Article Text

Abstract
Objective This study aimed to assess gender-based violence and associated factors during the time of armed conflict among female high school students in Kobo administration town, North Wollo, Ethiopia.
Study design An institutional-based, quantitative and cross-sectional study was conducted.
Setting This research was carried out in Kobo town, North Wollo, Ethiopia high schools.
Study participants This study was conducted among 422 female high school students in Kobo administration town at time of armed conflict from May 20 to 5 June 2022.
Outcome measures Gender-based violence (GBV) was assessed using a self-administered questionnaire. Data were entered in Epidemiological data (EPI-Data) V.3.1 and exported to SPSS V.25 for analysis. A binary logistic regression model was used to identify significant factors associated with GBV.
Results The magnitude of GBV among female high school students at Kobo town during armed conflict was 45%, with 95% CI 40.2% to 49.8%. Students with poor current academic performance (Adjusted Odds Ratio (AOR)=3.001; 95% CI 1.335 to 6.750), students with a family member who participated in conflict (AOR=1.809; 95% CI 1.135 to 2.882), students with a family member who was subjected to conflict (AOR=1.954; 95% CI 1.164 to 3.281), students who drank alcohol (AOR=8.158; 95% CI 4.325 to 15.386) and students who did not freely disclosing reproductive health issues (AOR=3.267; 95% CI 1.509 to 7.075) were more likely to suffer GBV.
Conclusions The magnitude of GBV during the armed conflict was high. Variables such as poor academic performance, family members who participated in the war, family members subjected to the war, students who drank alcohol and not freely discussing reproductive health issues were statistically associated with GBV. It is recommended to put in place programmes that address factors such as academic challenges, alcohol use, family trauma and the need for open discussions on reproductive health to help to reduce GBV.
- Crime
- Adolescents
- Behavior
- Dysmenorrhea
Data availability statement
Data are available upon reasonable request. The dataset used and analysed during the current study is available from the corresponding author, BTA upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Timely and relevant topic, addresses a critical issue of gender-based violence (GBV) during a specific period.
Focusing on female high school students allows the study to highlight a specific group that may be especially vulnerable.
Reliance on self-reported data may introduce bias, as participants may under-report experiences of violence due to stigma.
Studying a specific location (Kobo administration town) provides insight into the local factors influencing GBV.
This study focused on violence against female high school students at the time of armed conflict, rather than examining general violence against women throughout their lives.
Introduction
Gender-based violence (GBV) refers to violence against women, often involving a combination of physical, psychological and sexual violence.1 The WHO claims that GBV against women is a serious violation of human rights.2 Due to a number of variables, it is typical among women and girls who have experienced war.3 Women who are displaced refugees and living in conflict-affected areas are particularly vulnerable.2 It is estimated that pooled prevalence of GBV among refugees and internally displaced women was determined to be 48.20%.4 Another systematic review and meta-analysis study conducted among female students in Ethiopian higher education institution revealed that about 51.42% of female students were experienced lifetime GBV.5 Depending on the type of incident that was recorded, between 83 and 102 million women (45–55% of women) in the 28 European member states had experienced sexual harassment since the age of 15 years.6 People living in areas affected by conflict are concerned by the prevalence of violence worldwide.7 As a result, violence is the most widespread yet least recognised human right in the world.8
Women are more susceptible to GBV in wartime, which frequently includes rape and sexual exploitation and can lead to kidnapping.9 Numerous reports of violence against women have been presented worldwide. In armed situations, rape and other GBV are increasingly being employed as weapons of war.10 When violence was employed as a weapon of war, conflict-related sexual violence developed in Rwanda, Bosnia and Herzegovina.11 Students in conflict-affected areas are more likely to be attacked or kidnapped, and their academic performance suffers, particularly when girls begin to reach adolescence.12 All children have a fundamental right to access high-quality education, which is also a requirement for socioeconomic advancement and the eradication of poverty.13 Armed groups target girls for sexual assault and threaten their education, either directly as a result of a crisis or inadvertently as a result of harm.14 The issue of GBV in conflict environments is becoming more prevalent.15 One of history’s ‘great silences’ has been described as the brutality committed during conflicts against women and girls.16
The broad definition of this crime, which includes rape and sexual assault, raises serious concerns for communities from all socioeconomic strata. Victims experience psychological problems, alcohol and drug addiction, and severe gynaecological problems.17 18 According to a 2019 study conducted by the University of Oxford on the effects of the Israeli-Palestinian conflict, the significance of both the effect of conflict on academic achievement and the mechanisms underlying such possible effects is particularly high for high school students.19 A number of factors, such as alcohol consumption in relation to GBV, are multifaceted and complex and affect individuals’ behaviour, predisposing them to violent behaviour.20 Wartime violence against women can have detrimental effects on both short-term and long-term health.21 Additionally, it has detrimental effects on the reproductive health of the population and negatively affects sexual health, including unintended pregnancies, STDs, HIV/AIDS and sexual dysfunction.22 One of the factors contributing to GBV in conflict contexts is the rise in conditions brought about by war, such as displacement and economic disruption23
Most violent acts in emergencies go unreported due to a lack of health and support services, making it difficult to fully understand the scope of violence against women and girls in conflict areas. Additionally, previous studies have not adequately adjusted for key risk factors for GBV.24 Therefore, this study provides information about the magnitude of GBV and associated factors during armed conflict among female high school students in Kobo administration town.
Methods and materials
Study design, period and setting
An institutional-based cross-sectional study design was employed from May 20 to 5 June 2022.
Based on information taken from the district human resource administrative office, Kobo administration town is one of the Woreda administrations in the Amhara region, Ethiopia. It is located in the northeast corner of Amhara, bordered on the west by Gidan, on the north by the Tigray region, and on the east by the Afar Region. It is located approximately 567 km from Addis Ababa and 403 km from Bahir Dar. It has a total population of 57 737, and there are 2990 female high school students in the town. The town has three high schools: one private and two governmental schools.
Study participants
The source population includes all female students enrolled in high schools in the Kobo administration town during the period of armed conflict. All female high school students in Kobo administration town who were available during the study period were the study participants.
Inclusion criteria
All female high school students currently attending school in Kobo administration town, North Wollo, and who have provided informed consent.
Exclusion criteria
Male students, non-students, individuals without parental/guardian consent, students from outside the Kobo administration town were excluded from the study.
Sampling size determination
The single population proportion formula was used to calculate the required sample size using the lifetime prevalence of GBV among female high school students (47.2%) from the study conducted in Debre Birhan Basso High School24 considering 95% CI and 5% margin of error, which resulted in a total of 422 students.
Sampling technique and procedures
Stratified sampling was performed. First, the school was stratified by considering each grade level as a stratum. Proportion to population size sampling was then used to allocate the required sample from each stratum. Student’s grades and classes were randomly selected until the required sample size was fulfilled (figure 1).

Schematic diagram showing the sampling procedure for assessing gender-based violence and association factors during armed conflict among female Kobo high school students, North Wollo, Ethiopia, 2023.
Dependent variable
Gender-based violence (yes/no).
Independent variables
Independent variables included sociodemographic variables (age, religion, grade level, pocket money, academic performance, relationship status, living condition, parental educational status and family control), behavioural factors (alcohol drinking, chat chewing and cigarette smoking), sexual experience before the time of armed conflict (sexual history and free discussion of reproductive health with family) and war-related factors (family involvement in the war and family members subjected to war crime).
Variable measurement and definition of terms
Gender-based violence
Defined in this study as a form of violence that targets students’ experiences of physical, sexual or psychological violence perpetrated against female students.25 26
Sexual violence
Defined as any act on a female student physically forcing her to have sexual intercourse, forcing her to perform any other sexual acts and forcing her with threats or in any other way to perform sexual acts without her consent. At least one ‘yes’ answer to the three items classified the woman as experiencing sexual violence.27
Physical violence
In this study, physical violence was defined as any physical harm, including being slapped, pushed, fist/kicked, chocked/burnt, hurt using a gun/knife or dragged against female students. One ‘yes’ answer from the six items classified the student as experiencing physical violence.26 27
Psychological violence
Defined as the female student being made to feel bad about herself or insulted, humiliated in front of others, intimidated and intentionally subjected to inappropriate comments. At least one ‘yes’ answer to the four items indicated that the person was experiencing psychologically violent acts.27
During armed conflict
The time from the invasion of Kobo by the Tigray people invasion force from the beginning of August 2021 to the liberation of Kobo from the Tigray people invasion force at the end of December 2021.
Academic performance
Students who scored ≥80 are rated good, those who scored between 50 and 80 are rated average and those who scored below 50 are rated poor for academic performance.
Data collection tools and procedures
A formal, self-administered questionnaire was created based on the goals of the study. It was adapted from previous study.24 An expert in both languages translated the questionnaires into Amharic, and another person then translated them back into English to verify its consistency. Data were gathered using an interviewer-administered, pretested and structured questionnaire. The questionnaires were created with many questions examining students’ sociodemographic traits, sexual experience, behavioural aspects and GBV experience during conflict.24 Three diploma midwives and two BSc midwives from the Gidan Woreda Health Centres received training in supervision and data collection. A supervisor with a BSc in midwifery and the principal investigator continuously followed the data collection process. They were responsible for the overall data collection process and checked the consistency and completeness of the collected data.
Data processing and analysis
After data collection, the completed questionnaires were coded. The data were entered using Epidemiological data (EPI-Data) V.3.1 statistical software and analysed using SPSS V.25. Data cleaning was performed to check for frequencies, accuracy, consistency and missing values and variables. Incomplete and inconsistent data were excluded from the analysis. Descriptive analyses, such as proportions, percentages, means and measures of dispersion, tables and graphs, were used to describe the data. Binary logistic regression model was used. The goodness of model fitness was tested by Hosmer-Lemshow (0.829).
First, variables with p values <0.25 in bivariable logistic regression analysis were entered into multivariable logistic regression. Multivariable analysis was then used to examine the association between dependent and independent variables. A significant independent factor was being declared at the 95% CI and p value <0.05.
Data quality control
To ensure the quality of the data, training was provided to the data collectors and supervisors for 2 days on the objective, relevance of the study, respondents’ rights, informed consent and interview techniques. Before data collection, a pretest was performed on 5% (21) of the total sample size at Gidan Woreda Mujja High School randomly selected to ensure reliability and the standard of the questionnaire. Each questionnaire was checked for completeness and missing values; incomplete questionnaires were omitted from the analysis.
Ethical considerations
This study was approved by the Institutional Research Ethics Review Committee of Debre Markos University, College of Medicine, and Health Sciences, and ethical approval was obtained from the board. Written informed consent was obtained from each participant. Consent for participants under 18 years of age was obtained from a parents or legal guardians. To ensure confidentiality, the names and addresses of students were not recorded during data collection. None of the investigators had access to the collected data. The investigator only used the collected data to answer the stated objectives. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Patient and public involvement
Study participants were not involved in the design, conduct, reporting or dissemination plans of our research.
Results
Sociodemographic characteristics
A total of 411 female students completed the self-administered questionnaire out of the total of 422 students invited to participate in the study, a response rate of 97.4%. The mean age of the respondents was 17.32±1.3 years, with a minimum age of 14 and a maximum of 22 years. More than half of the respondents (54.5%) were under the age of 18 years. Most of the respondents (370, 90%) were followers of orthodox religion. Regarding academic performance, almost two-thirds, 261 (63.5%) of students were average, 95 students (23.1%) were good or above average and 55 students (13.4%) were poor (table 1).
Sociodemographic characteristics of respondents in Kobo high school female students, North Wollo, Ethiopia, 2023 (N=411)
The proportion of respondents who indicated that they consumed alcohol, chewed tobacco and smoked cigarettes was 89 (21.7%), 43 (10.5%) and 1 (0.2%), respectively (table 2).
Substance abuse/use related behaviours for assessing gender-based violence and associated factors during the armed conflict among Kobo high school female students, North Wollo, Ethiopia, 2023 (N=411)
Sexual experiences/history before the armed conflict
Among the total of 411 respondents, 22 (5.4%) had experienced sexual intercourse before war time and 51 (12.4%) freely discussed reproductive health with their parents
Prevalence of GBV
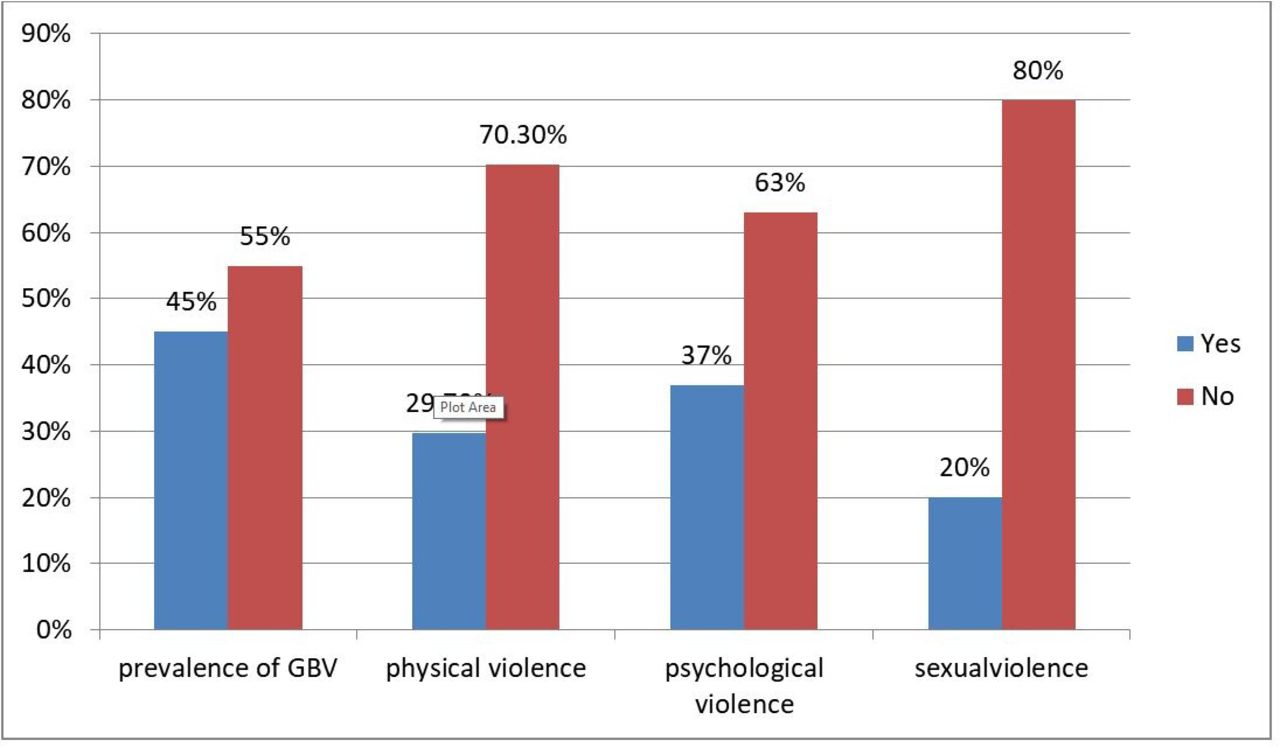
At least one type of GBV (psychological, physical and/or sexual violence) during armed conflict was found to be 45% (95% CI 40.2% to 49.8%). There were 152 (37%) students who experienced psychological violence (95% CI 32.3% to 41.7%), 122 students (29.7%) who experienced physical violence (95% CI 25.3% to 34.1%) and 82 students who experienced sexual violence (20.1%) (95% CI 16% to 24%) (figure 2).

{kind=link}
{kind=link}
The magnitude of GBV for those who experienced at least one type of violence and each type of violence among female Kobo high school students, North Wollo, Ethiopia, 2023 (N=411).
Psychological violence
Among students who experienced psychological violence, 108 (71.1%) reported being insulted, 37 (24.3%) reported being humiliated in front of others, 50 (32.9%) reported being intimidated and 33 (21.7%) reported being subjected to inappropriate comments. 91 (60%) instances of psychological violence were committed by an armed person and 71 (46.7%) of the violent crimes occurred on public streets
Physical violence
A total of 77 (63.1%) participants reported something being thrown at them, while 75 (61.5%) were shoved, 33 (27%) were fist-kicked, 21 (17.2%) were choked or burned, 31 (25.4%) were verbally threatened with a knife or pistol and 14 (11.5%) were pulled (online supplemental table 1).
Supplemental material
Sexual violence
When it came to sexual violence, nearly all of the incidents (82, 100%) involved unwanted sexual contact, the majority of whom were perpetrated by an armed person (44, 53.7%) and nearly half of them (36, 43.9%) were committed at home (online supplemental table 2).
Supplemental material
Factors associated with GBV
In the bivariable analysis, age, grade level, having a boyfriend, current academic performance, family control, chewing chat, drinking alcohol, having a female friend, involvement of family to defend the war, having a family member subjected to war and freely discussing their personal issues were all eligible predictor variables to enter into the multivariable logistic regression analysis. In the multivariable logistic regression analysis, current academic performance, involvement of family in defending war, family members subjected to war, drinking alcohol and freely discussing reproductive health with parents were significantly associated with GBV among female high-school students in Kobo administration town.
Students with poor current academic performance were three times more likely to be exposed to GBV than those with good and above-average academic performance (Adjusted Odds Ratio (AOR)=3.001; 95% CI 1.335 to 6.750).
Students whose family members fought or defended during the war were 1.8 times (AOR=1.809; 95% CI 1.135 to 2.882) more likely to experience GBV than those whose family members did not fight or defend during the war. Similarly, student’s family members subjected to war were two times (AOR=1.954; 95% CI 1.164 to 3.281) more likely to experience GBV compared with those students who did not have family members subjected to war.
Female high school students who reported drinking alcohol were about eight times more likely to experience GBV than those who did not drink (AOR=8.158; 95% CI 4.325 to 15.386)).
Students who did not freely discus personal issues, including reproductive health, with their parents, were three times (AOR=3.267; 95% CI 1.509 to 7.075) more likely to experience GBV as compared with those who freely discussed personal issues, including reproductive health (table 3).
Bivariable and multivariable logistic regression analysis of factors associated with gender-based violence among Kobo administration town female high school students, North Wollo, Ethiopia (n=411)
Discussion
Among all study participants, about 45%, (95% CI 40.2% to 49.8%) reported having experienced at least one type of GBV. Specifically, this is one of the first analyses of violence among high school students at time of the armed conflict. The high prevalence of GBV among students is a cause for concern because it may alter their behaviour and impair their academic performance. GBV was not a new scenario, but the increased severity and incidence of war can result in higher levels of GBV against women and girls, including arbitrary killings, torture, sexual violence and forced marriage during conflict.
In addition to the strengths of this study, it is vital to acknowledge methodological limitations that should be considered. First, the relatively limited sample size may restrict the degree to which our findings can be generalised to larger populations. Second, the cross-sectional design of the study inherently limits our ability to draw causal inferences. Longitudinal studies are essential for a more comprehensive exploration of causality. Furthermore, there exists the potential for selection bias, as participants were exclusively sourced from a single geographic locale, which may not encapsulate the heterogeneity of other demographic groups. Lastly, the dependence on self-reported data raises concerns regarding the potential for response bias, which could compromise the precision of the outcomes. These constraints indicate that, although our findings are encouraging, further investigations using larger, more heterogeneous samples and longitudinal methodologies are requisite to validate and expand on this conclusion.
The finding in this study was in line with those of previous studies conducted in Debre Berhan (47.2%),24 and Debre Markos Town (47.0%)25 and among females in refugees and internally displaced women, 48.20%.4 This resemblance may be explained by the fact that the conflict has resulted in notable amounts of violence, and that our study lasted only 5 months, which is typical of lifetime frame studies.
This study finding was higher compared with the Demographic Health Survey on domestic violence (33% in 2016),28 and the lifetime prevalence of intimate partner violence (IPV) in Ethiopia (37%).2 This might be due to differences between the study populations, study areas and study periods. In this study, including high school students during war was different from those that only studied domestic violence (even if major violence) and different from the WHO study of only sexual and physical violence of IPV, because we expected war-affected areas to have greater burdens of GBV.
Similarly, this study result was also higher compared with a study in Somalia during conflict in which 35.6% experienced physical or sexual IPV in adulthood,29 and 35.1% in South East Nigeria.30 The main reason for this study may be that only IPV was studied in Somalia and only physical and sexual violence was studied in both Nigeria and Somalia. Another possible explanation might be the socioeconomic and environmental factors.
This study result was lower than that in studies conducted in the Cote d’Ivoire 2014 armed conflict (57.1%),31 in East Hararghe zone (54.9%),32 in Hadiya Zone (62.20%)33 and in Aleta Wondo town, southeast Ethiopia (68.2%)34 and systematic review and meta-analysis study conducted among female students in Ethiopian higher education institution (51.42%).5 A possible explanation for this finding may be the time reference. For example, the current study measured GBV in 5 months during war, whereas other studies measured the lifetime frame. The second explanation might be that the study in Cote d’ Ivoire during conflict involved IPV of all females, whereas our study was only conducted with high school students.
Overall GBV (psychological, physical and sexual) was further analysed to determine possible associations with the independent variables.
Accordingly, poor current academic performance, family involved to defend against war, family members subjected to war, alcohol drinking and not freely discussing reproductive health issues with parents were statistically significant factors of GBV.
Students with poor academic performance were three times more likely to suffer GBV than those with good or higher performance. This finding is in agreement with another study conducted among Bahir Dar City female high school students; those who had poor educational performance were three times more likely to experience GBV than those who had good educational performance.26 Other studies were conducted in Menkorer High School, Debre Markos35 and among high school students in Baso, Debre Berhan and Ethiopia.24 This might signify that good school achievement among female students was found to be protective against GBV, while the problem of GBV is sustained and aggravated during war.
This finding is in line with studies conducted at University of Oxford in 2019 on the effect of the Israeli-Palestinian conflict among high school students.19 This may be due to the worsening of students’ psychological well-being as a result of their direct exposure to violent events.
Students whose family members participated in war were 1.8 times more likely to experience GBV than those with family who did not participate. This could be due to armed perpetrators taking revenge on the family members or violating the dignity of females, families, and societies because of the families’ defence of war. In addition, they may be used as weapons of warfare against enemy families and communities.
Similarly, students with family members subjected to war were twice as likely to experience GBV compared with students who did not have family members subjected to war. The possible explanation for this could be that the female student was exposed to the chance of violence because she spent time with their family during the war or when armed members attacked their family, and therefore she might also be victim to psychological, physical or sexual violence.
Female high school students who reported drinking alcohol were approximately eight times more likely to experience GBV than those who did not drink alcohol. This study is supported by studies conducted in Debre Markos Town,25 in East Ethiopia,27 in Dilla Town36 and in Mombasa, Kenya,37 which could be due to the relationship between alcohol drinking andGBV, which is the effect of alcohol use on the occurrence of violence. Impaired judgement of students who drink alcohol mean they might engage in different activities, such as visiting harmful places and being unaware of the possible dangers that may expose them to sexual violence and other risks.
Students who did not freely discussed reproductive health were 3.3 times more likely to experience GBV than those who did discuss reproductive health issues. This study was supported by studies conducted in Bahir Dar City at night with students,26 in Gondar38 and in Debre Berhan.24 The reason could be the lack of awareness of the consequences of gender-related health issues and lack of family protection because discussion of sexual reproductive health issues between family and students is one of the best ways to create awareness to prevent violence.
Conclusions
From the findings of this study, the overall magnitude of GBV among Kobo female high school students was high compared with other studies within the study period. Nearly half of the students experienced at least one incident of violence against female high school students during the armed conflict.
Current academic performance, family involvement in the war, family members subjected to the war, alcohol consumption and freely disclosing reproductive health were statistically significant. Moreover, learning about the effects of war on female students is crucial for a better understanding of the impact of violence on the development prospects of an economy, given that these students will constitute a large part of the country’s highly skilled workforce in the future. It is recommended to put in place programmes that address factors such as academic challenges, alcohol use, family trauma and the need for open discussions on reproductive health to help reduce GBV.
Data availability statement
Data are available upon reasonable request. The dataset used and analysed during the current study is available from the corresponding author, BTA upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was obtained from the Institutional Review Board of the Debre Markos University Health Science College Ethical Review Committee. A description of the purpose of the thesis and an offer to answer all inquiries were provided to the respondents. Written informed consent was obtained from all participants. Consent for participants under 18 years of age was obtained from a parents or legal guardians. They also acknowledged that they were free to withdraw their consent and discontinue their participation. The privacy and confidentiality of the collected information were ensured throughout the process, and no personal identifiers were used.
Acknowledgments
Our deepest gratitude goes to Debre Markos University for providing the opportunity to conduct this study. Finally, we express our appreciation to the data collectors and supervisors for their efforts.
Footnotes
Contributors GAA and BTA made substantial contributions to the conception and design, acquisition of data, and analysis and interpretation of the data. GDA and MWA were involved in drafting the manuscript and/or revising it critically for important intellectual content. All authors read and approved the final manuscript. BTA is the guarantor of the works for any aspect.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer-review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.