted by two reviewers (SZ and MZ), including authors’ names, participant counts, age spans, survey/diagnosis specifics and information on food and tinnitus. Given that dietary intake is a continuous variable, some researchers have typically performed stratified comparisons on the basis of regional intake standards and researchers’ characteristics. This strategy aimed to explore the impact of varying levels of increased intake on tinnitus incidence. For most continuous variables associated with food intake, adjusted OR values were assimilated in the meta-analysis when stratified according to dose intake, with the exclusion of the reference group. In cases of direct comparison, the singular adjusted OR value was integrated. Further insights into the ORs are provided in online supplemental etable 2.
Basic information to be incorporated into the article
Literature quality evaluation
The assessment of individual study quality was conducted by two reviewers (SZ and MZ) via a modified version of the Newcastle-Ottawa Scale. Previous studies were categorised as having a high (<5 stars), moderate (5–7 stars) or low (≥8 stars) risk of bias (see online supplemental etable 3).
Statistical analysis
Data analysis was performed via RevMan (V.5.3) and Stata (V.15.0). Mixed-effect models were used to aggregate maximally covariate-adjusted ORs across all studies. In current practice, ORs, relative risks (RRs) and HRs are about equal when events occur infrequently. For this situation, it is acceptable to include OR, RR and HR in the same meta-analysis. In cases where the p value of the Q test was <0.10 or the I2 statistic exceeded 50%, we conducted an assessment to determine significant interstudy heterogeneity. For observational studies, maximally covariate-adjusted estimates were strongly prioritised. If a study employed an analytical method incongruent with synthesis for the majority of other studies, we either converted the effect estimate to the appropriate combined ratio or excluded the study from the meta-analysis.
In cases of considerable heterogeneity in the analysis with significant differences, metaregression was used to explore the source of heterogeneity (note that metaregression was considered when the data included in the analysis were greater than 10). We visually assessed the asymmetry of the funnel plot and used Egger’s bias to detect possible publication bias, with estimation of missing studies conducted via eMethods if publication bias was suspected (note that publication bias analysis was considered when the data included in the analysis were greater than 6). Moreover, we conducted a sensitivity analysis of the pooled results employing a one-by-one exclusion method.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Results
The literature screening process is shown in online supplemental etable 4. Ten articles were found in the search.2 16–18 21–26 Among these, two articles delved into individual dietary factors, namely, chocolate23 and flavonoids,22 which were not investigated in other studies. While these two articles were included in the narrative review, they were excluded from the meta-analysis. The remaining eight articles composed the dataset for the meta-analysis.
Fifteen common dietary factors were analysed, and dietary sources were assessed via validated nutrition/diet questionnaires. The combined findings revealed that four diets (caffeine, fruit, dietary fibre and dairy products) were negatively associated with the incidence of tinnitus; that is, the higher the intake of caffeine, fruit, dietary fibre, and dairy products, the lower the prevalence of tinnitus.
A meta-analysis of dietary factors
The meta-analysis included eight studies with a total of 301 533 people and analysed 15 dietary factors, as shown in figure 2: carbohydrates (2/8, online supplemental efigure 1), caffeine (4/8, online supplemental efigure 2), varied diets (2/8, online supplemental efigure 3), eggs (2/8, online supplemental efigure 4), fruits (3/9, online supplemental efigure 5), fibres (3/8, online supplemental efigure 6), fat (3/8, online supplemental efigure 7), margarine (2/8, online supplemental efigure 8), meat (2/8, online supplemental efigure 9), sugar (3/8, online supplemental efigure 10), protein (2/8, online supplemental efigure 11), fish (3/8, online supplemental efigure 12), vegetables (4/8, online supplemental efigure 13), water (3/8, online supplemental efigure 14) and dairy (2/8, online supplemental efigure 15). The summary results are depicted in figure 2. The intake of dairy products, fruits, dietary fibre and caffeine was negatively correlated with the prevalence of tinnitus: 0.827 for dairy (95% CI 0.766 to 0.892), I2=0%, p<0.00001; 0.649 for fruit (95% CI 0.532 to 0.793), I2=0%, p<0.0001; 0.918 for fibre (95% CI 0.851 to 0.990), I2=63%, p=0.03; and 0.898 for caffeine (95% CI 0.862 to 0.935), I2=23%, p<0.003. No associations were found between other dietary factors and tinnitus.

{kind=link}
{kind=link}
Risk ratio summary of diet and tinnitus incidence. The blue or red dots represent OR values, and the black lines represent CIs. P<0.05 indicates statistical difference. The evidence classification criteria: class I (convincing evidence), class II (highly suggestive evidence), class III (suggestive evidence), class IV (weak evidence) and NS (non-significant). GRADE, Grade of Recommendations Assessment, Development, and Evaluation. Moderate: the results of current efficacy evaluation are likely to be close to the true value; low: the reliability of the current efficacy evaluation results is uncertain; very low: the reliability of the current efficacy evaluation results is very uncertain.
Sensitivity analysis
We conducted sensitivity analyses for various dietary intakes on the basis of predefined analysis criteria (requiring data from the included articles to exceed 6). Contradictory outcomes were noted in the aggregated results for caffeine (refer to online supplemental efigure 16), with the analysis attributing these contradictions to data within the same article (Abby McCormack, 2014). Sequential exclusion of fruit (refer to online supplemental efigure 17) and dietary fibre (refer to online supplemental efigure 18) maintained the statistical significance of the combined OR. Successive exclusion of summary results for vegetables (refer to online supplemental efigure 19) and sugar (refer to online supplemental efigure 20) revealed no contradictory outcomes in the combined OR, thus ensuring the robustness of the meta-analysis results. The comprehensive sensitivity analysis revealed the relative robustness of the meta-analysis results, confirming the associations of fruit and dietary fibre intake with the prevalence of tinnitus. No significant associations between other dietary intakes and tinnitus were found.
Publication bias
The funnel plot and Egger test findings for caffeine, fruit, vegetables, diet, sugar and fat indicated the presence of publication bias (online supplemental efigure 21–26). We performed a supplementary analysis using the shear compensation method, which yielded consistent results that suggest that publication bias did not impact the main outcome.
Discussion
In this systematic review and meta-analysis involving eight observational studies (comprising a total of 301 533 participants), we discovered that increased dietary consumption of fruit, dietary fibre, dairy products and caffeine was associated with a reduced occurrence of tinnitus. These reductions were 35.1% (20.7%–46.8%) for fruit intake, 9.2% (1%–14.9%) for dietary fibre, 17.3% (10.8%–23.4%) for dairy products, and 10.2% (6.5%–13.8%) for caffeine intake. These results were consistently supported by the sensitivity analysis.
The association between caffeine intake and tinnitus remains contentious. Our findings indicate that caffeine has a positive effect on tinnitus incidence. Some suggest that caffeine might effectively decrease tinnitus incidence, possibly because of its anxiety-reducing effects. Conversely, some scholars argue that individuals with tinnitus often experience insomnia, in which caffeine consumption could worsen, thus exacerbating tinnitus symptoms. Recent observational studies27 28 have revealed no link between caffeine consumption and depression or anxiety levels. Furthermore, additional dose analysis revealed a J-pattern association between caffeine intake and psychiatric disorders, with about 2–3 cups per day associated with decreased risk.29 Caffeine, which acts as a non-selective adenosine receptor antagonist, can mitigate anxiety when it is ingested at a daily dose of 10 mg/kg.30 Genetic analysis also suggested a correlation between caffeine consumption and reduced tinnitus incidence.31 This effect is achieved through adenosine receptor blockade, dopamine release promotion, acetylcholinesterase activity inhibition and sympathetic nerve stimulation.
The results of most studies16 18 25 32 showed that dietary fibre and fruit intake have a positive impact on reducing the occurrence of tinnitus, and the findings of our meta-analysis clarify this reliably and comprehensively by integrating and analysing the results of all relevant studies. Some scholars have proposed that dietary fibre is associated with increased insulin sensitivity.33 Studies indicate that hyperinsulinaemia resulting from low insulin sensitivity could disturb the inner ear environment, potentially increasing tinnitus risk.34 35 Conversely, research suggests that fibre and dairy products might enhance blood vessel function,36 a factor correlated with tinnitus. Abnormal microcirculation, for example, contributes to a sustained reduction in ear blood flow, potentially leading to cochlear damage and increasing tinnitus risk.18
Our combined analysis revealed no correlation between vegetable consumption and tinnitus. Identifying the source of heterogeneity was difficult because of the limited number of articles. Nevertheless, sensitivity analyses reaffirmed the strength of our conclusions. Vegetables and fruits, which are rich in diverse vitamins and minerals crucial for maintaining health, have been shown to improve ear microcirculation, alleviate tinnitus and offer additional benefits.17 32 Future studies are expected to provide clearer results.
The body has three main sources of energy: carbohydrates (sugars), fats and proteins. Our findings indicate that protein does not increase the occurrence of tinnitus (OR=1.002 (95% CI 1.001 to 1.004), p=0.009). Protein is a crucial nutrient that requires daily consumption and plays a vital role in supporting neuronal activity and neural development.37 38 Inadequate protein intake can lead to ototoxic side effects and impair the neural function of the auditory system.39 Dawes et al demonstrated that a higher intake of dietary pattern factor 3 (high protein) was linked to a reduced likelihood of tinnitus.16 Although low-protein diets may affect auditory vestibular function, no studies have specified the necessary amount of protein in the diet. Our analysis revealed links between protein intake and tinnitus risk. Moreover, high-protein diets have been shown to induce oxidative stress in the cerebral cortex and hypothalamus of rats.40 Hence, further research on the relationship between protein dosage and tinnitus is warranted in the future.
Sugar is an essential daily component; in line with our analysis, no significant effect of sugar intake on tinnitus incidence was observed (OR 0.997 (95% CI 0.967, 1.027)). High sugar consumption is typically associated with an unhealthy lifestyle. Proinflammatory foods, including sugary items, are often associated with increased systemic inflammation and microvascular damage, particularly microischaemic events.41 Elevated blood glucose levels can harm small blood vessels and nerves in the inner ear, leading to pathological alterations in outer hair cells and spiral ganglion cells. This can result in nerve tissue ischaemia and hypoxia, leading to nerve damage.39 Conversely, Spankovich et al demonstrated that high carbohydrate intake can prevent hearing loss in older adults.42 Tang et al reported a 45% decrease in tinnitus risk for participants in the fourth quartile compared with the first quartile of carbohydrate intake.18
Both excessive and insufficient dietary intake may have adverse effects on tinnitus, underscoring the need for a dose–response analysis of diet, which would provide valuable insights for preventing dietary tinnitus. Several studies have suggested that increasing the score of healthy foods, such as fruits, vegetables, legumes, nuts, fish and dairy products, may lower the risk of cardiovascular disease and mortality.43–45 Each one-fifth increase in the healthy diet score was associated with a corresponding decrease in overall mortality rate (HR=0.92; 0.90 to 0.93), severe cardiovascular disease (HR=0.94; 95% CI 0.93 to 0.95), myocardial infarction (HR=0.94; 0.92 to 0.96), stroke (HR=0.94; 0.89 to 0.99), and death or cardiovascular disease (HR=0.93; 0.92 to 0.94).46
The outcomes of our analysis did not support a notable connection between fat intake and tinnitus risk, although there was a discernible upward trend. Moreover, high-fat diets contribute to obesity and can lead to insulin resistance.47 Conversely, adopting a low-fat/low-cholesterol diet might aid in reducing blood cholesterol and triglyceride levels, potentially alleviating tinnitus symptoms.48 Future studies are needed to verify the relationship between fat and tinnitus.
A recent study revealed that increased levels of dietary variety, including quantity, evenness and quality, were inversely linked to the risk of depressive symptoms, especially among women and older adults.49 This could offer relief for patients with tinnitus. Moreover, dietary variety is believed to be correlated with insulin resistance.50 Given the protective effects of various diets on human health, further exploration of dietary variety is necessary to validate significant associations. Our pooled analysis indicated that a variation in diet was not significantly linked to a reduced tinnitus incidence (OR=0.653 (95% CI 0.410, 1.038)) based on the currently available evidence.
We found only one study that investigated the impact of chocolate and flavonoids on the onset of tinnitus,23 but it did not provide sufficient data for a meta-analysis. Flavonoids, which are abundant in fruits and vegetables, offer antioxidant, anti-inflammatory, and vascular health benefits, which align with the pathophysiology of age-related hearing loss and tinnitus.51 Additionally, flavonoids interact with signalling cascades involving protein and lipid kinases, inhibiting neuronal death induced by neurotoxicants such as oxygen radicals and promoting neuronal survival and synaptic plasticity.52 Despite the hypothesis that dietary flavonoids might protect against tinnitus development over a 10-year period, Tang et al.51 did not support this idea. However, it is important to note that this study has limitations, such as insufficient data collection.
Chocolate is a globally consumed product renowned for its high phenolic compound content (flavonoids are a subclass of polyphenols).53 A study by Lee et al indicated that chocolate consumption is not linked to tinnitus or tinnitus-related issues.23 An animal study demonstrated that polyphenols alleviate oxidative stress in the cochlea by suppressing apoptotic signalling pathways.54 Nonetheless, excessive chocolate consumption can have adverse effects on brain hyperexcitability.55 Future investigations into the association between chocolate consumption and tinnitus should consider the intake dosage.
This systematic review and meta-analysis represents the first attempt to explore the epidemiological link between diet and tinnitus. While we examined the relationships between fruit, dietary fibre, dairy product and caffeine intake and a reduced incidence of tinnitus, it remains inconclusive whether a causal relationship exists.
Conclusion
Diet-based strategies for tinnitus prevention are anticipated to play a significant role in chronic tinnitus management. Existing evidence suggests that consuming fruit, dietary fibre, caffeine and dairy may be associated with a reduced incidence of tinnitus. The primary underlying mechanisms may involve the protective effects of these diets on blood vessels and nerves, as well as their anti-inflammatory and antioxidant properties. However, it is crucial to interpret our findings cautiously because of the overall low quality of the evidence available. In the future, further well-designed, large-scale, cross-population cohort studies are warranted to complement and verify the relationship between dietary intake and tinnitus. Additionally, focusing on the dosage and categorisation of each dietary intake would provide valuable insights.
Data availability statement
Data are available upon reasonable request. The data used to support the findings of this study are available from the corresponding author upon request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
MZ, XW and SZ contributed equally.
Contributors All authors contributed to the study’s conception and design. SZ, MZ, XW and YJ conducted data collection and analysis. SZ and QZ designed the test plan. QF as the paper guide controls the quality of the paper. XH, XL, XW and HW drew the chart. XC, LW and LF completed the writing of the test plan. XL and QZ revised the manuscript. QZ is responsible for the overall content as the guarantor.
Funding This work was supported by the National Natural Science Foundation of China (No. 81774131, 82174198), ‘Xinglin Scholars Scientific Research Promotion Plan of Chengdu University of Traditional Chinese Medicine Innovation team of traditional Chinese medicine otorhinolaryngology discipline, natural science (No. XKTD2021003), the Sichuan Natural Science Foundation (No. 2023NSFSC0668).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.