Article Text

Abstract
Objectives This study aimed to dissect the aetiological subgroups of postpartum haemorrhage (PPH) that occur after vaginal delivery in women with full-term singleton pregnancies. Our goal was to craft and validate predictive models to guide clinical decision-making and optimise resource allocation.
Design A retrospective cohort study.
Setting Shengjing Hospital of China Medical University, Liaoning Maternal and Child Health Hospital, and Shenyang Women’s and Children’s Hospital.
Participants 29 842 women who underwent vaginal delivery were enrolled in the study across three hospitals from 2016 to 2022.
Primary outcome measures PPH, categorised into uterine atony (UA), placental factors (PF), cervical trauma (CT), and coagulation abnormalities (CA) by aetiology.
Results The logistic regression for overall PPH and UA-PPH showcased high discrimination (AUCs of 0.807 and 0.794, respectively), coupled with commendable calibration and DCA-assessed clinical utility, culminating in the development of a nomogram for risk prediction. The PF-PPH model exhibited a modest AUC of 0.739, while the CT-PPH and CA-PPH models demonstrated suboptimal clinical utility and calibration.
Conclusion The study identified factors associated with PPH and developed models with good performance for overall PPH and UA-PPH. The nomogram offers a valuable tool for risk prediction. However, models for PF-PPH, CT-PPH, and CA-PPH require further refinement. Future research should focus on larger samples and multicentre validation for enhanced model generalisability.
- Maternal medicine
- PERINATOLOGY
- Postpartum Women
- PREVENTIVE MEDICINE
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study included data from large multicentre cohorts in China, comprising 29 842 women to enhance the statistical power of the analysis.
Predictive models were developed for postpartum haemorrhage following vaginal delivery and for different aetiological subgroups.
The predictive models were visualised using nomograms for clinical application.
This study’s test set is a single-centre study specifically focused on vaginal delivery PPH, with a limited number of positive samples.
The existing external validation datasets are from hospitals of the same region and level, resulting in a lack of diversification and generalisability.
Background
Postpartum haemorrhage (PPH) is defined as blood loss exceeding 500 mL within 24 hours following vaginal delivery or exceeding 1000 mL within 24 hours following caesarean delivery.1 PPH is a widespread and serious medical condition that poses significant risks to women’s health around the world. It is particularly devastating in developing countries, where it is a principal contributor to maternal mortality.2 It is estimated that approximately 1.4 million maternal deaths globally are tied to PPH each year, with the tragic loss of a woman’s life to this condition occurring every 4 min.3 4 In Australia, the incidence of PPH increased from 6.3% in 2000 to 8.0% in 2009.5 Similarly, in the USA, the rate of PPH rose from 2.7% in 1999 to 3.2% in 2014.6 In China, despite a relatively lower maternal mortality rate of 17.8 per 100 000 in 2019, PPH accounted for one-quarter of these deaths.7
The WHO has conducted an analysis revealing that while PPH is a significant factor in maternal mortality and morbidity, the mortality rates vary considerably across different regions.4 In high-income countries, the risk of death due to PPH is significantly lower than in low-income countries.8 In high-income nations, the substantial blood loss primarily caused by PPH accounts for 13.4% of overall maternal mortality, while in Africa and Asia, this figure stands at 34% and 30.8%, respectively.4 The international obstetric community is actively engaged in research to better understand the incidence, risk factors, and management strategies for PPH.9–11 Despite the establishment of global clinical guidelines and the identification of various risk factors, further exploration is needed to enhance our understanding and management of PPH.12 13
PPH can be aetiologically classified into uterine atony (UA), placental factors (PF), cervical trauma (CT), and coagulation abnormalities (CA), each requiring distinct clinical management and treatment strategies.14 Clear aetiological classification is crucial for developing preventive strategies, formulating management plans and rational allocation of medical resources.15 While numerous cohort studies have focused on identifying risk factors for PPH, there is a scarcity of studies that quantify and weigh these risk factors for a comprehensive PPH risk assessment.16 17 Given the complexity of PPH and the interplay of multiple risk factors, a holistic approach is necessary to accurately assess the risk of PPH.
Clinical prediction models (CPMs) have been widely applied in clinical settings in recent years. By constructing CPMs, physicians and patients can make better medical decisions, and health departments at all levels can allocate medical resources more rationally. These models play an irreplaceable role in primary prevention (assessing the quantitative risk of future diseases) and secondary prevention (constructing highly sensitive and specific diagnostic schemes, practicing ‘early detection, early diagnosis, early treatment’), reflecting significant health economic value.
There is a gap in research regarding the development of clinical prediction models for women specifically following vaginal delivery. Many studies are constrained by limited sample sizes, which can affect the robustness of the models.18 Other research has focused on PPH prediction models for women undergoing caesarean sections.19 Our study aims to address this gap by constructing a clinical prediction model tailored to PPH after vaginal delivery. By analysing clinical data and risk factors through logistic regression, we can determine the relative impact of each factor on the likelihood of PPH. We further refined our model by performing secondary fitting based on the four aetiological subgroups, creating a nomogram that enhances the precision of predicting high-risk populations for PPH. This work provides essential insights for the prevention and management of this critical condition.
Materials and methods
Data sources and ethics statement
This cohort study was conducted at the obstetric wards of Shengjing Hospital of China Medical University, Liaoning Maternal and Child Health Hospital, and Shenyang Women’s and Children’s Hospital. The study population comprised women who underwent vaginal delivery between 1 January 2016 and 31 December 2022. The outcomes of interest were fetal birth outcomes within the first 24 hours postpartum. Inclusion criteria were women who consented to participate after being informed of the study’s scope. Exclusion criteria were defined as follows: age under 18 or over 50 years, delivery occurring at less than 37 weeks or more than 42 weeks of gestation, multiple births and instances of induced labour, stillbirth or fetal death. These factors were excluded to focus on women with full-term, singleton pregnancies undergoing vaginal delivery. Preterm and postterm pregnancies, multiple pregnancies and induced labour are associated with different physiological characteristics and obstetric risks, which could confound the analysis of PPH risk in this cohort. Additionally, stillbirth and fetal death involve other pathological processes and significant complications that are outside the scope of this study’s focus on live births and PPH risk.
Comprehensive data encompassing maternal characteristics, obstetric and gynaecological history, pregnancy complications, and details of the delivery process and neonatal conditions were collected. To protect participant privacy, all data were anonymised. The study protocol was approved by the Ethical Review Committee of Shengjing Hospital of China Medical University (No. 2016PS344K), and written information about the study was provided to all participants.
Sample size calculation
According to the obstetric big data from Shengjing Hospital of China Medical University, the incidence of PPH is approximately 6%–7%. Based on the sample size estimation using the p sample size package in R software, the minimum sample size required for constructing clinical prediction models is estimated to be between 1048 and 1536. The sample size included in this study far exceeds the minimum requirement.
Covariates
A range of covariates were taken into account, including: (1) age, categorised as <25, 25–29, 30–34 and ≥35 years; (2) ethnicity, divided into Han, Manchu and others; (3) education level, classified as high school or below, bachelor’s degree and postgraduate or above; (4) occupation, categorised as unemployed, light physical labour, moderate physical labour and heavy physical labour (based on the International Physical Activity Questionnaire, IPAQ); (5) monthly household income per capita, divided into <0.5, 0.5–2.0, 2.0 –5.0 and >5.0 thousand yuan; (6) prepregnancy BMI, categorised as underweight (<18.5 kg/m2), normal (18.5–23.9 kg/m2), overweight (24–27.9 kg/m2) and obese (≥28 kg/m2); (7) smoking and alcohol consumption history; (8) gravidity, categorised as 1, 2 or ≥3 times; (9) parity, divided into 0, 1 or ≥2 times; (10) history of miscarriage and induced labour; (11) assisted reproductive technology; (11) gestational age, categorised as <38, 38–40 and >40 weeks; (12) pregnancy complications: diabetes, hypertension, anaemia, coagulation disorder, uterine fibroids/adenomyosis, polyhydramnios, umbilical cord entanglement, premature rupture of membranes, placental abruption, vaginal bleeding during pregnancy and scarred uterus; (13) delivery time, divided into day time (8–16), evening (17–23), and night (0–7) shifts; (14) total duration of labour, categorised as normal (≤24 hours) and prolonged (>24 hours); (15) latent phase of the first stage, categorised as normal (primiparous ≤20 hours, multiparous ≤14 hours) and prolonged (primiparous >20 hours, multiparous >14 hours); (16) active phase of the first stage, categorised as normal (≤ 8 hours) and prolonged (>8 hours); (17) second stage duration, categorised as normal and prolonged based on specific criteria for primiparous and multiparous women with or without analgesia; (18) third stage duration, categorised as normal (≤30 min) and prolonged (>30 min); (19) placental retention/placenta accreta/placental implantation; (20) analgesia during labour; (21) instrumental assistance in delivery; (22) lacerations of the cervix, vagina or perineum and (23) newborn weight and length.
Aetiology subgroups
In this study, PPH was defined according to WHO standards as blood loss exceeding 500 mL following vaginal delivery. Patients were categorised into those with and without PPH based on this definition, and further analysis was conducted on the underlying aetiologies, including UA, PF, CT, and CA.
Model construction
For the purpose of our investigation, we have categorised the participants from the Shengjing hospital of China Medical University as Cohort I. This cohort was systematically split into a training dataset and an internal validation dataset with a ratio of 7:3. The training dataset was instrumental in developing the predictive model, while the internal validation dataset served to assess the model’s predictive accuracy. An additional cohort, comprising participants from two other hospitals, was designated as Cohort II. This external dataset was used to validate the model’s general applicability and its efficacy in real-world clinical scenarios.
Within the confines of the datasets, we employed both univariate and multivariate logistic regression analyses to identify potential risk factors across various subgroups. These factors were then subjected to a rigorous selection process for inclusion in the predictive model. The selected factors were further analysed using multivariate logistic regression (bidirectional elimination) in training dataset to discern their discriminative power, thereby establishing them as predictive indicators for the model. The women in the training set were divided into PPH and non-PPH groups based on PPH as the outcome variable. Subsequently, they were further categorised by aetiology into UA-PPH and non-UA-PPH groups, PF-PPH and non-PF-PPH groups, CT-PPH and non-CT-PPH groups, and CA-PPH and non-CA-PPH groups. Five predictive models were constructed sequentially, and the performance of these models was corroborated using both the test and validation datasets to ascertain the most accurate predictive model.
Evaluating the performance of the models
The area under the receiver operating characteristic curve (AUC) was the primary metric used to evaluate the discrimination of our models. An AUC value above 0.75 suggests excellent model discrimination, while an AUC below 0.6 indicates poor discrimination. Calibration curves were used to assess the models’ accuracy, with closer alignment between observed and predicted incidence rates indicating higher model fidelity. Decision curve analysis (DCA) was also employed to evaluate the clinical utility of the models, offering a thorough assessment of the models’ net benefits across various clinical scenarios.
Nomogram development
Nomograms for postpartum haemorrhage and its four aetiological subgroups were crafted to offer a visual representation of the risk scores derived from the logistic regression analysis. This tool simplifies the interpretation of complex statistical outcomes, providing a more straightforward approach to understanding risk assessments.
Statistical analysis
All statistical computations, construction of traditional logistic models and calculation of model discrimination and calibration were carried out using R V.3.6.3 from the R Foundation for Statistical Computing, Vienna, Austria. This software facilitated the development of traditional logistic predictive models and their subsequent evaluation for discriminative power, calibration and clinical utility. Continuous variables conforming to the normal distribution were expressed as the mean±standard deviation (SD), while non-normally distributed continuous variables were presented as medians with interquartile ranges. Categorical data were analysed using χ2 tests, and continuous variables were analysed using ANOVA or Mann-Whitney U tests, as appropriate. Variables were adjusted as dummy variables, and OR with corresponding 95% CI were calculated using univariate and multivariate logistic regression analyses, with significance level set at p<0.05.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
From 2016 to 2022, a total of 27 389 patients underwent vaginal delivery at the Shengjing Hospital of China Medical University. Forty-two patients under 18 years of age or over 50 years were excluded. Additionally, 2456 patients with gestational age less than 37 weeks or more than 42 weeks at delivery, 6 patients with multiple births and 52 patients with induced labour, stillbirth or fetal death were also excluded. Ultimately, 24 833 patients met the inclusion criteria and were enrolled in the cohort. According to the inclusion and exclusion criteria, a total of 5099 patients in Cohort II were included in the external validation dataset. The general characteristics of all patients are presented in table 1. All patients were followed up within 24 hours after delivery for neonatal outcomes, with a follow-up rate of 100%. The patient selection criteria flowchart is shown in figure 1.
The general view of the maternal

Patient selection criteria flowchart.
Comparison of basic characteristics and risk analysis for postpartum haemorrhage (PPH) and its subgroups
Based on the occurrence of postpartum haemorrhage, the parturients in Cohort I were divided into two groups: the non-PPH group and the PPH group. Similarly, within the aetiological subgroups, they were categorised into UA-PPH and non-UA-PPH groups, PF-PPH and non-PF-PPH groups, CT-PPH and non-CT-PPH groups, and CA-PPH and non-CA-PPH groups. The comparison of basic characteristics and analysis of risk factors for each group are presented in online supplemental file table 1–5.
Supplemental material
In the multivariate analysis of risk factors, apart from age, parity, prepregnancy BMI, anaemia, premature rupture of membranes, and combined placenta retention/placenta accreta/placental implantation, other specific risk factors were found to be associated with specific aetiologies of postpartum haemorrhage. For instance, polyhydramnios was associated with UA-PPH; analgesia during labour, instrumental assistance, and cervical/vaginal/perineal lacerations were associated with the occurrence of CT-PPH (table 2).
Multivariate risk factor analysis for postpartum haemorrhage (PPH) within subgroups
Selection of predictive factors for PPH and its subgroups in the training dataset
Through random sampling of Cohort I, 70% of the data (n=17 383) from parturients were used to form the training dataset, with the remaining approximately 30% (n=7450) forming the internal validation dataset. Multivariate analysis of risk factors for PPH and its subgroups was performed again in the training dataset, with results presented in online supplemental table 6. After selection, predictive models were constructed for each group using the selected risk factors.
Supplemental material
Evaluation of predictive model discrimination
The ROC curves were plotted using R software for the PPH group and its various subgroups across the training dataset, internal and external validation dataset.
The results indicated that the predictive models, namely PPH-Logistic, UA-PPH-Logistic, PF-PPH-Logistic, CT-PPH-Logistic and CA-PPH-Logistic, demonstrated high discriminative power in the training dataset with AUCs of 0.807 (95% CI: 0.792 to 0.821), 0.794 (95% CI: 0.777 to 0.811), 0.796 (95% CI: 0.761 to 0.830), 0.935 (95% CI: 0.901 to 0.969), and 0.802 (95% CI: 0.769 to 0.892), respectively (figure 2A–E). However, the PF-PPH-Logistic model exhibited only moderate discrimination with an AUC of 0.739 (95% CI: 0.666 to 0.813) in the internal validation dataset. Furthermore, the CA-PPH-Logistic model showed significantly lower discrimination in the external validation dataset with an AUC of 0.662 (95% CI: 0.450 to 0.873), which was notably inferior to its performance in the training and test datasets. This discrepancy may be attributed to the lower proportion of patients with coagulation disorders causing PPH in the validation dataset.

AUC Curve for Postpartum Haemorrhage (PPH) Group and four subgroups. (A) PPH Group; (B) Uterine Atony PPH Group; (C) Placental Factors PPH Group; (D) Cervical Trauma PPH Group; (E) Coagulation Abnormalities PPH Group. The blue line signifies the training dataset, which is employed to evaluate the model’s predictive capabilities following the training phases. The green line corresponds to the internal validation dataset, pivotal for refining model parameters and for conducting initial assessments of the model’s accuracy. The purple line denotes the external validation dataset, which is utilised to ascertain the model’s generalisability and to verify its performance in an independent dataset.
Assessment of predictive model calibration
Calibration curves for the PPH and its subgroups were plotted for the Logistic predictive model within the training dataset (online supplemental figure 1A–E). The performance of the PF-PPH-Logistic, particularly the CT-PPH-Logistic, and CA-PPH-Logistic models was suboptimal in certain aspects, with lower calibration, as observed in the test and external validation datasets (online supplemental figure 1F–J, online supplemental figure 1K–O).
Supplemental material
Evaluation of clinical utility of predictive models
In the evaluation of clinical utility, the PPH-Logistic and UA-PPH-Logistic models demonstrated satisfactory performance across all datasets. However, the clinical utility of the PF-PPH-Logistic, CT-PPH-Logistic, and CA-PPH-Logistic models was found to be relatively poor (online supplemental figure 2A–O).
Supplemental material
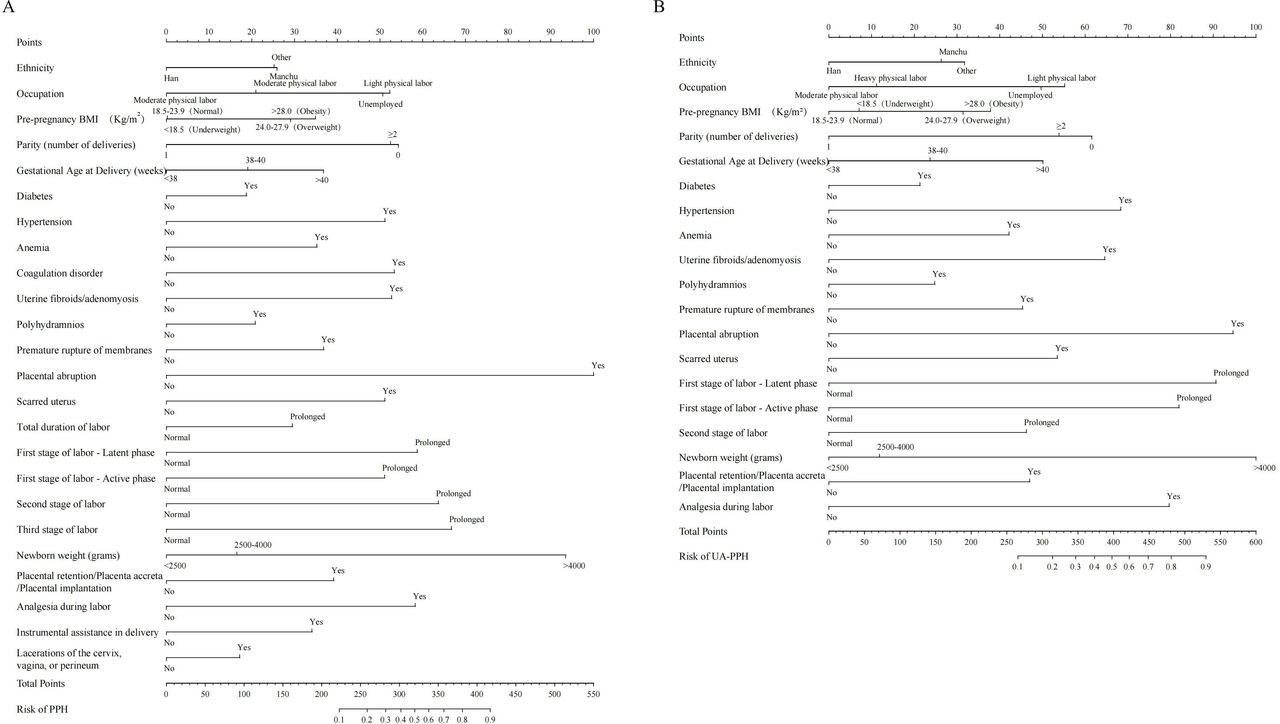
Nomogram construction
Using R software, we constructed nomograms for PPH and UA-PPH, with the results presented in figure 3A–B. Physicians can assess the risk probability of PPH occurrence by summing the individual scores on the nomogram. This practical tool aids in a more precise estimation of PPH risk, thereby, enhancing clinical decision-making.

{kind=link}
{kind=link}
{kind=link}
Nomograms for Postpartum Haemorrhage (PPH) and Uterine Atony PPH Group. A. PPH Group; B. Uterine Atony PPH Group.
Discussion
Maternal mortality has emerged as a pivotal indicator in global maternal and child health, serving as a significant benchmark for assessing the socioeconomic status of nations. Consequently, the effective reduction, prevention, and improvement of conditions leading to maternal deaths have become a focal point for public health initiatives worldwide. Among the various causes of maternal mortality, PPH stands out as a preventable condition that has attracted considerable attention.16 17 With the rise in global economic standards and the evolution of medical technologies, there has been approximately 50% decrease in the worldwide maternal mortality rate between 1990 and 2015. In China, the maternal mortality rate has seen a dramatic reduction of 98.78%20 since the establishment of the People’s Republic of China. Despite these advancements, a substantial proportion of maternal deaths, estimated between 27% and 40%,21 remain avoidable due to a range of factors, including inadequate social and medical interventions. PPH is a critical area of focus within this context, and the prediction and prevention of PPH to reduce avoidable maternal mortality present a significant challenge on the global stage.
Early prediction or identification of PPH and timely preventive or intervention measures are extremely valuable, necessitating a clear understanding of the aetiologies of PPH for targeted management. The overall PPH model provides a comprehensive perspective that captures common risk factors for postpartum haemorrhage, offering a baseline risk assessment for women. This broad assessment helps in formulating general preventive measures and policies, ensuring that all women at risk of PPH are monitored. Although the overall PPH model demonstrates higher overall accuracy, it may mask the heterogeneity between different PPH subtypes in clinical practice, limiting its guidance for individualised management. Subtype-specific models, on the other hand, can delve deeper into the specific risk factors of each subtype, helping to enhance our understanding of the potential mechanisms of PPH and meet the diverse needs of clinical practice. The value provided by these models in treatment is more critical, as they can guide clinicians to adopt effective therapeutic strategies tailored to the specific aetiology, thereby reducing complications and mortality and promoting the development of precision medicine. In this study, the predictive models developed for PPH and UA-PPH demonstrated excellent performance in effectively identifying high-risk populations. For women at high risk for UA-PPH, early cord clamping should be considered. After the placenta is delivered, uterine fundal massage can be performed, and oxytocin should be administered immediately to promote uterine contraction and reduce bleeding. If necessary, mechanical compression or uterine artery ligation can be employed for haemostasis. In other PPH subtype models, the performance may be suboptimal due to factors such as insufficient positive sample sizes, requiring further sample expansion and model optimisation to enhance predictive ability and improve the general applicability of the models. Overall, high-risk women for PPH should be closely monitored, and proactive interventions should be implemented, such as promoting uterine contractions, advising patients to avoid excessive straining that could cause lacerations, and timely correction of coagulopathy.
The advent of the big data era has brought new opportunities for the management of PPH. The era is characterised by the digitisation and standardisation of medical records, along with an increasing volume of data, which has ushered in an era of data-driven management and treatment for maternal care. Leveraging big data analytics for disease risk prediction can contribute to the reduction of avoidable maternal deaths.
A review of the literature reveals over 200 prognostic models in obstetrics, three of which are pertinent to PPH.22 However, few models have been applied in routine clinical practice, and the majority of studies have not provided model formulas, hindering independent external validation. The earliest PPH prediction model, dating back to 1994, originated from a case-control study in Zimbabwe,23 where PPH was defined as blood loss exceeding 600 mL following an unassisted vaginal delivery. This study included 150 PPH patients and 299 patients with normal deliveries, with a low positive predictive value of less than 7% and only 35.0% of patients experiencing postpartum bleeding. Since then, approximately ten additional PPH prediction models have been published. These models have varied in focus, with some concentrating on the relationship between placenta previa and PPH, while others have included only vaginal deliveries23–26 or caesarean sections,19 27 28 and some have targeted women with placental implantation disorders29 or general obstetric populations.30 PPH research has been conducted in hospitals across various countries, including Italy, China, France, the USA, the United Kingdom, South Korea, the Netherlands, Spain, Zimbabwe, Denmark, and Egypt. From the 14 published studies, a total of 124 independent variables were identified as potential predictors (ranging from 5 to 38 per study), and 64 variables were ultimately selected for the final models (an average of 5 to 15 factors per study). Common predictors included parity, low pre-pregnancy haemoglobin, antenatal bleeding, maternal age over 35, gestational age, high neonatal weight, multiple pregnancies, body mass index (BMI) over 25, previous caesarean section, anterior placenta, and retained placenta. These predictors have also been incorporated into our predictive model.
Once a clinical prediction model is developed, it must undergo validation and evaluation to assess the model’s effectiveness, reproducibility, and portability. Published PPH prediction models have reported AUCs ranging from 0.7024 to 0.9026, with external validation AUCs of 0.83,19 which are comparable to the results of our study. In addition to discrimination, calibration is essential to evaluate the consistency between the predicted probabilities of clinical outcomes and the observed event probabilities. Only a few studies, such as one by Albright in 2019 on the prediction of PPH following caesarean section, have utilised calibration curves,19 while most have employed the Hosmer-Lemeshow goodness-of-fit test to compare predicted probabilities with actual event probabilities for significant differences. The Hosmer-Lemeshow test, however, has limited efficacy in small-sample prediction models as it does not quantify model calibration31 32 or provide direction or magnitude of miscalibration.33
The decision curve analysis (DCA)33 has been used to evaluate the clinical utility of models, focusing on the selection of true positives from positive patients to avoid unnecessary medical resource consumption and reduce harm from overtreatment of false positives. DCA is particularly suitable for scenarios where symptoms suggest the possibility of disease but a diagnosis has not yet been confirmed, guiding the decision on whether or what kind of screening method to adopt for disease diagnosis. The DCA’s axes represent the threshold probability (P) and net benefit (NB), allowing for the determination of intervention measures based on the predicted probability of adverse events.34
In essence, both ROC and DCA can be used to assess the quality of predictive models, but they differ fundamentally in their theoretical constructs. While ROC combines sensitivity and specificity to compare the accuracy of predictive models through the AUC, the highest AUC does not necessarily represent the optimal model in clinical practice. For instance, in this study, patients in the CA-PPH group, due to coagulation disorders, all underwent caesarean section deliveries to minimise the number of false positives. This requires decision-makers to consider practical issues, as a high ROC does not always indicate the best treatment approach. Furthermore, for some extreme cases, the accuracy of ROC becomes less critical, and DCA evaluation results are needed for reference.
Statistical analysis of previously published PPH data has shown that factors such as general anaesthesia in pregnant women, prolonged use of oxytocin, excessive uterine tension (multiple pregnancies, polyhydramnios), and chorioamnionitis are all associated with uterine atony, potentially increasing the risk of postpartum bleeding. Previous studies have suggested that for pregnant women with high-risk factors, assessing and selecting appropriate treatment options and management based on the type and weight of different risks can reduce the risk of adverse pregnancy outcomes or death.35 Early prediction and intervention are key measures in reducing maternal mortality, with studies finding that timely intervention can effectively lower maternal mortality rates by 10%.36 Establishing a model that predicts the risk of PPH following vaginal delivery and guides clinical practice is a significant task for maternal and child health.
Limitation
Although some subtypes in this study showed promising predictive results, the clinical application of the logistic regression models for the PF-PPH, CT-PPH and CA-PPH groups is limited by insufficient positive sample sizes in these subgroups, which prevents fully achieving the initial goal of aetiology-based PPH prediction. Compared with previously published models, this study’s test set is a single-centre study focusing specifically on vaginal delivery PPH, with a limited number of positive samples. Additionally, the external validation datasets come from hospitals of the same region and level, lacking diversity and generalisability. Therefore, future plans include multicentre collaboration, increasing sample sizes, and seeking higher-quality prediction methods to provide more robust clinical evidence.
Furthermore, the PPH scoring model developed in this study is not applicable to women with preterm or postterm labour, induced labour, or multiple pregnancies. These populations have unique physiological and pathological factors, along with higher complication rates, that fall outside the scope of this study. Further research is needed to develop individualised risk assessment models for these groups. It is important to note that these models incorporate not only antepartum factors but also postpartum factors such as labour characteristics and newborn weight. This comprehensive approach aids in understanding the mechanisms of PPH and provides a basis for targeted prevention or intervention strategies aimed at risk factors. However, these models are not entirely suitable for antepartum clinical decision-making or real-time prediction.
Conclusion
In conclusion, our study has successfully developed and validated predictive models for PPH following vaginal delivery, offering a novel approach to risk assessment in this critical area of maternal health. The models, particularly for overall PPH and UA-PPH, demonstrated high discriminative power and clinical utility, with the nomogram providing a user-friendly tool for clinicians. Despite the promising results, limitations exist in the application of the PF-PPH, CT-PPH and CA-PPH models due to the insufficient positive sample size in these subgroups. The generalisability of our findings may also be limited by the single-centre nature of the study and the regional characteristics of the included hospitals. Future research should aim to expand the sample size and include multicentre data to improve the models’ applicability and robustness. This study contributes to the growing body of evidence on PPH management and has the potential to influence policy and practice, ultimately enhancing maternal care and outcomes.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics approval and consent to participate: The study was approved by the Ethics Committee of Shengjing Hospital of China Medical University (No. 2016PS344K, Date.17/12/2016). All participants provided informed consent. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions. We would like to acknowledge that Jinke Li and Dandan Zhang have contributed equally to this work.
References
Footnotes
JL and DZ contributed equally.
Contributors JL, DZ and YZ designed the study and drafted the manuscript. HL, MS, and XW done the data collection. YZ and XC designed the statistical analysis plan. DZ has participated the training and reviewed and co-authored the manuscript with ZS. All authors have read and approved this manuscript. ZS is responsible for the overall content as guarantor.
Funding This study was supported in part by grants from 345 Talent Project of Shengjing Hospital of China Medical University (No. M0946), and Medical Education Research Project of Liaoning Province (No. 2022-N005-03).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.