Article Text

Abstract
Introduction Due to high workload, shift work and shortage of human resources, nurses are vulnerable to various mental health problems which are significantly related to their physical health, patient safety and healthcare quality. The long-term monitoring of nurses’ mental health and identifying its risk factors are necessary. Accounting for more than one-fifth of global nurses, Chinese nurses have a demanding healthcare workload, especially in tertiary hospitals, yet there is no national cohort concerning their mental health and associated factors. This study (Nurses’ Mental Health Study, NMHS) aims to investigate the mental health of Chinese nurses in tertiary hospitals and to identify the risk and protective factors.
Methods and analysis NMHS is a multicentre prospective cohort study which plans to recruit at least 30 000 registered nurses from 62 tertiary hospitals using the cluster sampling method. Baseline data collection will be implemented through online questionnaires after obtaining informed consent from each participant. Variables including sociodemographic information, work-related factors, health status, lifestyle habits, objective experiences, family and social relations, current affairs opinions and overall evaluation will be collected. Annual follow-up will be conducted via a questionnaire link to monitor subsequent changes in nurses’ mental health and related factors.
Patient and public involvement statement No patient and public involvement in the study design.
Ethics and dissemination This study was approved by the Institute Review Board from the ethical committee of The Second Xiangya Hospital of Central South University (E20230048) and NMHS will be performed in line with Helsinki Declarations. The results of NMHS will inform nursing research and practice by providing evidence to nurse managers, healthcare organisations and the government about the target mental health outcomes for early prevention and intervention.
Trial registration number This study has been registered at the Chinese Clinical Trail Registry (ID: ChiCTR2300072142, https://www.chictr.org.cn/showproj.html?proj=192676).
- Nurses
- MENTAL HEALTH
- Occupational Health Services
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
To the best of our knowledge, this study will be the first cohort study of Chinese nurses concerning mental health, analysing the protective factors and risk factors from multiple dimensions including environmental factors, health behaviour and physical diseases which will provide target outcomes for interventions.
Participants will consist of nurses from all provinces in mainland China, ensuring the representativeness of the whole sample.
Self-reported questionnaires will be used to gain most of the data which may cause recall bias.
There may be selection bias since nurses who refuse to participate in the baseline survey or lost to follow-ups may have different characteristics compared with those who volunteer and stay in the cohort.
Hospitals with beds <2000 will not be included in this study which may cause sample bias.
Introduction
Due to high workload, shift work and shortage of human resources, nurses are vulnerable to various mental health problems, such as depression, anxiety, insomnia, burnout and post-traumatic stress disorder (PTSD).1 2 This situation became worse due to the COVID-19 pandemic and the associated public health pressure, like the stress and workload from frontline healthcare.3 Meanwhile, nurses are also more susceptible to offensive behaviours (eg, workplace violence) than other health professionals,4 resulting in higher stress.5 Mental health problems of nurses are significantly related to their poor physical health,6 decreased patient safety and healthcare quality.7 Therefore, the long-term monitoring of nurses’ mental health and identifying the risk factors of mental health problems would be crucial to their health and the healthcare system. A longitudinal study would be necessary to fully understand the mental health outcomes associated with environmental exposures and work-related factors over time. More than one-fifth of nurses work in China, taking on a non-negligible healthcare role worldwide. However, only two cohort studies focused on Chinese nurses and none of them were concerned with mental health.
Background
According to WHO, mental health refers to a state of mental well-being that enables people to cope with the stress of life, realise their abilities, learn well and work well and contribute to their community.8 Mental health is a continuum including positive and negative states. The positive aspect involves well-being and life satisfaction, while the negative element involves psychopathology, manifesting as mental health problems.9 Mental health problems of nurses include mental disorders and symptoms that affect nurses which may result from biological, economic and social factors.10 Compared with other healthcare professionals, nurses are generally more likely to suffer from mental health problems due to frequent night shifts and heavy workloads, especially after the COVID-19 pandemic.11 Taking care of COVID-19 patients took immense physical and psychological toll on nurses. In addition, healthcare workers were at very high risk of infection during the pandemic which brought extra stress on nurses.12 13 The prevalence of overall mental health problems among nurses was 25–39% during the COVID-19 pandemic, with the prevalence of anxiety, depression, PTSD and burnout being 25.8%, 30.3%, 39.3% and 31.5%, respectively.11 14 15 During the postpandemic period, they still suffer from mental health problems.16 In addition, nurses are vulnerable to compassion fatigue from repeated exposure to patients’ suffering and pain which causes them emotional and physical exhaustion.17 Over 90% of nurses have experienced compassion fatigue and over 70% experienced moderate-to-severe levels.18
The mental health problems of nurses negatively affect their health and are associated with poor patient safety.6 19 It is reported that nurses’ mental health problems may increase the risk of chronic diseases (eg, coronary heart disease, hypertension), tumours (eg, lung/colorectal cancer) and other diseases (eg, systemic lupus erythematosus, Crohn’s disease).6 20–23 Meanwhile, nurses with mental health problems are more likely to experience adverse events than others which threatens patient safety.15 19 As for organisations, mental health problems among nurses are associated with increased absences (eg, sick leave and resignation),24 which would exacerbate the shortage of human resources. Therefore, understanding the risk factors and protective factors of nurses’ mental health problems would be urgent due to the adverse influence on nurses’ health and the healthcare system.
The cohort study design is an appropriate method to clarify protective and risk factors of mental health in nurses. Several cohort studies have been conducted in developed countries, such as the Nurses’ Health Study conducted in America,25 the Japan Nurses’ Health Study26 and the Danish Nurse Cohort.27 In these cohorts, their primary outcome was somatic illnesses, however, depression, anxiety, PTSD and other mental health disorders were included as potential risk factors.6 Evidence has demonstrated that mental health problems (such as depression, anxiety and PTSD) are influenced by multiple factors including individual factors, behaviours, community and policy.6 28–30 However, previous studies of nurses’ mental health mainly relied on cross-sectional evidence.31 32 Besides, mental health problems in nurses from different countries are diverse and findings from cohort studies in other countries are not entirely applicable to Chinese nurses. The current situation of mental health and its influencing factors on Chinese nurses remained little known.
As the world’s second most populous developing country, China boasts a nurse workforce exceeding five million as of 2021,33 more than one-fifth of the global nurses.34 However, the density of nurses (per 10 000 pop) is 33.05 in China, far lower than in developed countries like Australia (137.99), the USA (124.68), Canada (102.70) and the UK (86.86).35 Consequently, Chinese nurses grapple with a demanding healthcare workload, especially those in tertiary hospitals who provide care for patients with complex or rare diseases.36 In addition, the beds and the utilisation rate of beds are higher in tertiary hospitals and over 50% of inpatients and outpatients are in these hospitals.37 Thus, nurses in tertiary hospitals have heavier workloads and pressure, making them even more vulnerable to mental health problems. Up to now, there have been only two cohorts of nurses in China, the Chinese Nurses’ Health Study (The TARGET study)38 and the National Nurse Health Study,39 but both of them only involved nurses in one hospital or one province which could not represent the national circumstances. Therefore, it is necessary to conduct a national multicentred large cohort study of nurses’ mental health.
Study objectives
This study (Nurses’ Mental Health Study, NMHS) aims to investigate the mental health of Chinese nurses in tertiary hospitals and to identify the risk factors and protective factors for nurses’ mental health, by establishing a large-scale cohort of nurses across China. We will include nurses from 62 tertiary hospitals in 31 provinces, indicating good representativeness.
Methods and analysis
Study design and theoretical model
Study design
The NMHS is a nationwide multicentre prospective cohort study and its sample can represent nurses in tertiary hospitals in mainland China. This study will include a baseline survey and longitudinal follow-ups and has been registered on the Chinese Clinical Trial Registry (ChiCTR2300072142, https://www.chictr.org.cn/showproj.html?proj=192676). Figure 1 shows the procedure and overall flow of NMHS. The recruitment and baseline survey were conducted between December 2023 and January 2024.

The procedure and overall flow of the Nurses’ Mental Health Study (NMHS).
Theoretical model
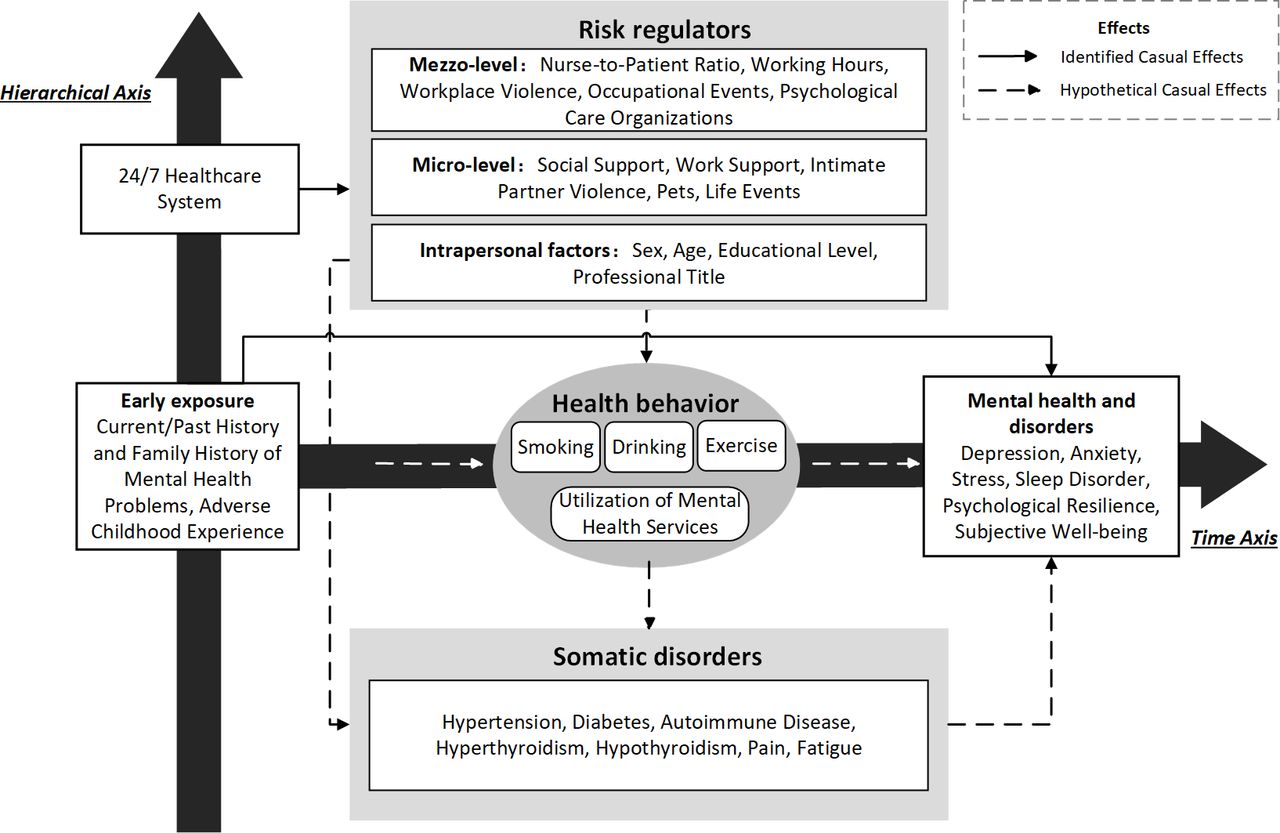
The potential influencing factors of nurses’ mental health will be identified according to the Ecosocial Model by Glass and McAtee40 which directs attention to the biology–environmental interactions on health and health behaviours across the lifespan. Glass and McAtee proposed time axis and hierarchical axis to demonstrate the impact on health outcomes, from multilevel and different life stage.40 The time axis represents one’s life span or a certain period, emphasising the cumulative effects of early exposure. The hierarchical axis demonstrates a multilevel nested system from genes to cells and organs to human behaviour and the environment.40 The theory framework of this study is shown in figure 2.

{kind=link}
{kind=link}
Theory framework for risk factors of nurses’ mental health problems, adapted from Ecosocial Model.40
Study population
Sample size
To detect any events with a proportion as low as 1% with ±0.1% precision (ie, it offered a relative precision of ±10% with a two-side 95% confidence level),41 this study will need to include at least 30 000 nurses.
Sampling criteria
Nurses working in tertiary hospitals in mainland China will be recruited. Inclusion criteria are as follows: (1) at least 18 years old; (2) working full-time as a registered nurse in a tertiary hospital. Exclusion criteria are (1) training nurses (eg, student nurses, nurses in preregistration or standardised training programmes); (2) nurses from other hospitals who are in short-term programmes of specialised certifications (eg, intensive care unit nursing specialists). The determinant factors for mental health are different between student nurses and full-time nurses due to their distinct roles and pressure.42 Nurses in short-term programmes always come from non-tertiary hospitals which are not eligible for inclusion in hospitals. For these reasons, they will be excluded from this study.
Sampling method
A cluster sampling method will be used to recruit participants. First, two tertiary hospitals will be selected from each of the 31 province-level administrative regions (hereafter, ‘provinces’) in mainland China, making up 62 primary sampling sites. Dividing the required sample size (30 000) equally into 62 hospitals in 31 provinces, the baseline recruitment will need to recruit at least 630 nurses in each hospital considering a potential non-response rate of 30%. According to the Guidelines for Medical Service Capacity of Tertiary General Hospitals (2016 Edition) proposed by the National Health and Family Planning Commission of the People’s Republic of China,43 the minimum nurse-bed ratio in tertiary general hospitals is 0.4, which means targeted hospitals in this study will need to have 1575 beds. Meanwhile, given that the biggest hospitals in some remote provinces (eg, Qinghai and Tibet) do not have so many beds, we conservatively decided to choose hospitals with 2000 beds in most provinces, while in others, the target hospitals will be chosen from the top five tertiary hospitals ranked by bed numbers with the same criteria. Thus, the inclusion criteria of hospitals are: (1) having at least 2000 beds except for hospitals in remote provinces; (2) general hospitals capable of dealing with a range of disease types similar to other tertiary hospitals in the provinces. Hospitals unwilling to participate or quit during follow-ups will be excluded.
With hospitals selected, all registered nurses in those hospitals who met the inclusion and exclusion criteria will be invited to participate the study. Since the range of beds among all tertiary hospitals in mainland China is 500∼12 000, the number of nurses in each primary site may vary from 200 to 4800 according to the lowest nurse-bed ratio of 0.4:1.
Procedure
Baseline recruitment
Baseline recruitment and data collection will be performed through online questionnaires via the Wenjuanxing platform which has been widely used in multicentre studies.44 45 Variables including sociodemographic information, work-related factors, health status, lifestyle habits, objective experiences, family and social relations, current affairs opinions, overall evaluation and identification information will be collected. Details of the variables are shown in table 1 and the questionnaire is presented in online supplemental table S2.
Supplemental material
The main variables measured by the online questionnaire and the time points
Directors of nursing departments in each potential primary study site will be invited first through Chinese Nursing Association. Once they agree, their hospital will be officially included as the primary study site and all nurses in the hospital will be recognised as potential participants. Based on the basic hospital information provided by directors of nursing departments, a unique QR code (Quick Response Code) for each hospital, which links to informed consent and online questionnaires will be generated and distributed by two trained researchers. The QR codes will be sent by head nurses to all nursing units in selected hospitals through their wechat group. Eligible nurses in these departments can participate in this study voluntarily. Once nurses log in, they will first be provided with an online informed consent claiming with the following information: (1) this is a national multicentre cohort study concerning mental health and associated factors; (2) after baseline recruitment, there will be annual follow-ups in the next 5 years or longer; (3) the participation is voluntary and they could refuse or quit at any time and could withdraw their data before data analyses; (4) data will only be used for research purposes and will be kept confidentially; (5) personal information (eg, email address, phone numbers) will be carefully stored and only used for follow-up invitation; (6) participating in the study and responding to questionnaires will have no influences on their life or career. Participants could choose ‘agree’ to continue or choose ‘disagree’ to quit. Completing the survey questionnaire indicated consent to join. If the questionnaire is not completed, it is not considered consent to participate and the data for the uncompleted questionnaire will not be saved. Baseline recruitment in each hospital will be finished within 2 months and the whole baseline recruitment in 62 primary study sites will be finished within 3 months.
Follow-up
Participants will receive annual follow-up online questionnaires through a link. The initial duration of follow-ups is 5 years and additional funding applications will be performed to transform this study into a continuing project. Hospitals unwilling to participate or quit during follow-ups will be excluded. However, nurses in those hospitals can still join in follow-ups with online questionnaires sent to them through a link.
Outcomes
The primary outcomes are the mental health status of nurses, including both positive aspects and mental health problems. Specifically, subjective well-being, resilience and life satisfaction will be the three main indicators of positive aspects and depression, anxiety, obsessive symptom/disorder, PTSD, compassion fatigue, self-harm and suicidal behaviours will be the main outcomes for mental health problems. The scales for different mental health variables will be passed to all the participants.
Similar to previous studies,6 symptom burden or incidents of mental disorders will be measured using a Boolean OR operator approach (self-reported clinician-diagnosed disorders or severe symptoms by published cutpoints, such as Patient Health Questionnaire-946). All outcome indicators will be identified using sophisticated self-reported questionnaires and scales. Specifically, mental disorders will be recorded once participants reported newly diagnosed by a doctor during follow-ups. The details of measures and diagnostic criteria for primary outcomes are shown in online supplemental table S1.
Supplemental material
Data management and statistical analysis
Data management and usage
All collected data will be uploaded and stored on an encrypted big data platform by the data manager using a dual entry system. Two independent researchers will perform data cleaning before data analyses which includes three steps. First, the duplicated questionnaires will be removed. If the birth month, phone number and the last four digits of the ID number are all the same in two questionnaires, the one submitted first will be retained. Next, the outlier of the continuous variable will be removed, including numbers less than P25−3IQR and over P75+3IQR.47 Finally, logical conflict checks will be employed. For example, if a participant reported years of work experience more than their age, it will be considered a logical conflict. Questionnaires with over two such conflicts will be excluded. No missing data in this study because the questionnaire can only be submitted after all the items are completed.
After concealing the personal information of participants and basic data cleaning, data per hospital will be opened to themselves. Researchers from participating hospitals can also apply for access to the overall data by submitting study proposals which will be evaluated by professionals and the research team. They are also welcomed and encouraged to make suggestions for the project in light of the local reality.
Statistical analysis
Two main data analyses will be performed using R, Stata and Python software. P value of <0.05 will be recognised as statistically significant. The sample size for specific analysis will be determined by the study aims and calculated based on statistical power. The variables and methods for analyses will be based on the theoretical model in figure 2.
The first set of analyses will describe the overall mental health status of Chinese nurses, including the characteristics and trends over time. Mean (SD) or median (interquartile spacing) will be used for continuous variables, while number and frequency (percentage) for categorical variables. Latent variable analysis and disease trajectory analysis will be used to describe trends and changes in mental health over time.
The second set of analyses will identify influential factors that protect or threaten nurses’ mental health and generate and test prediction tools for different indicators of mental health. To achieve this, a comparison of differences between groups will be performed using a t-test, analysis of variance for continuous variables conforming to normal distribution, non-parametric test for continuous variables with non-normal distribution and χ² test for categorical variables. Correlation analysis will be used to test correlations between variables. Cox proportional risk models and logistic regression models will be used to identify risk factors for nurses’ mental health from individual, interpersonal, organisational and environmental perspectives. Prediction models will be generated using machine learning algorithms (eg, K-Nearest Neighbour, Naïve Bayes models and random forest models48) while the performance of different models will be compared using the area under the receiver operating curve, prospective prediction results and decision curve analysis.
Quality control
Sampling control
This study uses whole group sampling and all nurses within that hospital who met the criteria are invited to complete the survey after the hospital was selected. The Wenjuanxing platform will record the number of participants with non-consent or non-completion anonymously.
Data quality control
Before the survey, the study team conducted several rounds of expert consultation and revised the questionnaire. The self-assessment questionnaire will be quality-controlled through the system. The reliability of the questionnaire will be assessed using questionnaire reliability, logical verification of the questionnaire data and composite assessment of multiple data sources.
Lead unit quality control
The research team will conduct regular meetings with research site leaders (nursing directors of each hospital) to check on the progress of the research. Meanwhile, irregular annual on-site inspections will be performed by project consultants and technical staff from the lead unit to ensure the quality of data collection.
Handling of adverse events and emergencies
Assessment of risk for suicide and self-harm behaviour: If nurses are at high risk for anxiety, depression, self-harm and suicide assessed by the self-reported questionnaire, the page after completing the questionnaire will show access to professional mental health services. In addition, the research team will provide them with a professional self-care manual through email and the details can be found in online supplemental table S3. They will also be recommended for further diagnosis and treatment in specialised hospitals or institutions.
Each project site should record other unintended or adverse events (eg, strong issues about this study, unexpected death of nurses by suicide or other accidents and turnover of nurses) and report to the lead unit timely. The study team will revise the operation manual based on feedback.
Supplemental material
Ethics and dissemination
This study obtained ethics approval by the Institute Review Board from the ethical committee of The Second Xiangya Hospital of Central South University (Ethics approval number: E20230048). Before data collection, the purpose and content of the study will be fully explained to the participants and informed consent will be obtained from each participant. Participants in the baseline survey and follow-up studies will be offered ¥1∼100 (US$0.13701∼13.701) randomly as thanks for completing questionnaires through online WeChat payment. This study will be performed in line with the protocol, Chinese law and Helsinki Declarations. Participants are free to join or refuse and they will be formally included only after giving fully informed consent. Participants will have the right to quit the study at any time, yet their data can be withdrawn only before data analyses which will not harm their health or career. The study reported in this paper will not involve the use of any animal or human tissue. All data will be kept anonymously and only used for this study. The findings of NMHS will be disseminated through peer-reviewed journals and national and international conferences.
Patient and public involvement statement
Patients or the public will not be involved in the design, or conduct, or reporting, or dissemination plans of our research.
Discussion
To the best of our knowledge, this study may be the first to establish a large cohort of Chinese nurses concerning mental health. We will analyse the protective factors and risk factors including policy, health behaviour, work-related factors and somatic disorders, and construct a risk prediction model of nurses’ mental disorders. The results of our study will offer a long-term observation and an accurate understanding of the mental health trajectories of nurses over time, providing researchers and nurse managers with significant mental health outcomes which will be a scientific basis for implementing targeted interventions. Moreover, our study will provide scientific evidence for the government to formulate macro prevention and control policies for nurses’ mental health problems and ultimately improve the mental health of nurses and improve nursing quality and patient safety.
Current status of this study
The baseline recruitment was conducted between December 2023 and January 2024. The follow-up procedure will start one year after.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors All authors contributed to the study conceptualisation. MN: Writing—original draft; Writing—review and editing; Visualisation. XL: Writing—review and editing; Visualisation. ZC, JY, QY, CH, YC, YT: Writing—review and editing. Y-ML: Methodology; Funding acquisition; Resources; Supervision; Validation; Project administration. SX: Methodology. Y-ML is responsible for the overall content as the guarantor.
Funding This work was supported by the STI2030-Major Projects (2021ZD0200700) and the Scientific Research Project of Health Commission of Hunan Province (W20243200). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note Co-first authors: Meng Ning and Xuting Li contributed equally to this work.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.