Article Text

Abstract
Objectives To evaluate the effect of delivery hospital busyness on the postnatal condition and the perinatal mortality among small preterm infants born at ≤32+0 gestational weeks.
Design The daily delivery volume distribution is defined as lowest 10% (‘quiet’) and highest 10% (‘busy’) delivery-volume days, and days between (80%) as optimal delivery-volume days. We analysed differences in the incidence of selected adverse outcomes between quiet and busy days compared with optimal delivery-volume days by logistic regression followed by crude (ORs) and adjusted ORs (aORs) with 99% CIs.
Setting A population-based cohort study based on prospectively collected real-world data from five university hospitals and 21 non-tertiary-level delivery hospitals in Finland, 2006‒2016.
Participants 4323 small preterm infants.
Primary outcome measures Umbilical cord pH ≤7.05, Apgar score 0–3 points at the age of 1 min, Apgar score 0–3 points at age 5 min, birth asphyxia (International Classification of Diseases-10 code), resuscitation with intubation.
Secondary outcome measures Perinatal mortality comprising stillbirths and early neonatal deaths (<7 days).
Results Busy days (busy vs optimal) showed no correlation with the primary birth-related outcomes. However, in the university hospitals, quiet days were associated with 80% lower odds of asphyxia (aOR 0.20, 99% CI 0.08 to 0.48) and 47% lower odds of resuscitation (aOR 0.53, 99% CI 0.39 to 0.72) compared with their incidence on optimal days.
In university hospitals, the odds of early neonatal mortality among small preterm infants on busy days were twofold (aOR 2.08, 99% CI 1.26 to 3.45) than on optimal days. In the non-tertiary hospitals, however, this difference was statistically non-significant (aOR 0.68, 99% CI 0.19 to 2.45).
Conclusions In the tertiary university delivery hospitals, busyness was associated with a twofold increase in early neonatal mortality among small preterm infants, whereas infants’ condition at birth on busy days was comparable to their condition on optimal days. Neonatal capacity in tertiary units during busy days may be critical under stress.
- OBSTETRICS
- Quality in health care
- PERINATOLOGY
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The methodology of this study setting was validated in previous studies on term pregnancies.
Medical Birth Register data were completed with Population Register data from the Finnish Digital and Population Data Service Agency (live births), and cause-of-death data from Statistics Finland (stillbirths and small preterm deaths).
The number of daily deliveries served as the best proxy for the busyness but did not take into account the casemix differences and upward transfers from secondary to tertiary-level university hospitals.
Exposure, defined here as ‘busyness’, was estimated on a daily basis and may have varied over the length of a day.
Introduction
Preterm birth is one of the leading causes of severe perinatal morbidity and mortality worldwide.1 The WHO has categorised preterm birth as extremely preterm (<28+0 weeks), very preterm (28+0–31+6 weeks) and moderate or late preterm (32+0–36+6 weeks).2 The highest risk of antepartum death, stillbirth and early neonatal death occurs, among very or extremely preterm infants, in whose their earlier gestational age and low birth weight causes increased severe morbidity or mortality.3 Antepartum mortality may be associated with maternal pregnancy complications or infection leading to fetal asphyxia and/or infection, placental dysfunction or fetal abnormalities or severe haemorrhage.4 5
Preterm deliveries begin spontaneously with contractions, with the rupture of amniotic membranes or due to some medical indication. Labour induction or caesarean section may be necessary, based on the condition of either fetus or mother.6 Delivery hospital practices play a major role in preventing early neonatal mortality.7 Small preterm infants make up one of the most vulnerable patient groups with their need for special high-level care8; quality-improvement targets are essential to reduce child mortality.6 9 Obstetric care has clear implications for perinatal outcome, but quality indicators may vary, with consensus as to the best possible indicators being rare.10
In addition to quality indicators, the delivery hospital’s busy days, once categorised, can provide novel indicators of obstetric care quality. Therefore, defined busyness indicate as a quality indicator of weaknesses in processes leading to worsening outcomes of term infants.11 Busyness in obstetrics, resulting from suddenly increasing daily patient flow, is in part unavoidable; labour moves into its active stage on its own individual schedule. However, busyness in delivery hospitals may also challenge neonatal service capacity12 altering the processes13 or outcomes of obstetric and neonatal care.14 Still, the association of busyness in delivery hospitals with premature births is the unstudied topic.
Our aim was to study the effect of delivery hospitals’ daily delivery volume, defined as quiet, optimal or busy days, on the quality of obstetric care defined as selected adverse outcomes of small preterm infants with gestational weeks ≤32. Optimal busyness in delivery hospitals is difficult to assess and might well differ from unit to unit. In this study, the daily average was initially used as the optimal number of births. On quiet days (approx. 10% of days), the number of births was below the daily average, and on busy days (approx. 10% of days), at least twice the average. Hospitals were classified into categories based on their annual number of births and hospital profile. Therefore, lowest 10% and highest 10% allowed us to analyse hospital system’s capacity to keep the quality of care stable also during the busiest days, compared with optimal.12 13
Method
Finland is a Nordic country with 5.5 million inhabitants. In 2024, the annual delivery volume was approx. 43,700. Almost all women (99.4%) give birth in publicly funded delivery hospitals; private delivery hospital services are not available.15 The profile of the Finnish delivery hospital varies based on location and expertise level from the tertiary-level university hospitals to small local delivery hospitals with <1000 annual deliveries. Based on the legislation of the Health Care Act,16 deliveries at ≤32+0 weeks gestational age—ones equalling beforehand estimated low birth weight (<1500 g)— are centralised in five university-level hospitals to achieve the best possible care. Due to long distances and unpredictable course of pregnancy, this is not always possible. Non-tertiary hospitals also need to be able to deal with premature infants and have 24/7 readiness for emergency cases, including a neonatal surveillance unit with required equipment. A referral system is available between all delivery hospital levels with a well-functioning patient transfer system.17 18
This is a population-based cohort study, based on data from the Finnish Medical Birth Register (MBR), a mandatory national database including information on all live and stillbirths (from 22 gestational weeks or birth weight of 500 g). Data include information on maternal characteristics, care during pregnancy and birth, and each newborn’s characteristics and outcomes. MBR data are owned and maintained by the Finnish Institute of Health and Welfare. MBR data have been collected since 1987 and are highly respected for their coverage and reliability.19 20 Study data were collected from 2006 to 2016 and include information on 634 810 hospital deliveries. For this study, only singleton small preterm infant deliveries were included at ≤32+0 weeks of gestational age, meaning exclusion of multiple pregnancies (n=9149, of which 806 were born at ≤32+0 weeks).
During the study period, the Finnish delivery hospital network consisted of 34 delivery hospitals, 8 of which had an annual delivery volume of fewer than 1000. Due to this low delivery volume, these hospitals were closed during the study period. The 24 414 deliveries occurring in these small hospitals comprised 25 premature singleton births. After this exclusion, the total for preterm infants born at ≤32+0 gestational weeks in the remaining 26 delivery hospitals was 4323.
Unfortunately, our data did not include the information on patient transfers. The policy is to transfer most of the very low birthweight infants postnatally to university hospitals, but we are unable to analyse this in the current study.
Quality of care was assessed based on five selected adverse outcomes: umbilical cord arterial pH≤7.05 at the moment of birth (missing values 391, 9.0%), Apgar score 0–3 points at 1 min (missing values 306, 7.1%), Apgar score 0‒3 points at 5 min (missing values 550, 12.7%), birth asphyxia (all asphyxia diagnoses based on cardiotocography, diagnoses or microsampled blood during labour and/or the International Classification of Diseases (ICD)-10 codes O68, P20 or P21 arterial and/or vein or umbilical artery blood pH<7.05), and all resuscitation performed when intubation was necessary. Perinatal deaths were explored separately for stillbirths (including deaths before or during delivery) and early neonatal mortality (0‒6 days).
To study the effect of daily delivery volume as an exposure of the present study, daily delivery volume was defined separately for each calendar day for each included (n=26) delivery hospital. A day was defined from midnight (00.00 am) to midnight (24.00 pm). As previously described,11 12 14 quiet days were determined by defining around 10% of days, when the daily delivery volume was lowest at delivery-hospital level. To define busy days by the same methods, daily delivery volume was defined as approximately 10% of the days when the daily delivery volume was highest at delivery-hospital level. Days in between were defined as optimal days (around 80%), to reflect the period when daily delivery volume at delivery-hospital level was optimal for that hospital’s capacity. This approach was supported by our earlier publication.12 Delivery hospitals numbered five university hospitals and 21 non-tertiary-level delivery hospitals. The adverse outcomes of small preterm infants occurring on quiet and busy days were compared with adverse outcomes of those born on optimal days.
The prevalence of newborn and maternal demographics, as well as obstetric characteristics, is reported by daily delivery volume (quiet, optimal and busy days) and hospital categories (university hospitals and non-tertiary hospitals). Logistic regression with crude (ORs) and adjusted ORs (aOR) with 99% CIs to consider casemix, allowed study of the association between small preterm infants’ adverse outcomes and daily delivery volume defined as quiet, optimal or busy. Optimal days served as the reference category, with comparisons made between quiet versus optimal and busy versus optimal days. Analyses covered the total population and were conducted separately for the two hospital categories.
Covariate selection was made based on previous literature and chosen as delivery mode (vaginal, vacuum-assisted, caesarean section and elective caesarean section), birth weight (≤500 g, 501–1500 g and ≥1501 g), gestational weeks (≤28+0, 28+1–32+0), pre-eclampsia and gestational diabetes (identified based on ICD-10 codes O24.4 and O24.9).
All analyses were conducted using the Statistical Package for Social Sciences V.29.
Patient and public involvement
Neither patients nor the public were directly involved with this study in any way. Study participants were not contacted at any stage of this population-based cohort study. All of the data used were pseudonymised.
Results
Quiet, optimal and busy days in delivery hospitals
In university hospitals, 494 (13.8%) deliveries occurred on quiet, 2732 (76.4%) on optimal and 424 (9.8%) on busy days. In non-tertiary hospitals, deliveries numbered a respective 76 (10.2%), 597 (79.9%) and 74 (9.9%) (table 1). The occurrence of these characteristics did not statistically vary between quiet, optimal and busy days in the whole cohort, in university hospitals, or in other non-tertiary hospitals.
Background characteristics of 4323 small preterm infants with gestational weeks of ≤32+0 by delivery hospital categorisation on quiet, optimal and busy days
When comparing the differences in incidences of adverse outcomes by daily delivery volume in both hospital categories, university hospitals and non-tertiary hospitals, differences were detectable. In university hospitals, incidence of asphyxia was positively associated with daily delivery volume, although non-significantly. Incidences of asphyxia were 1.8%, 8.1% and 9.1% during quiet, optimal and busy days. Based on these figures, it seems obvious that busyness in university hospitals was associated with increased cases of asphyxia in preterm infants. In non-tertiary hospitals, the effect was the reverse, with lower incidence of asphyxia associated with busyness: 5.3%, 3.4% and 1.4%, during quiet, optimal and busy days. An association was also noticeable in university hospitals for resuscitation of preterm newborns: 21.9%, 32.8% and 32.0% during quiet, optimal and busy days. In contrast, in non-tertiary delivery hospitals, the proportions of resuscitation were lower on busy days, 18.4%, 12.9% and 10.8%, during quiet, optimal and busy days (table 2).
Selected outcomes in different level delivery hospitals and in total during quiet, optimal and busy days
In the university hospitals, the odds of early neonatal mortality were twofold (aOR 2.08, 99% CI 1.26 to 3.45) on busy when compared with optimal days. In addition, in the university hospitals, quiet days compared with optimal days were associated with 80% (aOR 0.20, 99% CI 0.08 to 0.48) and 47% (aOR 0.53, 99% CI 0.39 to 0.72) decreased odds of asphyxia and resuscitation, respectively. For non-tertiary hospitals, comparable results were non-significant (table 2, figure 1).

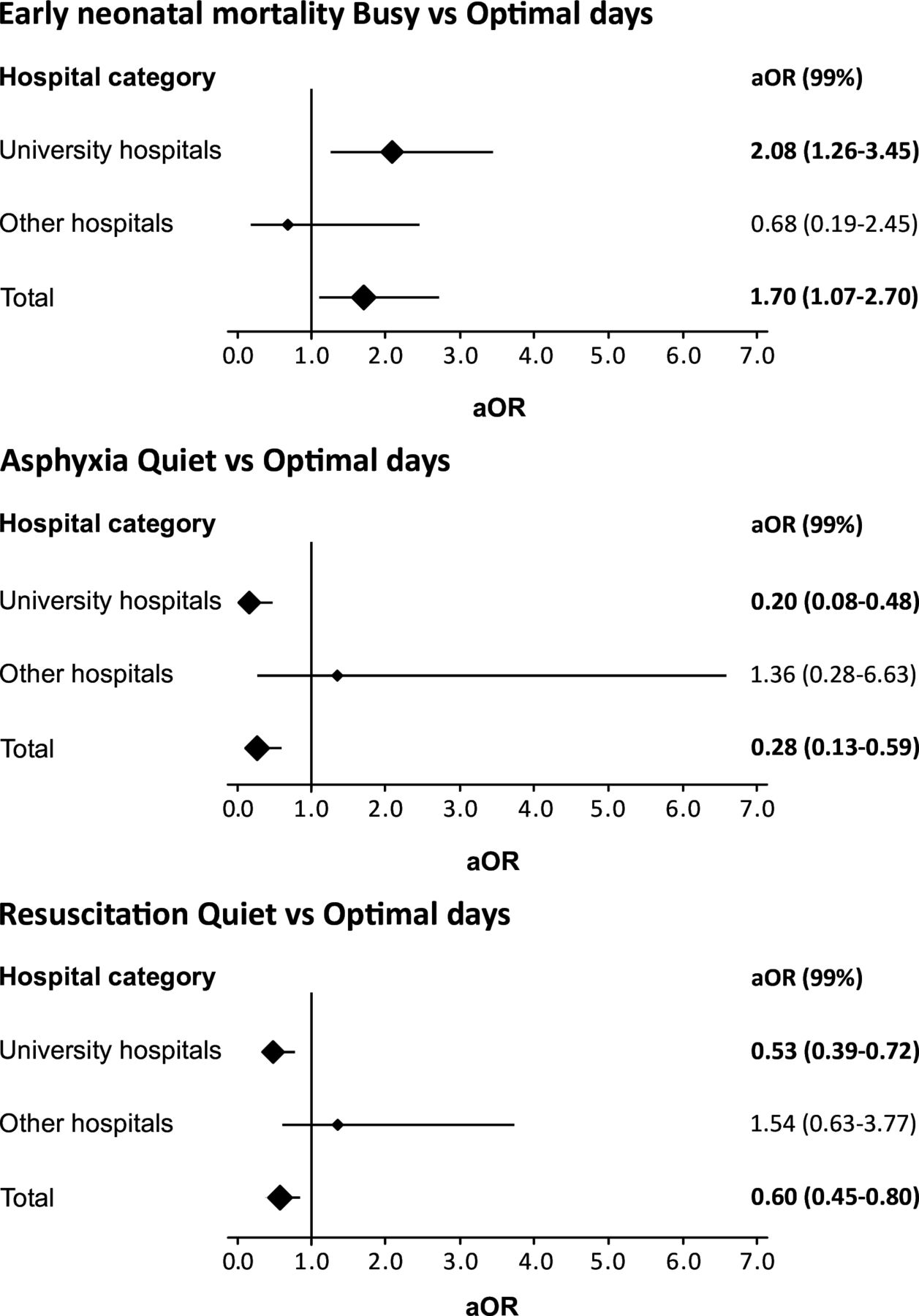{kind=link}
Forest plots of early neonatal mortality, asphyxia and resuscitation. aOR, adjusted OR.
Discussion
Birth on a busy day in the Finnish university hospitals was associated with a significantly higher perinatal mortality in small preterm infants than occurred on optimal or quiet days. The increased risk was doubled and related not to varying stillbirth rate, but to increased early neonatal mortality. Interestingly, the early postnatal condition of small preterm infants did not differ by daily variation in delivery hospitals busyness, suggesting that the outcome difference was related to differences in neonatal care rather than in differences in obstetric care. Quiet days in the university hospitals resulted less frequently than did optimal days in newborn asphyxia and resuscitation, with a decrease in perinatal mortality remaining non-significant. In the non-tertiary hospitals, differences in small preterm outcomes between quiet, optimal and busy days were non-significant, but interestingly, these trends were the opposite from those in university hospitals.
The present observational study showed a significant association between busyness and early neonatal mortality for small preterm infants in tertiary-level university hospitals but not in non-tertiary hospitals. These findings emerged, however, only from real-world data, because no deliveries and newborns can be exposed to busyness in randomised studies. On the busy days in the university hospitals, the condition of small preterm infants at birth was equal to their condition on optimal days, but still, the number of early neonatal deaths doubled. This suggests that busyness in a tertiary university hospital challenges neonatal services, a situation probably leading to the full capacity also being in use in the neonatal unit. That quiet days were protective against these adverse outcomes in university hospitals strengthens this conclusion. In the non-tertiary hospitals, busyness was unrelated to adverse outcomes, suggesting that overall neonatal capacity is on par with obstetric services. The patient casemix in non-tertiary hospitals is likely to put less stress on neonatal services compared with university hospitals. Interestingly, on quiet days in non-tertiary hospitals, the trend was towards worsening outcomes. This may reflect the ambition to treat complicated cases, when there were more available resources at the non-tertiary hospitals.
This study focused on the concept of busy day effect on obstetric outcomes.11 12 14 The novelty of this study was its adaptation of the same methods as in earlier studies. Busyness in delivery hospitals was used as a quality indicator of delivery hospitals’ ability to keep the quality of care constant, when delivery hospitals are under pressure with one of the most vulnerable patient groups, prematurely born infants at ≤32+0 weeks. Studies focusing on the consequences of busyness in the obstetric environment are limited in number. Some of them have suggested that busyness in a delivery ward during weekends (vs weekdays) was a risk factor for neonatal asphyxia,21 for increased odds of a <7 Apgar score, for neonatal seizures, or for admission to a neonatal intensive care unit.22
The strength of this study is that the study setting has been tested and validated by use of the same register data. The data were completed with Population Register data from the Finnish Digital and Population Data Service Agency (live births) and cause-of-death data from Statistics Finland (stillbirths and infant deaths). Furthermore, a large sample size increases the reliability of this study. Based on our earlier study results, the busyness of the delivery hospitals has been suggested as one of the quality indicators for obstetric care to evaluate delivery hospitals’ capacity to work under varying patient flow days.11 12 14 In the present study, the setting was well defined to small preterm infants and to their condition during and after birth, and the outcomes were widely recognised and used.
We defined quiet, optimal and busy days based on the daily delivery volume in different sized hospital categories and estimated to the nearest 10% to represent quiet and busy delivery volume days. However, due to the complexity, duration and nature of the delivery process, the calculations may not be exact, and the daily delivery volume does not describe the actual workload in the hospital during varying daily periods or by the various stages of the labour.
The weakness of this study is the definition of quiet, optimal and busy days. Busyness in a delivery hospital may vary hour by hour, so that 24 hours may be too wide a time window to estimate associations between busy days and neonatal outcomes. The day before the actual birth may sometimes be even busier than the actual birthday of the infant. Moreover, the data did not allow direct analysis of neonatal intensive care unit busyness. Furthermore, the data did not include birth weight z-score, which would have made regression model even better.
The data from multiple pregnancies are not included in this study, and this may be considered as a limitation. Unfortunately, the current work was a subanalysis of the original cohort, where the design excluded multiple births. However, multiple births are over-represented in preterm infants and would thus have been interesting.
Another limitation of this study was its definition of stillbirth, for which the timing of death remained in most cases unknown, leading to an assumption that the antepartum death may not have occurred on the same day on which the infant was born. It is possible to speculate that neonatal death may occur after possible patient transfer, and this may be seen as a limitation of this study. Patient transfers upward from non-tertiary to tertiary university hospitals may actually be related to busyness in the tertiary hospital, meaning that both patient volume and risk case concentration were biasing both the exposure and outcome. However, the MBR data do not include the information on patient transfers between varying level delivery hospitals, and for these reasons, patient transfers are not in the scope of this study.
Preterm infants with an expected birth weight less than 1500 g or gestational age less than 32 weeks are delivered in tertiary hospitals when possible. Long distances, emergencies and difficulties in predicting preterm labour may lead to delivery in non-tertiary hospitals. Thus, all delivery hospitals are required to have 24/7 readiness for emergencies, but smaller units have less experience with premature infants and before the centralisation of neonatal care in Finland preterm infants born in central hospitals had higher mortality than those born in university hospitals.23 The decision to deliver preterm baby in central or local level hospital needs to balance the risks of delivery with those of the transfer and depends on local experience and travel time to the nearest university hospital.
Conclusions
In small preterm infants, a significant association existed between birth on a busy day in the university hospital and higher perinatal mortality. This association was due to early neonatal mortality, not to increased rate of stillbirths. Since the infants’ condition at birth was not compromised, it was likely that differences were not explained by the differences in obstetric care. Instead, these results suggest that the capacity of neonatal care was suboptimal to tolerate the load. These findings call for further studies, to reveal whether neonatal resourcing in tertiary university hospitals on busy days should be improved.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
No ethics approval was required for this study. The THL Finnish Institute for Health and Welfare gave its permission to use its confidential register data.
Footnotes
X @shraisanen
Contributors The study group, consisting of RV, SH, SR, SA, MG and ML, collaboratively planned the study setting. RV, as the corresponding author, was responsible for the writing process, including the introduction, methods, results and discussion sections. All authors contributed their expertise and provided feedback on every section of the study. The study design and statistical analyses were planned and conducted by RV, ML and MG. ML is responsible for the overall content as the guarantor. The guarantor (ML) accepted full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This work was supported by the Foundation for Pediatric Research in Finland (Lastentautien tutkimussäätiö Funding number 220123).
Disclaimer Study or funder had no role in the study design: in the data collection, analysis, or interpretation of data; in the writing of the report or in the decision to submit the article for publication. In addition, the authors confirm the independence of the/all researchers from all funders and that all authors, external and internal, had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The lead author (the manuscript's guarantor: ML) affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned (and, if relevant, registered) have been explained.