Article Text

Abstract
Objectives To explore the chained mediating role of self-efficacy and e-health literacy in the association between social support and technophobia in older adults in urban communities.
Design A cross-sectional study conducted from June 2023 to April 2024.
Setting This study was conducted in three districts of Taiyuan City, Shanxi Province, China.
Participants The study enrolled 1658 older adults (> 60 years old) in urban communities in Taiyuan.
Methods The analyses included assessments using the technophobia, e-health, self-efficacy and social support scales, and the mediating effects of these indices were investigated using Model 6 in SPSS V.26.
Results The level of technophobia in older adults was found to be moderately high. Technophobia was negatively correlated with social support, self-efficacy and e-health literacy. Stepwise regression analysis showed that age, residential situation, health and the frequency of electronic device use were risk factors for technophobia (p<0.05). Social support could influence technophobia directly (β=−0.266). In addition, self-efficacy (β=−0.080) and e-health literacy (β=−0.098) significantly mediated the relationship between social support and technophobia.
Conclusion Social support was found to affect technophobia in older adults via the independent or chained mediating effects of self-efficacy and e-health literacy.
- Community-Based Participatory Research
- Cross-Sectional Studies
- Health Services for the Aged
- MENTAL HEALTH
- PUBLIC HEALTH
- Social Support
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Community-Based Participatory Research
- Cross-Sectional Studies
- Health Services for the Aged
- MENTAL HEALTH
- PUBLIC HEALTH
- Social Support
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study explores the relationship between social support and technophobia among older adults in the community and its associated mechanisms, as well as the mediating roles of self-efficacy and e-health literacy, by constructing a chain mediation model.
The use of survey data from only one region may limit the generalisability of the research results.
As the study is cross-sectional in design, it is weak in causal inference and carries the risk of reverse causality.
Introduction
With global demographic changes and advances in digital technologies, technology-empowered smart care for older adults is an inevitable trend. Smart care services can help to not only enrich the lives of older adults and provide convenience but also mitigate health-resource shortages, reduce social service costs and improve service efficiency. However, despite the advantages resulting from the development of digital technology, many older people still maintain traditional cultural concepts, are sceptical of new technologies in the outside world and are even more worried about privacy leaks. In addition, existing intelligent health technologies have limited inclusiveness.1 Due to declines in physical function, the elderly are easily overwhelmed and experience anxiety and fear when faced with the complex functions of smart devices and operating interfaces, potentially leading to technophobia.2 As a phenomenon associated with technology and psychological issues associated with modern technology,3 technophobia refers to an individual’s irrational anxiety and fear of digital technologies, such as mobile communication devices, artificial intelligence (AI) and robots, and can even result in the avoidance of technology altogether.4 Technophobia has been reported to be a risk factor for impeding health-promoting behaviours in older adults in the digital era.5 In 1996, Celaya6 reported that 20‒33% of Americans experienced technophobia, while a more recent study by Osiceanu7 reported the existence of technophobia in 50% of Americans of different ages, indicating that the number of people who experience technophobia is increasing, not decreasing, over time. Moreover, research on technophobia in older adults has focused mainly on investigating the current situation and its influencing factors,8–11 and with few studies on the mechanisms by which social support can help overcome technophobia in older people in the communities. Social support represents an important means of anxiety alleviation among older adults in urban communities,12 and research on its relationship and associated mechanisms with technophobia has received extensive attention in the fields of psychology and public health. The present study aims to explore the specific associations between social support and technophobia and provide a theoretical and practical basis for improving the physical and mental health of older adults.
The relationship between social support and technophobia
The term social support indicates the social behaviour of a specific social network in providing unpaid help and services to socially vulnerable groups by material or spiritual means and ways.13 Social support network theory holds that the relationship network formed by individuals in social life can provide emotional support, material assistance and information exchange, among other factors, and that these supports are of significant importance in enabling individuals to cope with stress and to improve their quality of life.14 First, social support, as an available external resource, provides a buffering effect on stressed individuals through the internal cognitive system, alleviating the negative impacts of stressful events, which represents an important way of enhancing the health and well-being of older adults.15 At the same time, encouragement from family, friends and other members of the social network enables improved understanding of health-related information, allowing optimal health-related decision-making.16 Research has shown that social support plays an important role in the achievement and maintenance of good mental health.17 The stronger the social support network an individual has, the better they are able to cope with various challenges from their environment, directly reducing the individual’s level of anxiety.18 Technophobia represents a major problem for older adults and requires social support for its alleviation. Therefore, Hypothesis 1 of this study is proposed: Social support has a negative effect on technophobia in older adults.
The mediating role of self-efficacy
Self-efficacy represents a person’s confidence or belief in their ability to perform a task or work behaviour and is a subjective judgemental behaviour.19 Social support theory states that social support is closely related to self-efficacy.20 Social support perceived by individuals can increase their self-efficacy for emotion regulation.21 Additional research has found that self-efficacy can have a direct effect on technophobia. A study of teleworkers during the COVID-19 pandemic showed that e-work self-efficacy buffered the positive effects of technology stressors on symptoms of depressed mood and anxiety.22 At the same time, self-efficacy significantly influenced the perceptions and emotional responses to the use of technology.23 Thus, self-efficacy can influence a person’s evaluations and perceptions of their ability to use e-health technology. In addition, biochemical experiments have shown that high self-efficacy can influence the production of substances, such as catecholamines, that activate the autonomic nervous system, which regulates both immune and neuropsychiatric functions.24 It can thus be inferred that self-efficacy may negatively influence the level of technophobia in older adults. Therefore, Hypothesis H2 is proposed: Self-efficacy mediates the relationship between social support and technophobia among older adults in urban communities.
The mediating role of e-health literacy
e-health literacy indicates the ability of an individual to use electronic media to select, understand and evaluate health-related information and to apply the knowledge gained to solve and manage health problems.25 Research has demonstrated a positive association between the intensity of social software use and e-health literacy.26 Increased online social support received by individuals through the use of electronic devices and social networking sites or software contributes to e-health literacy. In turn, e-health literacy has been positively associated with health-related behaviours.27 The ability of older people to access and use health-related information is linked to an improvement of health perceptions, the development of health-related behaviours, and reduction in anxiety over physical health and the use of digital technology.28 In addition, improving the level of e-health literacy can help older people in urban environments use health-related products and services and assist them in integrating into the digital health society and enjoying the benefits of smart healthcare services, thus reducing their anxiety surrounding the use of technology.29 In summary, e-health literacy functions as a bridge and buffer between social support and technophobia. The positive effects of social support can be enhanced by increasing individual e-health literacy, which in turn alleviates technophobia and improves the quality of life, as well as health behaviours of older people. Therefore, this study proposes Hypothesis H3: e-health literacy mediates between social support and technophobia among older adults in urban communities.
The chain-mediating effect of self-efficacy and e-health literacy
According to Bandura’s theory, individuals with a strong sense of self-efficacy are more inclined to take the initiative in meeting challenges, put in more effort, persevere longer and be more resilient in the face of difficulties.30 This self-regulatory ability enables individuals to set goals, observe behavioural performance, assess the gap between performance and goals, and adjust their behaviour accordingly in the process of improving e-health literacy, thus effectively improving e-health literacy. Therefore, increased support from urban communities enhances the self-efficacy and e-health literacy levels of older adults, reducing the level of technophobia. Therefore, this study proposes Hypothesis H4: Self-efficacy and e-health literacy play a chain-mediating role between social support and technophobia.
Methods
Study design and participants
From June 2023 to April 2024, field research was conducted on older adults in urban communities in Taiyuan, China. A multistage sampling method was used. First, three districts (Ying ze District, Jian cao ping District and Jin yuan District) were randomly selected from six urban districts in Taiyuan, after which three communities were randomly selected from the selected districts using streets as the sampling unit, followed by convenience sampling of older adults aged 60 years and above from the selected communities.
Inclusion criteria: (1) aged 60 years and over; (2) have good hearing and vision, and able to communicate; (3) willing to participate in the study; (4) have lived in the selected communities for 3 years or longer.
Exclusion criteria: (1) have severe organic diseases or mental disorders; (2) unable to communicate; (3) unwilling to participate in the study.
Calculation of the sample size required a ratio of sample size to observed variables of 10:1–15:1. The study included 18 variables (eg, demographic variables). To ensure a 20% sample loss rate and the representativeness and accuracy of data, the sample size was calculated to be ≥216 cases.
Data collection
Professional training was provided to the survey personnel before conducting the questionnaire survey to ensure their familiarity with the survey methods. Before administering the questionnaires, the survey personnel explained the purpose of the survey and filling out the questionnaire to the older adults in the communities and emphasised the anonymity and confidentiality of their responses. After obtaining informed consent from the participants, the survey personnel distributed questionnaires to them one-on-one. Those with the ability to read and write completed the questionnaire themselves, while for participants who were illiterate or had difficulty with completing the questionnaire, the survey personnel read the questions one-by-one and the participants chose their answers which were then recorded by the survey personnel. If the participants experienced difficulty in understanding the questions, the survey personnel provided neutral and accurate explanations and recorded the answers based on the responses. After the collection of the questionnaires, other survey personnel verified the data and checked for any missing information so that missing information could be filled out on-site. A total of 1801 older adults from urban communities were surveyed, of whom 143 were excluded due to missing information or voluntary withdrawal from the study. Finally, 1658 effective questionnaires were included in the analysis, with an effective recovery rate of 93.56%.
Measures
The survey tools used in this study included the following:
Questionnaire on sociodemographic characteristics: this questionnaire comprised items on age, gender, marital status, residential situation, education level, monthly income, self-rated health and frequency of using digital health products.
Technophobia scale: this scale was developed by the American researcher Khasawneh,31 and was translated, back-translated and cross-culturally adapted by Sun et al 32 to the Chinese version, comprising 13 items in 3 dimensions (fear of technology, anxiety about technology, and privacy concerns). The scale is scored using a 5-point Likert scale (5=strongly agree, 4=agree, 3=neutral, 2=disagree, 1=strongly disagree), with a total score of 13–65. A total score of ≥39 indicates a high level of technophobia, while a total score of <39 indicates a low technophobia level. Cronbach’s α of this scale is 0.911, with Cronbach’s α of factors ranging from 0.759 to 0.885 and a split-half reliability coefficient of 0.851. This indicates that this scale has good reliability and validity and was suitable for assessing technophobia in older adults in China.
Questionnaire on e-health literacy: this questionnaire was developed by the Canadian researcher Norman,33 and it was translated, back-translated and cross-culturally adapted by Guo et al 34 to the Chinese version, which comprises eight items in three dimensions (ability to apply online health information and services (five items), critical thinking ability (two items) and decision-making ability (one item)). The scale essentially assesses an individual’s ability to obtain, understand and evaluate health information using electronic devices and to apply the acquired knowledge to handle health issues. It is also scored using a 5-point Likert scale, with a total score of 8–40. A higher total score indicates higher e-health literacy. A total score of 26 is the cut-off and scores <26 indicate lower levels of e-health literacy, while total scores ≥26 indicate high e-health literacy. Cronbach’s α is 0.966 and the factor analysis loading ranges from 0.754 to 0.856, indicating good reliability and validity.
Self-efficacy scale: this scale was translated, back-translated and cross-culturally adapted by Wang et al.35 This scale comprises 10 items and is used to assess the confidence of individuals in overcoming difficulties. It is a 4-point scale, with a total score of 10–40, with scores of 10–20 denoting low self-efficacy, 21–30 indicating medium self-efficacy and 31–40 representing high self-efficacy; thus, higher scores indicate better self-efficacy. Cronbach’s α is 0.87.
Social support scale: this scale was translated, back-translated and cross-culturally adapted by Xiao36 in 1994. It is used to assess the types and degree of assistance and resources obtained from others. It comprises 10 items in 3 dimensions, with a total score of 12–65, with scores of 12–22 denoting low social support, 23–44 denoting medium social support and 45–65 representing high social support; thus higher scores indicate higher levels of social support. Cronbach’s α is 0.73.
Statistical analysis
The data were imported into SPSS V.26.0 for analysis. For descriptive statistics, the number of cases (n) and percentage (%) were used to describe categorical data. In this study, differences between the levels of various major variables in the overall data were examined. The major variables, namely, e-health literacy, technophobia, self-efficacy and social support, were all essentially normally distributed and independent samples t-tests and one-way analysis of variance (ANOVA) were used for comparisons. Based on the literature, factors with statistical significance in the one-way ANOVA were used as control variables. Model 6 in SPSS V.26.0 was used for analysis; this is specifically designed for the analysis of chained-mediation models and enables the testing of multiple indirect effects, including indirect effects arising from M1, those arising from M2 and those arising from both M1 and M2 together. It allows the comparison of the effect sizes of different mediation paths and the assessment of their relative importance in the total effect. Moreover, the process plug-in uses the bootstrap method to test the function of the mediation effect and uses a resampling technique to estimate the CI of the indirect effect, enabling the assessment of the significance of mediation effect, which is a more robust statistical method.
Common method bias test
At the data analysis stage, Harman one-way tests were used for examining the bias of the sample data, and exploratory factor analysis of the four-variable question revealed that 12 factors had an eigenvalue greater than 1. Of these, the first factor had a total variance that explained 34.80%, which is less than the 40% threshold and does not represent statistical bias.
Patient and public involvement
None
Results
Demographic characteristics
The characteristics of the participants are shown that in terms of gender, 907 participants were male, accounting for 54.7%, while 751 participants were female, accounting for 45.3%. A total of 749 participants were aged between 60 and 70 years, accounting for 45.2%, while 641 (38.7%) were aged between 71 and 80 years. In terms of marital status, 679 participants were married, accounting for 41%, and 978 (59%) lived with their families. Overall, 713 (43%) of the older adults had a monthly income above 3000 yuan, with no significant differences in the numbers of participants with income levels of 1000–3000 and those below 1000. In terms of education level, 618 (36.3%) had an educational level of high school or above, while 530 participants were junior middle school graduates, accounting for 32%, and 68 (4.1%) were illiterate. In terms of self-rated health, 716 (43.2%) rated their health as average, while 571 (34.4%) rated themselves as healthy, indicating that the health of the participants was generally good. In terms of frequency of using electronic devices, 683 (41.2%) used electronic devices frequently, and 631 (38.1%) used such devices occasionally.
Influences of demographic characteristics on different variables
As can be seen from table 1, the results of the one-way ANOVA showed that age, residential situation, education level, health and frequency of using electronic devices significantly influenced the incidence of technophobia in older adults, while age, marital status, residential situation, education level, health and frequency of using electronic devices significantly influenced e-health literacy, and age, residential situation, monthly income and education level influenced self-efficacy, and age, marital status, residential situation, education level, self-rated health and frequency of using electronic devices significantly influenced social support in the older adults.
Influences of demographic characteristics on different variables in older adults
Correlation analysis of technophobia, e-health literacy, self-efficacy and e-health literacy
As shown in table 2, there is a significant correlation between social support, self-efficacy, e-health literacy and technophobia. Technophobia was negatively correlated with e-health literacy (r=−0.395, p<0.01), self-efficacy (r=−0.416, p<0.01) and social support (r=−0.377, p<0.01).
Correlation analysis of technophobia, e-health literacy, self-efficacy and social support in older adults
Hypothesis testing
Through correlation analysis, the correlations of variables were preliminarily tested. In this section, hypothesis testing was conducted for further examination of associations between variables. According to the correlation hypotheses proposed above, the direct impact of social support on technophobia was used as the main outcome. On this basis, the chained mediating effects of self-efficacy and e-health literacy were further examined in this model. Additionally, variables that showed significant effects on technophobia in the analysis (age, residential situation, education level, health and use frequency of smart devices) were included in the model as control variables. Model 6 in SPSS V.26 was used for testing. The testing results consisted of two parts, namely, the stepwise regression results and the results of the bootstrap random sampling mediating effect testing. A CI of 95% was used as the threshold. The mediating effect was determined by observing whether the 95% CI includes 0. If the 95% CI did not include 0, the corresponding effect is significant; otherwise, it is non-significant.
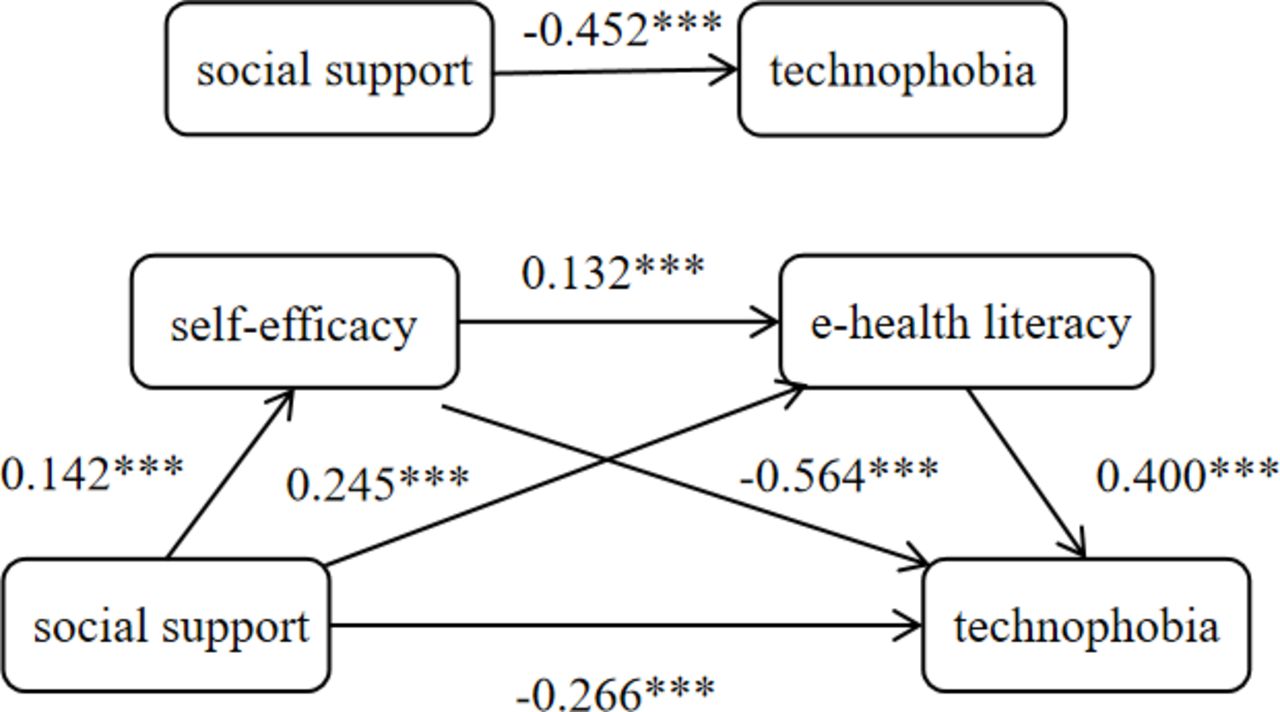
Table 3 shows the mediating effect results obtained from the stepwise regression. In Model 1, social support had a significantly negative influence on technophobia (β=−0.452, p<0.001), suggesting that technophobia in older adults was negatively associated with social support. In Model 2, social support had a significant positive influence on self-efficacy (β=0.142, p<0.001). In Model 3, social support (β=0.245, p<0.001) and self-efficacy (β=0.132, p<0.001) both had significant positive influences on e-health literacy, while in Model 4, social support negatively affected technophobia (β=−0.266, p<0.001), as did self-efficacy (β=−0.564, p<0.001) and e-health literacy (β=−0.400, p<0.001). Overall, the coefficients were significant in all models. Overall, self-efficacy and e-health literacy had mediating effects as partial mediators .
Investigation of mediating effects using stepwise regression
Chain intermediary path analysis
As can be seen from table 4, the indirect effect of the path ‘social support–self-efficacy–technophobia’ was −0.080, and the 95% CI (−0.101 to –0.059) does not include 0. The indirect effect was significant and accounted for 17.7% of the total effect. Self-efficacy thus partially mediated the effect of social support and technophobia. The indirect effect of the path ‘social support–e-health literacy–technology fear’ was −0.098, and the 95% CI (−0.124 to –0.074) does not include 0. The indirect effect was significant, accounting for 21.7% of the total effect. e-health literacy thus partially mediated the effect of social support and technophobia. The indirect effect of the path ‘social support–self-efficacy–e-health literacy–technophobia’ was −0.008, and the 95% CI (−0.011 to –0.004) did not include 0, indicating a significant mediating effect, accounting for 1.8% of the total effect. As shown in figure 1, self-efficacy and e-health literacy played a chain-mediating role between social support and technophobia.
Chained-mediating role of self-efficacy and e-health literacy in the correlation of social support with technophobia in older adults

{kind=link}
Paths of chained mediating effects in older adults in urban communities in Taiyuan, China. ***p<0.001.
Discussion and analysis
The direct influence of social support on technophobia in older adults in urban communities
Our study found that social support is a direct negative predictor of technophobia. The classic buffering hypothesis of social support holds that social support can enhance an individual’s ability to cope with stress and emotional distress by providing psychological, emotional, informational and material resources. The psychological resilience of older adults can be enhanced through encouragement and emotional support from family members and friends, which will enable them to be more independent in the use of digital technology and will reduce their fear and unease when facing complex systems. Greater levels of social support also imply an expansion of the individual’s social networks,37 which can provide older people with access to a variety of resources through which individuals can enhance their skills and technical knowledge, thereby reducing the anxiety associated with unfamiliarity with or inability to master technology. Of course, social support can assist in changing older people’s perceptions of technology.38 For example, having experienced friends or family members around them can not only help older adults understand the value and use of technology but also alter their originally negative cognitive patterns to be more positive when facing technological challenges, thus effectively reducing technophobia. In addition, social support in the form of instrumental support (such as hearing aids, presbyopes and speech recognisers) can alleviate the discomfort that many older people experience as a result of their declining abilities, thus reducing the technophobia that arises when faced with new technology. In addition, instrumental support (such as hearing aids, reading glasses and speech recognition devices) can alleviate the difficulties caused by reductions in physical capability in the elderly. At the same time, social material support, such as smart devices with simple procedures, can effectively reduce the likelihood of intelligent ‘out of control’ during use, potentially alleviating levels of technophobia in older adults. It can be seen that social support can thus directly reduce the levels of technophobia in older adults through different forms.
Roles of self-efficacy and e-health literacy in the correlation of social support with technophobia in older adults in urban communities
Our findings show that social support can influence the level of technophobia in older adults through self-efficacy. This is consistent with the results of a study by Ginja et al 39 showing that the less social support received, the lower the level of self-efficacy and the higher the level of anxiety instead. Self-efficacy is an important mediating variable in the influence of social support networks on the health of older adults.40 Compared with younger age groups, older adults are less receptive to new things and often show a lack of self-confidence when faced with smart health technologies, resulting in lower levels of self-efficacy in the use of these applications. A study on the mental health of urban empty nesters found that social support had a significant negative effect on their psychological anxiety.41 In contrast, older adults with higher self-efficacy were more adaptive and able to deal with new technologies, resulting in better health beliefs, which in turn reduced the level of technophobia. In addition, our findings support that social support can also influence technophobia through e-health literacy. Consistent with the findings of Piccirillo et al,42 the primary reason for this is that social support provides more social networks and increases older adults’ ability to access health resources through smart health technologies, thus strengthening their level of e-health literacy and ultimately reducing their level of technophobia. Indeed, low e-health literacy is an obstacle for older adults in accessing e-health information,43 as it can lead to technophobia and affect their willingness to use and accept new technologies.44 Several studies have attempted to enhance the self-efficacy of older adults by providing them with social support, showing that the overall mood and outlook of the older adults were significantly improved compared with the control group.45 In other words, social support can significantly improve the mental health of older adults and their confidence in the utilisation of information technologies. Interventions to improve self-efficacy were found to be effective in enhancing the e-health literacy of college students during the COVID-19 epidemic.46 However, e-health literacy was negatively correlated with technophobia.47 48 Overall, self-efficacy and e-health literacy were found to have chained mediating effects.
Factors influencing technophobia in older adults in urban communities
Our study showed that there were high to moderate levels of technophobia in older adults in urban communities in Taiyuan, China. This is consistent with the findings of previous studies.49 As they age, older people’s demand for social services increases, while their ability to understand and master new things gradually weakens. They are thus less capable of using digital technology, and the conflict between high demand and low ability further intensifies their feelings of tension, helplessness and resistance, leading to increased technophobia.50 Compared with older adults who live with family, the level of technophobia in elderly people living alone is significantly higher. Lacking emotional and material support, these people may feel unprepared when faced with new technology. In addition, educational attainment provides a knowledge base for the understanding and use of new technology, while health status determines whether an individual can successfully perform the physical and cognitive activities associated with smart devices. Frequency of use also has a direct effect on the proficiency and confidence of the elderly in using smart devices. These factors work together to affect older adults’ acceptance of new technology and their level of technophobia.
Recommendations
First, the government should implement specific plans to address the difficulties faced by the elderly in using intelligent technology, clarify the responsibilities of each department and ensure that the elderly can enjoy intelligent services equally and conveniently. Relevant laws and regulations should be improved to safeguard the privacy rights and security of personal information of older adults when using intelligent technologies. Second, social enterprises should promote the ageing-friendly transformation of intelligent terminal products, in terms of manufacturing them with large screens, large fonts, high volume and large battery capacities, and enabling simple operation that would assist the elderly. In addition, the community could promote knowledge about intelligent technology to the elderly through various means, such as graphics, videos or audio, to increase their confidence and willingness to use it. Volunteers and professional organisations could be organised to provide training on the use of smart devices for the elderly, helping them master basic operational skills. At the same time, family members should spend more time with the elderly and discuss their experiences and feelings about using smart devices, thus enhancing their willingness and confidence in using them and thereby reducing the digital divide and enabling the elderly to enjoy the convenience and benefits associated with technology.
Limitations
In our study, sample was limited to older adults in urban communities in Taiyuan, which may affect the generalisability of the research results. It is difficult to determine causal relationships between the study variables due to limitations inherent in the cross-sectional study design, and the level of technophobia in the elderly was also affected by confounding factors such as the length of time spent using electronic devices, the level of sophistication of the electronic devices, and the elderly themselves. As a result, there may be some bias in the research results. In addition, all participants were informed that the study was investigating social support, self-efficacy, e-health literacy and technophobia. Since the results relied on the self-reports of the participants, this may have introduced a degree of bias. Additionally, factors such as health conditions, traditional culture and living habits may also influence technophobia in older adults. Further investigations are required for a comprehensive elucidation of the causes of technophobia in older adults.
Conclusion
This study visually demonstrates the mechanism by which social support influences technophobia among old adults in urban communities through the construction of a mediation effect model. The independent and chained mediating roles of self-efficacy and e-health literacy in the correlation of social support with technophobia of older adults in urban communities were demonstrated. On a theoretical level, these findings contribute to the understanding of the mechanisms by which social support affects technophobia in older adults, as well as providing new research directions for future studies and advancing research on the psychological health of older adults in the context of smart health. On a practical level, based on the findings of this study, research institutions and social and government agencies, among others, should strengthen cooperation and provide targeted services to older adults in the community to improve their health and well-being.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee of Shanxi Medical University (No. 2023007). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank all the participants in the present study.
References
Footnotes
Contributors DL contributed to the conceptualisation, formal analysis and writing the original draft. JL and CW made contributions to the data curation and verification. YS and HQG contributed to the writing, review and editing. ZGD acts as a guarantor for the final manuscript.
Funding This research received grants from the 2023-2024 Shanxi Province Large Health Industry high-quality development research project (No.:DJKZXKT2023001).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.