Article Text

Abstract
Objectives To assess the association between depression and suicide attempt (SA) by age and region.
Design Cross-sectional study.
Setting First Affiliated Hospital of Wannan Medical College from January 2021 to January 2022.
Participants Hospitalised patients.
Primary outcome measures SA was the primary outcome and data on SA was obtained from the electronic medical records of hospitalised patients.
Methods and analysis In this study, data on inpatients of the First Affiliated Hospital of Wannan Medical College from January 2021 to January 2022 were extracted from the medical record system using the convenience sampling method. According to the exclusion criteria, 7593 eligible research subjects were obtained. Logistic regression analysis was used to assess the association between depression and SA, combining age and region. Subgroup analyses were carried out to assess the relationship between age, region and SA in depressed patients, after excluding non-depressed patients, and to inspect the interaction of age and region. Finally, further comparisons of the disparities in suicide patterns among different age groups and regional groups were made.
Results Among 7593 patients (3630 males), 655 (8.6%) patients with SA were observed. We found that depression was significantly associated with SA by age and region (all p<0.05). Specifically, depressed juveniles and adults had a higher risk of SA compared with non-depressed adults, and ORs (95% CIs) were 2.62 (1.59 to 4.30) and 1.67 (1.30 to 2.13), respectively. Furthermore, rural individuals with depression, urban individuals without depression and urban individuals with depression had a higher risk of SA compared with rural participants without depression, and ORs (95% CIs) were 1.60 (1.22 to 2.12), 1.29 (1.04 to 1.61) and 2.53 (1.83 to 3.49), respectively. In subgroup analyses, we further found that depression was strongly associated with SA in juveniles (OR 2.84, 95% CI 1.19 to 6.76, p=0.018) and urban patients (OR 1.67, 95% CI 1.15 to 2.40, p=0.006). Notably, the predominant methods of suicide among individuals with depression were the utilisation of sleeping pills or antidepressants.
Conclusion Our study found individuals with depression are at higher risk of SA, especially juveniles and urban individuals. Effective integration of mental health and urban–rural services could mitigate the risk of suicide and contribute to better outcomes.
- AUDIT
- Suicide & self-harm
- Depression & mood disorders
- Adolescents
Data availability statement
The data underlying this article cannot be shared publicly due to the privacy of individuals who participated in the study. The data will be shared on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study used subgroup analysis and logistic regression analysis to investigate the relationship between depression and attempted suicide.
This study was conducted in a single province and city in China; therefore, the results should be extrapolated to other provinces and cities with caution.
This study did not include several potentially important covariates, such as education and parental information.
Introduction
Suicide represents a significant global public health issue. The prevalence of suicide deaths has witnessed a concerning rise worldwide, with a 6.7% increase between 1990 and 2016.1 The WHO reports that over 700 000 people lose their lives to suicide each year, and more than 10 million individuals attempt suicide, ranking as the fourth leading cause of death among individuals aged 15–29 years old.2 Depression is one of the most common mental diseases associated with suicide.3–5 In 2015, the WHO reported that over 3.22 million individuals worldwide experienced depression, with more than half of suicides or suicide attempts (SA) preceded during periods of depression.6 Although extensive studies have been conducted on the correlation between depression and suicide rates worldwide,7–12 given the grim form of SA, the relationship still needs further study.
Previous studies regarding depression and SA have mainly concentrated on the risk factors of SA among patients with depression, such as sleep quality,13 14 negative emotions,15 anxiety5 14 16 and social support.17 Studies have also explored the relationship between depression and SA within specific groups, such as adolescents,18 19 university students,20 high school students,21 the elderly22 and military personnel.9 In China, while the suicide rate among individuals over 25 years old has been decreasing, the suicide death rate among individuals aged 5–14 has seen an alarming increase from 2010 to 2021.23 Adolescents, constituting one-sixth of the global population, are particularly vulnerable due to their immaturity and emotional sensitivity, making them more susceptible to suicidal ideation, self-harm and SA.24 Currently, most studies on SA have focused singularly on either adolescents or adults, with limited evidence regarding the differences between the two populations.25–27
Furthermore, the disparity between the SA in urban and rural areas has been a contentious topic. Rural areas often face more challenging social, economic and cultural conditions compared with urban areas, resulting in higher suicide rates.28 29 This finding has been supported by 24 previous studies conducted in different countries.28 However, several studies have also indicated that the incidence of SA is higher in urban areas compared with rural areas.30 31 Given the inconsistent evidence, policy development and social support are limited.
Therefore, this study aimed to use a large-scale clinical sample to explore the association between depression and SA by age and region. By identifying the specific characteristics of suicide within different groups, targeted prevention strategies can be developed to effectively address this pressing public health issue.
Methods
Study design and setting
This study was a large-sample clinical research that used data from patients admitted to the First Affiliated Hospital of Wannan Medical College. It used a convenience sampling method to extract the medical data of inpatients from January 2021 to January 2022 in the medical record homepage system. This approach was based on practical considerations including data stability issues due to a system upgrade and COVID-19 lockdown, as well as resource constraints. The 1 year research period allowed for intensive data handling within our limitations, with an extra month added to compensate for reduced patient numbers during lockdown. In the current study, participants aged <11 and >85 years (n=44 308), serious physical diseases (n=51 812), repeated hospitalisations (n=8642), death records (n=1012), migrant
population (n=827) and other serious mental illnesses (n=296) were excluded. Finally, 7593 individuals were included in the final analysis (figure 1).

Flowchart of the study.
Primary outcome
Suicide attempt
SA was defined as a form of suicide in which an individual had a will to terminate their own life but did not die.32 In the current study, SAs were collected from electronic medical records of patients who were hospitalised for suicide behaviour, including the use of pesticides, antidepressants, sleeping pills, other medications, cutting tools, carbon monoxide poisoning and other methods.
Depression
In this study, depressed patients were identified according to the International Classification of Diseases code ICD-1033 from the homepages of the medical record.
Covariates
Socio-demographic and clinical information included sex (male and female), marriage (single, married and others), occupation (students, farmers, retirees, unemployed and others), taking antidepressants (yes or no) and chronic diseases (diabetes, hypertension, hyperlipidemia, stroke, coronary heart disease, thyroid dysfunction and chronic obstructive pulmonary disease).
Patient and public involvement
None.
Statistical analysis
Frequency and percentage were used for categorical variables, and mean and standard deviation (X±SD) were used for continuous variables. Logistic regression analysis was used to examine the association between depression and SA, combining age and region. Bootstrap sampling was performed by randomly sampling 90%, 80% and 70% of the sample size to ensure the robustness of the association between depression and SA. The sizes of the resampled samples were 6834, 6074 and 5315, respectively.
Furthermore, subgroup analyses were performed to assess the association of age and region with SA in depressed patients, excluding non-depressed patients and examined the interaction of age and region. Finally, we further compared the differences in suicide patterns between different age groups and regional groups.
SPSS 27.0 and R 4.3.3 software were used for all analyses. A two-sided p<0.05 was considered statistically significant.
Results
Among 7593 participants, 1290 (17.0%) depressed patients were observed and 655 (8.6%) suicide attempts were recorded. SA patients were more likely to be married females, as well as unemployed farmers. Furthermore, SA patients were more likely to be urban adults. More details are shown in table 1.
Sociodemographic and clinical characteristics (n = 7593)
In logistic regression analysis, it was found that age, region, depression, sex, occupation and the number of chronic diseases all had statistically significant impacts on SA (online supplemental figure 1). In this study, individuals with depression were more likely to have SA compared with those without depression (OR 1.42, 95% CI 1.16 to 1.74). Urban residents showed a higher risk of SA than rural residents (OR 2.77, 95% CI 2.32 to 3.30), and juveniles were more prone to SA than adults (OR 1.75, 95% CI 1.08 to 2.83).
Supplemental material
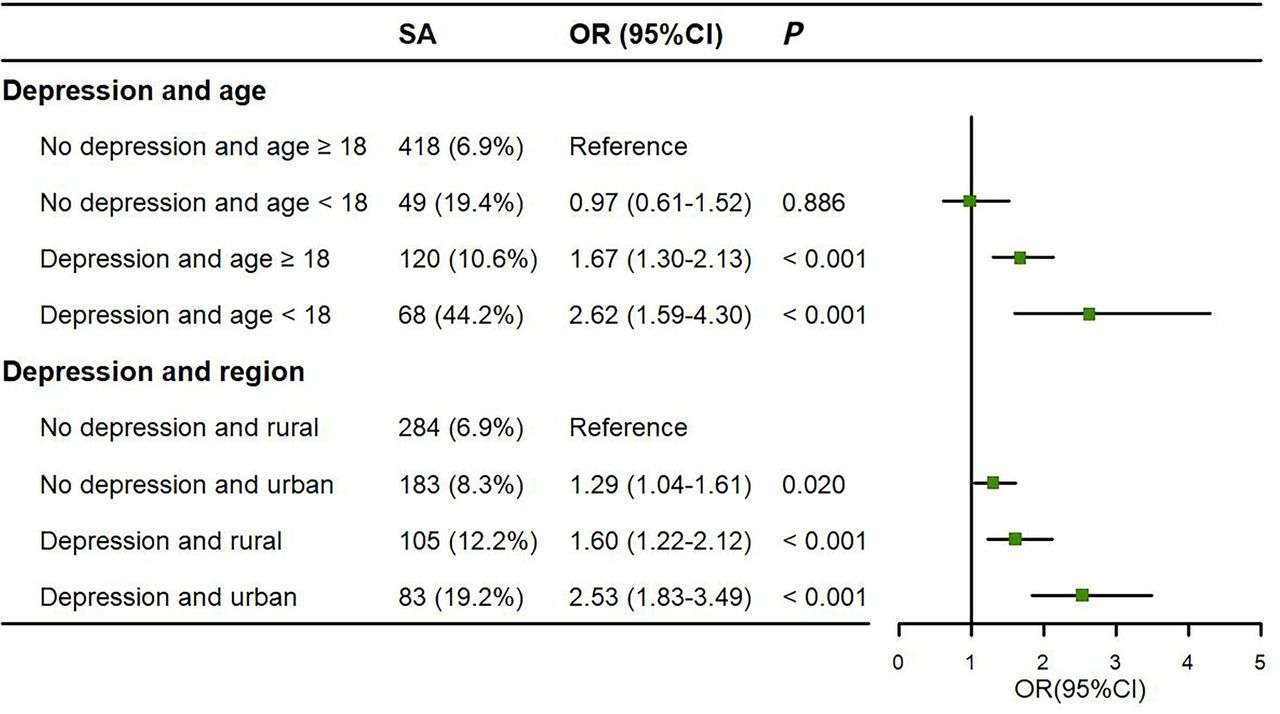
Furthermore, we found that depression was positively associated with SA by age and region. Specifically, compared with non-depressed adults, depressed juveniles and adults had the higher risks of SA, and ORs (95% CIs) were 2.62 (1.59 to 4.30) and 1.67 (1.30 to 2.13), respectively (figure 2). Furthermore, compared with rural individuals without depression, rural individuals with depression, urban individuals without depression and urban individuals with depression had the higher risks of SA, and ORs (95% CIs) were 1.60 (1.22 to 2.12), 1.29 (1.04 to 1.61) and 2.53 (1.83 to 3.49), respectively. Bootstrap analyses were used to verify the robustness of the association between depression and SA (n=6834 for 90%, n=6074 for 80% and n=5315 for 70%, respectively). Interestingly, the results of bootstrap analyses were consistent with the findings of the total population (online supplemental figures 2 and 3).

Association between depression and SA varied in age and region (n=7593). Note: confounding factors such as sex, occupation and chronic diseases were adjusted. SA, suicidal attempt.
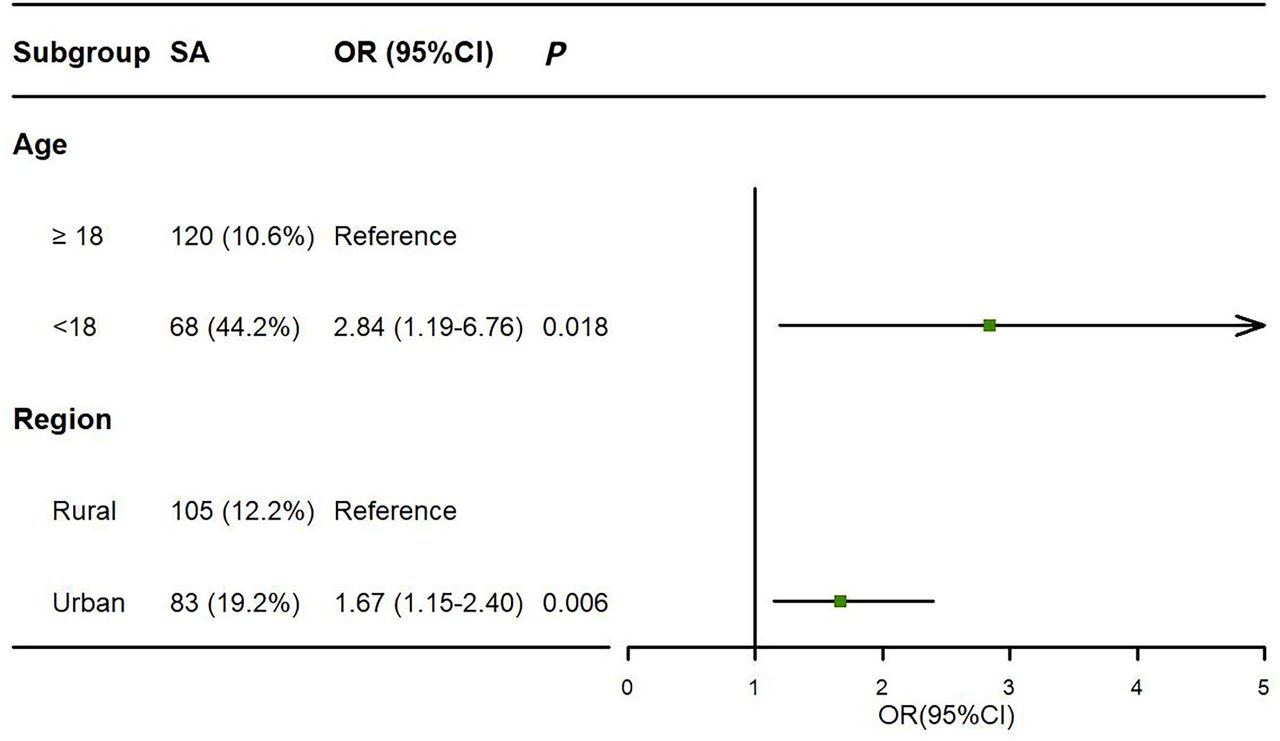
In a subgroup analysis, we further discovered that depressed juveniles were more likely to attempt suicide compared with depressed adults (OR 2.84, 95% CI 1.19 to 6.76, p=0.018), and urban patients with depression had the higher risk of SA compared with rural patients with depression (OR 1.67, 95% CI 1.15 to 2.40, p=0.006) (figure 3). Moreover, there was an interaction between region and age on SA (p=0.002) (online supplemental figure 5).

Association of age and region with SA in depressed patients (n=1290). Note: confounding factors such as sex, occupation and chronic diseases were adjusted. SA, suicidal attempt.
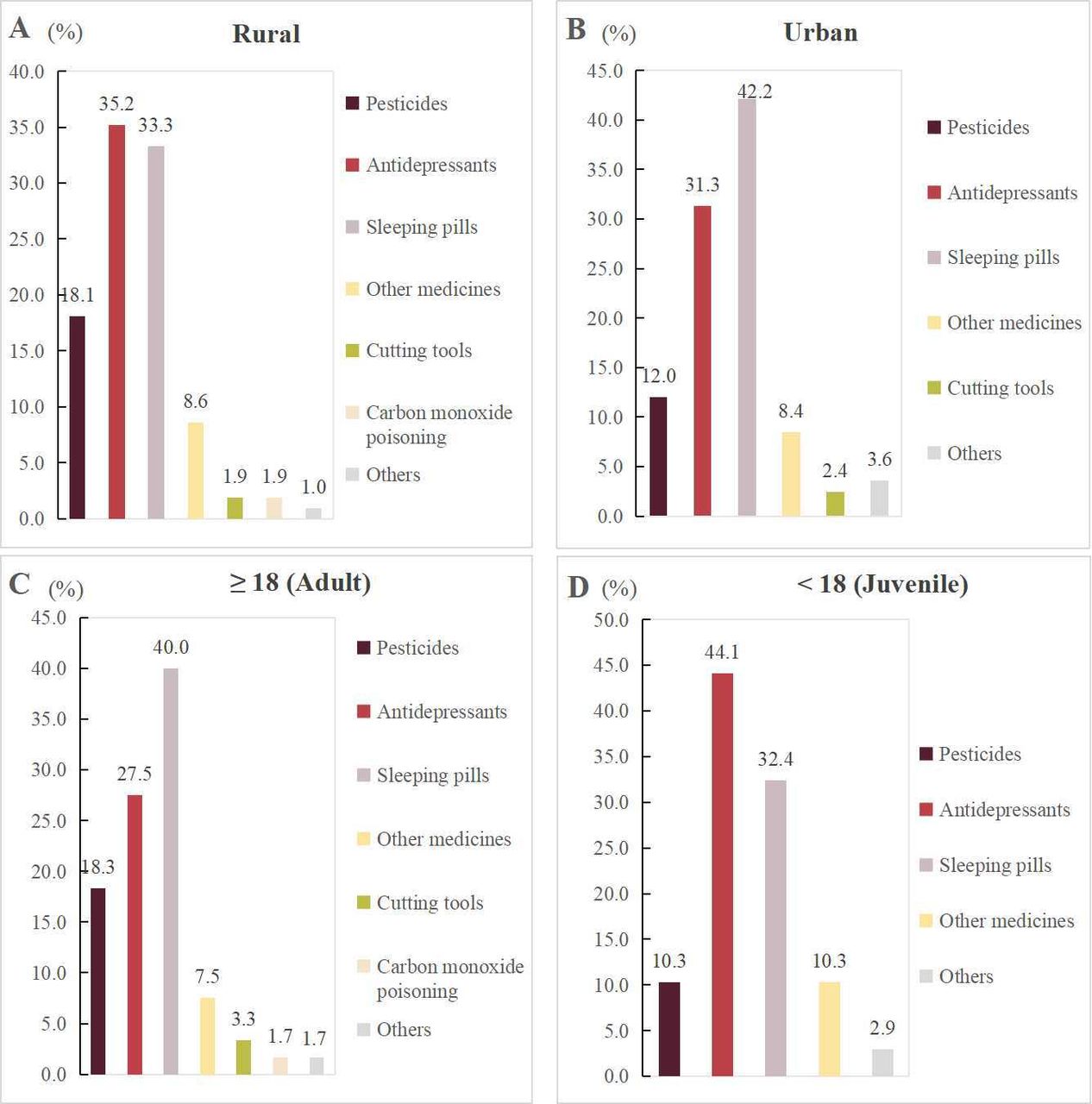
Notably, a total of 188 patients with SA were identified as having a history of depression. Among the depressive patients residing in rural region, the most prevalent method of SA involved the utilisation of antidepressants (35.2%), whereas urban patients frequently resorted to sleeping pills (42.2%). Regarding age groups, antidepressant usage (44.1%) was the predominant method of SA among juveniles, while sleeping pill consumption (40.0%) was more prevalent among adults (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Age and region differences in suicide methods among depressed patients.
Discussion
This was a large-scale clinical study assessing the association between depression and SA by age and region. Our study revealed a significant association between depression and an increased risk of SA, particularly among juveniles and urban individuals. The predominant methods of suicide among individuals with depression were the utilisation of sleeping pills or antidepressants.
In this study, we found that depression was strongly associated with SA, which was consistent with previous studies.34–36 Depression, as a mental health condition characterised by persistent feelings of sadness, hopelessness and despair, poses a substantial risk for suicidal ideation and behaviour.37 38 A reasonable explanation is that the intense emotional distress experienced by individuals with depression can become overwhelming and unbearable, leading them to consider suicide as a means to escape their pain.39–41 In addition, depression often leads to withdrawal from social interactions and a diminished support network, leaving individuals feeling isolated and disconnected.42 The absence of a strong support system can exacerbate the feelings of despair and increase vulnerability to suicidal thoughts and attempts.
Furthermore, the current study demonstrated the higher risk of SA among juveniles compared with adults. Depression is a prominent contributing factor to suicidal behaviour, especially among children and adolescents worldwide, with an estimated prevalence of mild to severe depression at approximately 21.3%.43 Children under the age of 15 diagnosed with depression are more susceptible to experiencing suicidal ideation and engaging in self-harming actions24. Adolescents, with their heightened emotional sensitivity and ongoing physiological changes, are prone to psychological and behavioural issues. The underdeveloped prefrontal cortex, responsible for emotional regulation, further impedes their ability to cope with negative emotions.24 Academic pressure, particularly prevalent in Chinese youth, has also been identified as a significant contributing factor to juvenile suicide.24–44 Notably, the COVID-19 pandemic has likely influenced the observed suicide rates, as it has had a profound impact on the lives, employment and studies of individuals in this study.45 46
Notably, urban patients with depression had a higher SA risk compared with rural those with depression, which was inconsistent with previous studies.28 29 47 Rapid urbanisation has spurred the intensification of population mobility and increased pressures in work, housing and social integration, jointly exacerbating the mental health challenges faced by urban residents, all of which are key factors driving the higher suicide risk in urban areas compared with rural areas.48–50 Moreover, it is important to note that mental healthcare accessibility in rural areas is limited, leading to the underestimation of suicide prevalence in these regions.51 Stigmatisation surrounding mental illness and suicide is particularly pronounced in rural areas, resulting in the concealment of such issues as accidental deaths by relatives of affected individuals. We also discovered that there was an interaction between region and age on SA. This interaction disclosed the complexity and specificity of the risk of SA among different urban–rural environments and age groups. For instance, urban adolescents, being in an environment with more abundant and diverse information, have easier access to various social phenomena, cultural concepts and value systems.19 52 This extensive exposure enables them to understand the complexity and diversity of society more comprehensively, but it might also cause them to perceive social pressure and competition earlier compared with their rural counterparts, thus increasing the risk of SA.
Interestingly, our study found that sleeping pills and antidepressants were the most common suicide methods used by individuals with depression. This finding is noteworthy, particularly considering the reduction in pesticide suicides observed in China.31 Discrepancies in suicide methods across nations can be attributed to social, economic and cultural disparities, as well as the availability of means for suicide.53 54 Additionally, the prolonged use of medication among individuals with depression, stemming from policies extending prescription periods, may contribute to the preference for sleeping pills and antidepressants as suicide methods.55
This study found several points worthy of consideration. First, urban healthcare providers should prioritise early screening and intervention for depressed adolescents to mitigate SA risks. Second, mental health caregivers should closely monitor medication use, especially sleeping pills and antidepressants, to prevent misuse and overdose. Finally, there is a need to strengthen collaboration among medical, school, community and family sectors to provide comprehensive mental healthcare for urban adolescents.
In summary, our large-scale clinical study highlights the significant association between depression and SA, emphasising the heightened risk among urban areas and juveniles. Sleeping pills and antidepressants emerged as the most prevalent methods of suicide among individuals with depression. These findings provide valuable insights for comprehending and addressing the complex dynamics surrounding depression and suicidal behaviour.
Limitations
There were some limitations to this investigation. First, because the study was retrospective, it was unable to determine the causal association between SA and depression, as well as region and age. Second, the study did not investigate the impacts of education and parental information on SA. Third, the study only collected data from one general hospital, not from others. Fourth, this study was carried out in a single province and city in China. Because of disparities in economy, geographical location and customs of culture, it is unclear whether the findings may be generalised to other provinces and cities. In future work, we will extend the duration of the study, enrich the variables, expand the research area and conduct longitudinal multi-centre studies to comprehensively understand suicide attempts in different contexts and ensure the extensive applicability of research findings.
Conclusion
This study found that high risk for SA in depressed populations include juveniles and urban participants, and revealed that the primary ways of suicide among depressed individuals are the use of sleeping medications and antidepressants, highlighting the importance of strengthening drug control and surveillance. Overall, our findings provide valuable insights into the relationship between depression and SA, offering implications for targeted interventions, mental healthcare improvements and suicide prevention strategies to mitigate the burden of depression-related SA.
Data availability statement
The data underlying this article cannot be shared publicly due to the privacy of individuals who participated in the study. The data will be shared on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve sensitive personal information, and all data has been meticulously de-identified. The Science and Technology Department (ethical committee management department) of Yijishan Hospital of Wannan Medical College exempted this study from ethical review (kyc2023061) in accordance with the 2023 regulations set forth by the National Committee on Science, Technology and Ethics of China.
Acknowledgments
We would like to thank all those who participated and supported the project.
References
Footnotes
Contributors DG, YX and ZZ contributed to the study design. DG and YX were responsible for data collection, data analysis data interpretation and the production of the initial manuscript. DG and YX made critical revisions to the manuscript. All authors have read and approved the final version of the manuscript. The guarantor of this article is DG.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.