Article Text

Abstract
Prophylactic respiratory support for patients after extubation is effective in improving their outcomes and prognosis. However, the optimal post-extubation respiratory support for different populations and disease types of mechanically ventilated patients remains controversial, and there is a lack of detailed, multidisciplinary, evidence-based recommendations for clinical application.
Methods and Analysis This protocol strictly follows the development process outlined in the WHO Handbook for Guideline Development and Guidelines 2.0, as well as the guidelines for the development of relevant methodological standards. Key steps in developing the guideline include: (1) establishing the guideline working groups, (2) defining the scope of guideline application, (3) selecting the priority clinical questions, (4) retrieving and screening evidence, (5) grading the quality of evidence, (6) forming recommendations and (7) conducting an external review.
Ethics and dissemination Ethical approval has been granted by Changzhi People’s Hospital (2023K023). Findings from this study will be disseminated through peer-reviewed publications.
Guideline registration PREPARE-2023CN418.
- Adult intensive & critical care
- Neonatal intensive & critical care
- Paediatric intensive & critical care
- Adult intensive & critical care
- Respiratory Therapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Adult intensive & critical care
- Neonatal intensive & critical care
- Paediatric intensive & critical care
- Adult intensive & critical care
- Respiratory Therapy
STRENGTHS AND LIMITATIONS OF THIS STUDY
The strength of this study lies in our working group’s diverse composition, which includes clinical and nursing experts with extensive critical care experience, alongside methodologists and policymakers, ensuring the guideline’s development is professional, scientific and feasible.
This is a post-extubation respiratory support guideline in development specifically for different populations and disease types of mechanically ventilated patients.
We are developing this guideline protocol and formal guideline document in strict accordance with the Guidelines 2.0 and the Reporting Items for Practice Guidelines in Healthcare.
The limitation of this study is that only literature in Chinese and English will be included.
Introduction
Diseases such as acute respiratory distress syndrome and sepsis are often triggered by infections, trauma and inhalation injuries, leading to activation of the pulmonary immune system.1 Neutrophils are rapidly recruited to the lungs, releasing a variety of inflammatory mediators, such as tumour necrosis factor alpha, interleukin (IL)−1 and IL-6, which further exacerbate alveolar injury. Lymphocytes play a crucial role in regulating the appropriate inflammatory response, and a reduction in circulating lymphocytes may perpetuate a harmful inflammatory state.2 As the lungs fail to effectively provide oxygen to other parts of the body or remove carbon dioxide, these patients require mechanical ventilation support to assist with breathing. Approximately 30% of patients in the intensive care unit (ICU) rely on mechanical ventilation for respiratory support.3 4 However, routine and prolonged mechanical ventilation (PMV) significantly increases the incidence of complications associated with ICU-acquired weakness, atelectasis, pneumothorax, ventilator-associated pneumonia and other conditions, severely impairing physical functions, delaying recovery and increasing length of stay in hospital and treatment costs.5–7
Therefore, during the course of treatment, when the patient’s primary condition is under control and ventilation and oxygenation are corrected, the ventilator and the artificial airway (extubation) should be removed as soon as possible.8 However, some patients in the ICU (about 10–30%) present complex and critical conditions (high risk of extubation failure), experiencing respiratory distress, reduced oxygenation and inability to maintain spontaneous breathing after extubation, necessitating reintubation. Reintubation not only prolongs the duration of mechanical ventilation but also results in mortality rates as high as 25–50% in these patients.9 10
The benefits of providing post-extubation respiratory support to ICU patients are still under discussion.11 Several studies have found that providing post-extubation respiratory support to patients at high risk of extubation failure (eg, due to underlying comorbidities such as heart failure, severe obesity or chronic obstructive pulmonary disease)12 can effectively improve clinical symptoms, lung function, prognosis and reduce the rates of reintubation and mortality.13–15 However, some studies have found that prophylactic use of respiratory support after extubation in patients with brain injury does not reduce the rate of reintubation and length of hospitalisation.16 17
In recent years, respiratory support options include conventional oxygen therapy (COT), nasal continuous positive airway pressure (NCPAP), non-invasive positive pressure ventilation (NIPPV) and high-flow nasal cannula (HFNC), among other modalities.18 19 Given the wide range of respiratory support treatment options available, existing guidelines do not provide adequate guidance regarding appropriate treatments for different populations and disease types. Consider the following examples of various ill-defined post-extubation respiratory support treatment options. Regarding the choice of respiratory support, a guideline recommends using HFNC in high-risk and/or obese patients undergoing cardiac or thoracic surgery to prevent immediate respiratory failure.20 Similarly, the American College of Physicians guideline recommends the use of HFNC in hospitalised adults with acute hypoxemic respiratory failure after extubation.20 21 However, some studies have found that HFNC after extubation does not prevent reintubation.22 For example, HFNC may be less effective than NIPPV in preventing reintubation in patients receiving PMV for at least 2 weeks.23
In summary, the effectiveness and optimal post-extubation respiratory support in different populations (adult, paediatric and neonatal patients) and various disease types (such as respiratory failure, post-cardiac surgery, hypercapnia) remain controversial, and no clinical guideline currently provide guidance for the best post-extubation respiratory support for all types of mechanically ventilated patients.24 There is a lack of detailed, multidisciplinary and evidence-based support. Therefore, it is necessary to develop a high-quality, evidence-based guideline for post-extubation respiratory support in mechanically ventilated patients in the ICU. This development should be based on the methodology outlined in the WHO Handbook for Guideline Development (second edition, 2014).25
Methods and Analysis
Guiding principles of the guideline
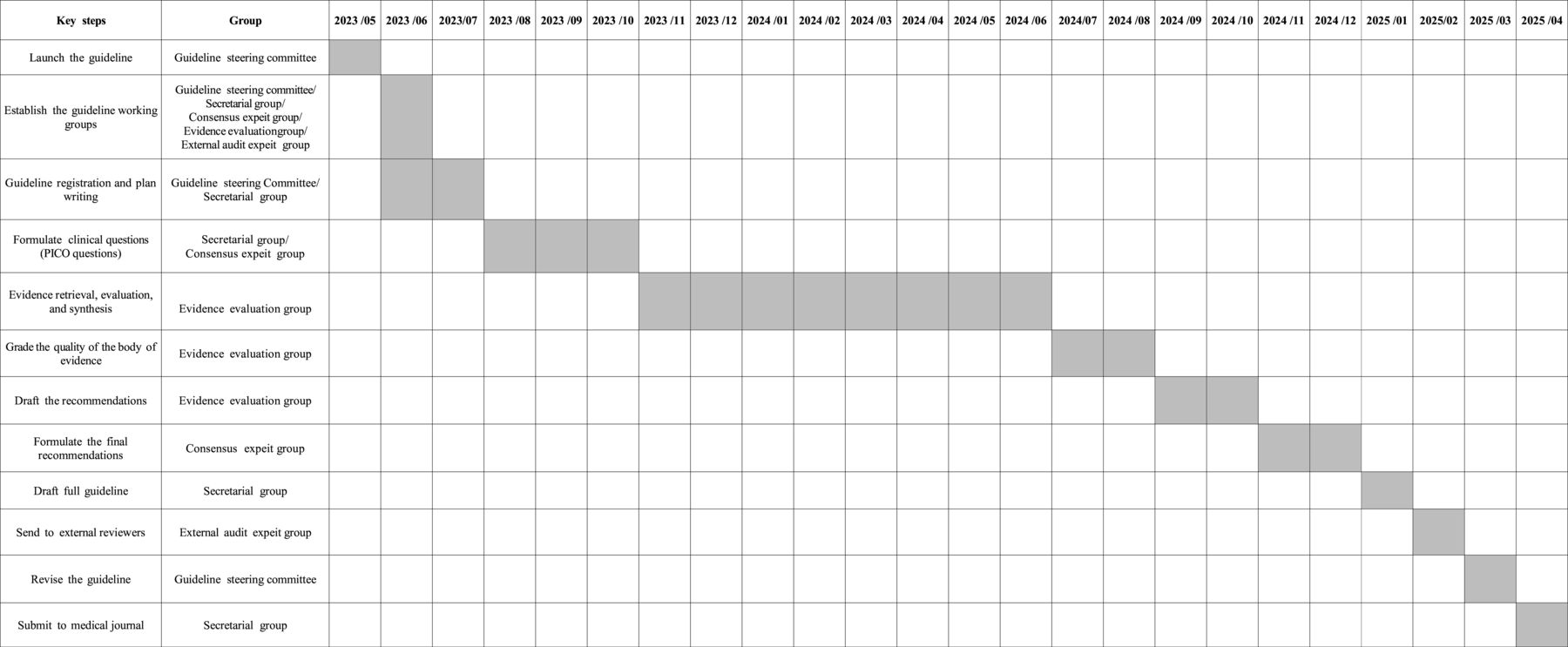
We will develop this guideline based on the concept of clinical practice guidelines from the US Institution of Medicine and the National Academy of Medicine.26 The guideline development process and methodological standards outlined in the WHO Handbook for Guideline Development are used,27 along with the Appraisal of Guidelines for Research and Evaluation II (AGREE II).28 The guideline is formulated in accordance with the Guidelines 2.0 and the Reporting Items for Practice Guidelines in Healthcare (RIGHT).29 A detailed overview of the working groups’ directives and their roles in this guideline is provided in online supplemental table 1. This guideline development study began in May 2023 and is scheduled to conclude in April 2025. The key steps and timeline of the guideline are shown in a Gantt chart (figure 1).
Supplemental material

Gantt chart. The key steps and timeline of guideline development. PICO, patient/population, intervention, comparison and outcomes.
Sponsors and supporting organizations of the guideline
This guideline is jointly sponsored by Changzhi Nursing Association and Changzhi People’s Hospital. The methodology and evidence are supported by the Evidence-Based Medicine Centre of Lanzhou University and the WHO Collaborating Centre for Guideline Implementation and Knowledge Translation.
Patient and public involvement
None.
Guideline registration
This guideline was registered on the International Practice Guide Registration Platform in both Chinese and English. The registration number is PREPARE-2023CN418.
Establishment of guideline working groups
The guideline development group consists of the guideline steering committee, the consensus expert group, the secretary group, the evidence evaluation group and the external audit expert group. They are responsible for identifying guideline topics, formulating clinical questions, conducting evidence searches, synthesising and evaluating evidence, developing recommendations, drafting this guideline and completing external reviews. Online supplemental table 2 provides a detailed overview of the composition and responsibilities of the guideline working groups. Furthermore, the study will be conducted in accordance with the Declaration of Helsinki (revised in 2013), ensuring that the dignity, rights, safety and health of participants are upheld throughout the research. To be selected for the guideline groups, members must be (1) experts in clinical medicine, nursing, guideline development, bioethics, health economics and other fields related to critical care medicine; (2) representative of different regions, with a balanced age and gender distribution and (3) providers for informed consent. All members of the guideline working groups are required to declare any conflicts of interest and these declarations will be published as an appendix to the final guideline document.
Scope of the guideline
The guideline focuses on the key issues related to post-extubation respiratory support treatment for ICU patients, including adult, paediatric and neonatal patients who are receiving mechanical ventilation. It is intended for healthcare professionals, including ICU clinicians, nurses, respiratory therapists and those in related fields such as paediatrics and critical care. The target population includes all patients undergoing mechanical ventilation extubation in the ICU.
Conflict of interest and funding
All members of the guideline steering committee, consensus expert panel, external audit expert group, secretariat and evidence evaluation group are required to complete a conflict-of-interest declaration form and manage any potential conflicts of interest. This guideline has not received any funding from pharmaceutical companies.
Identification of clinical questions and evaluation of their importance
Preliminary clinical questions related to post-extubation respiratory support for mechanically ventilated patients in the ICU are generated through the review of relevant guidelines both domestically and internationally, as well as by conducting questionnaires to clinicians, nurses and respiratory therapists. The secretariat will be responsible for organising the collected clinical questions, eliminating duplicates and consolidating remaining questions. The final clinical questions for the guideline will be determined through two rounds of the Delphi method, where a panel of experts rates and provides feedback on each question to reach consensus on their importance and scope. In the second-round meeting, team members will evaluate the importance of all issues on a scale of 1 to 5 (with five being the most important and one the least, indicating clinical insignificance). Specific clinical questions will be formulated according to the PICO elements: P (population), I (intervention), C (comparison) and O (outcome). Subsequently, the top 10 to 20 clinical questions will be selected according to the highest scores. After approval by the expert committee, the clinical questions to be addressed in this guideline will be finalised.
Evidence retrieval, screening and data extraction
Eligible studies will be identified through searches in databases including Pubmed, Medline, Embase, the Cochrane Library, Epistemonikos, UpToDate, BMJ Best Practice, Clinical Key, DynaMed Plus, the China Biology Medicine disc, ClinicalTrials.gov, the International Clinical Trial Registry Platform and other Chinese and English databases. Searches will also be supplemented by clinical trial registries and by tracing the references of included articles. Both Medical Subject Headings terms and free words will be used to form the search strategy, limited to publications from the inception of the databases until January 2024. Searches will be conducted in English or Chinese. The search terms include “Airway Extubation*”,“Tracheal Extubation*”,“Intratracheal Extubation*”,“Endotracheal Extubation*”,“post-extubation”,“high flow nasal cannula”,“high flow nasal oxygen”,“HFNC”,“HHFNC”,“HHFN”,“NHF*”,“high flow”,“Cannula”,“Nasal Cannula*”,“oxygen inhalation therap*”,“Positive Pressure Respiration”,“Non-Invasive Ventilation*”,“Noninvasive Ventilation*”,“non-invasive positive pressure ventilation*”,“noninvasive positive pressure ventilation*”,“NIPPV”,“NPPV”,“conventional oxygen therapy”,“COT”,“standard oxygen therapy”,“SOT”,“venturi mask”,“face mask”,“bag valve mask”, “entrainment mask”. The search strategy for the PubMed database is presented in the Supplementary file.
Literature inclusion criteria: (1) the subjects of the study were patients of any age undergoing mechanical ventilation and extubation; (2) the types of studies included China and international guidelines, systematic reviews or meta-analyses, randomised controlled trials (RCTs), diagnostic tests, cohort studies, case-control studies, case series and case reports. Exclusion criteria: we excluded articles that were not written in Chinese or English. However, journal articles with formal translations in Chinese or English will not be excluded. Additionally, we excluded articles with incomplete or missing research data, articles for which we were unable to obtain original data, and duplicate articles.
If the literature from secondary research (defined as analyses or systematic assessments based on existing primary data or published research findings, such as systematic reviews and meta-analyses) fails to address the clinical questions required for the guideline, lacks relevant secondary evidence or needs updating (publications older than 2 years and the original studies published within 2 years), a systematical search will be conducted for RCT, non-randomised controlled studies, case reports and other relevant studies.
The guideline development team will work in pairs to independently search and screen the literature by title, abstract and full text. They will extract data from the literature and record the number of articles initially retrieved and those finally included. Any disagreements will be resolved by discussion or consultation with a third-party expert in evidence-based methodology.
Evaluation of the quality of literature
We will use the AGREE II,30 A MeaSurement Tool to Assess systematic Reviews,31 the Cochrane Collaboration’s tool for assessing the risk of bias in randomised trials32 and the Newcastle-Ottawa Scale33 to evaluate the methodological quality of the included literature. Online supplemental table 3 provides a detailed description of the assessment tools used for various study types in the assessment process. The assessment will be conducted independently by two researchers using the research instrument. If there is a disagreement between their findings, it will be resolved through discussion or negotiation with a third-party expert to reach a final consensus.
Grading the quality of evidence
Evidence quality grading was conducted for the pooled evidence corresponding to each guideline question’s outcome indicator. The guideline questions included in the original research evidence were assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system. This assessment considered five downgrading factors: limitations (risk of bias), imprecision, inconsistency, indirectness and publication bias, as well as three escalating factors: large effect, dose-response and the presence of all plausible residual confounding. The quality of evidence will be classified as follows: high (a): very certain that the observed value is close to the true effect; moderate (b): moderately certain that the observed value is probably close to the true effect, but there is a possibility of substantial differences; low (c): limited observational values which may be substantially different from the true effect and very low (d), observational values are likely to be substantially different from the true effect. The evidence quality was graded according to these evaluations, and a summary table of the evidence was compiled.
Forming recommendations and reaching a consensus
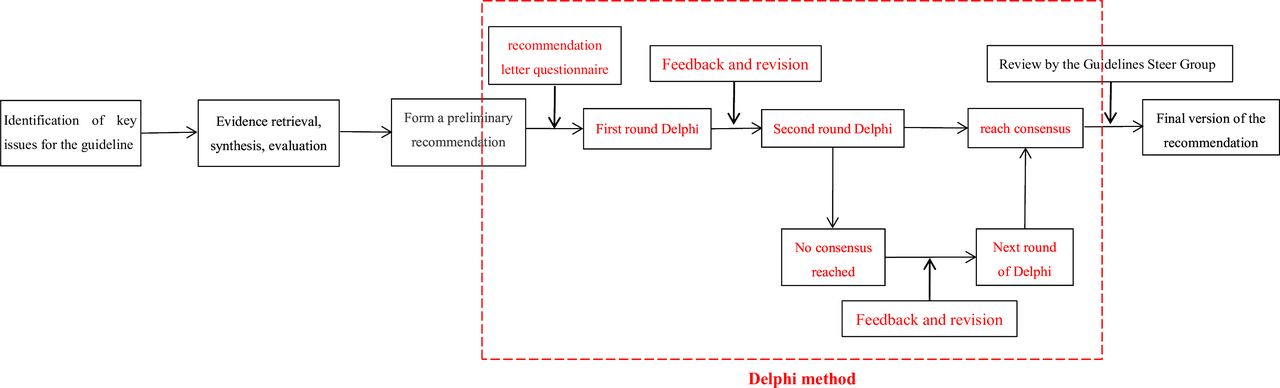
Recommendations supported by evidence will be categorised into four levels according to the GRADE system: strong, weak, strong against and weak against (table 1). The consensus expert group assessed factors such as the quality of evidence, values, economic analysis, balance of advantages and disadvantages to form a preliminary recommendation. All the recommendations were compiled into a recommendation letter questionnaire, which was distributed to the consensus group experts for evaluation and suggested modifications. The consensus expert group reached a consensus on the recommendation after conducting 2–3 rounds of Delphi method. A flowchart depicting each stage of the Delphi process is shown in figure 2.

{kind=link}
{kind=link}
The flowchart showing each stage of the Delphi process.
GRADE strength level of recommendation
The rules for reaching a consensus are as follows: if over 50% of the experts chose ‘2’, and over 70% chose ‘2’ or ‘1’, the recommendation achieved consensus with a ‘strong’ recommendation strength. If more than 50% of the experts chose ‘2’ or ‘1’, and fewer than 20% chose ‘−2’ or ‘−1’, the recommendation also reached consensus but with a ‘weak’ recommendation strength. Other scenarios were considered as lacking consensus, and the recommendation moved forward to the next round of voting. For guideline issues where no consensus was reached but a recommendation was needed, the guideline steering committee further discussed and determined the final recommendation based on the voting analysis. When all issues reached either a consensus or a non-consensus threshold, and no new significant opinions emerged, the Delphi process was deemed complete.
Guideline drafting and external review of recommendations
The RIGHT checklist, which consists of 22 items, can assist guideline developers in effectively reporting their guidelines.29 The secretariat will draft the initial version of the guideline according to the RIGHT entries and submit it to the external audit expert group for review and feedback. This group consists of clinical medicine, nursing, methodology and other multidisciplinary experts. They will evaluate the draft from the perspectives of acceptability, clarity of expression and clinical feasibility and provide suggestions for improvement. The secretariat and the evidence evaluation group will revise the draft based on feedback from external audit experts to create the final version of the guideline.
Guideline approval, release and update
The final draft of the guideline will be reviewed, finalised and approved by the expert committee. With the agreement of 2/3 of the consensus group experts, the expert committee can modify and refine the important issues in the proposal. The secretariat is responsible for accurately documenting the entire modification process. We are in the development of a comprehensive programme for regular review and updates, which includes a systematic process for monitoring new evidence, reviewing guideline content and incorporating necessary changes. Guideline updates will be based on the following criteria: (1) the recommendations remain unchanged, but new evidence is available based on a larger sample size or higher quality than previously considered and (2) the recommendations have changed due to new high-quality evidence that does not support the existing recommendations, or there have been changes in the safety or target population of the existing recommendations.
We plan to formally review and update the guidelines every 2 to 3 years. This schedule allows us to incorporate important new evidence and ensures that our recommendations align with the latest clinical research and practice standards.
Guideline dissemination, implementation, and evaluation
After the guideline is released, the project team will promote and disseminate it primarily through the following methods: (1) presentations at relevant academic conferences; (2) organisation dedicated guideline promotion meetings in some provinces and cities in China to ensure that clinicians, respiratory therapists and nurses fully understand and correctly apply the guideline; (3) distribution of guideline interpretations through commonly used medical websites, applications and short video platforms in China; (4) organisation of guideline training sessions in different provinces for clinicians, pharmacists and nurses to familiarise them with the guideline; (5) members of the guideline steering committee and guideline development expert panel will write articles related to the guideline for publication in journals and (6) evaluation of the guideline’s impact on clinical decision-making. We aim to provide evidence-based recommendations to enhance clinicians’ decision-making process, reduce variability in treatment practices and ensure consistent application of best practices. 2 to 3 years after the publication and implementation of the full text of the guideline, we will evaluate the current status of post-extubation respiratory support modalities for mechanically ventilated patients in the ICU in China and abroad. This evaluation will help us understand the dissemination of the guideline, the recognition of its recommendations in clinical practice, and its impact on treatment decisions. Additionally, it will be beneficial for improving and refining the guidelines during its next update.
Ethics and dissemination
Ethical approval has been granted by Changzhi People’s Hospital (2023K023). Findings from this study will be disseminated through peer-reviewed publications.
Discussion
34 ,35Due to the physiological and pathophysiological differences among adults, children and neonates (such as preterm infants who are more susceptible to complications and even death post-extubation due to immature organ function, particularly respiratory function34) and the distinct characteristics of various diseases (for example, in patients with respiratory failure, severe impairment of pulmonary ventilation and/or gas exchange can lead to a series of pathophysiological changes and corresponding clinical syndromes),35 it is clear that providing the same type of respiratory support to all extubated patients is unreasonable. Instead, tailored respiratory support should be provided according to their individual needs to maintain normal respiratory function and improve their prognosis.
With advancements in medical technology, various methods of post-extubation respiratory support are available for mechanically ventilated patients. Non-invasive ventilation (NIV) helps maintain airway defences while aiding bronchial re-expansion and restoring respiratory mechanics, but it has a high complication rate.36 Two common modes of NIV are NCPAP and NIPPV. NCPAP enhances alveolar compliance, reduces airway resistance and improves pulmonary ventilation and gas exchange; however, its tolerance and adherence are relatively poor.37 NIPPV provides positive end-expiratory pressure and airway pressure, improving cardiopulmonary function and oxygenation indices, but it may increase the risk of ventilator-associated lung injury.38 NHFOV is an emerging mode of NIV that adds pressure oscillations to NCPAP, providing greater benefits in maintaining alveolar stability, improving oxygenation and promoting carbon dioxide elimination.39 HFNC is also a novel form of respiratory support that delivers patients with high-flow heated and humidified gases with stable inspired oxygen concentrations, significantly enhancing patient comfort and tolerance while demonstrating improved clinical outcomes.40 41 However, current guidelines only recommend the prophylactic use of post-extubation respiratory support without providing specific guidance for different populations and diseases,42 leaving users often unable to obtain useful information on respiratory support modes from these guidelines.
To recommend the best respiratory support methods for patients, we will establish a multidisciplinary team to develop a guideline for respiratory support after mechanical ventilation extubation. This process will strictly adhere to the WHO Guideline Development Handbook27 and the guideline development checklist.43 This protocol will serve as the foundation and framework for the guideline development process, ensuring standardisation in both procedures and methods. The guideline development working group will conduct a thorough review of the literature and surveys to fully understand the key clinical issues in post-extubation respiratory support. They will systematically search for, evaluate and grade existing best clinical evidence, integrating this with clinical expert experience and various other factors to develop high-quality guidelines. This guideline will aim to scientifically guide evidence-based clinical practice and ultimately improve patient outcomes.
Ethics statements
Patient consent for publication
References
Footnotes
XH, JC and JH contributed equally.
Contributors All listed authors meet authorship criteria and no others meeting the criteria have been omitted. XH conceived the idea for the project. All authors (JC, JH, MZ, YH and JT) contributed to the design of the study. XH wrote the first draft of the manuscript. JC, JH and JT contributed to the refinement of the study methods and critical revision of the manuscript. All authors read and approved the final version of the manuscript. The guarantor of the study is XH, accepts full responsibility for the finished work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.