Article Text

Abstract
Objective Unintentional injuries constitute a significant global public health issue with significant social and economic costs. Previous evidence suggests ambient temperatures are associated with unintentional injury occurrences. However, the impacts of ambient temperature on unintentional injury economic burden have received little research attention. The objective of the study was to examine the association between ambient temperature and economic burden of unintentional injury.
Design Time-stratified case-crossover study.
Setting This study was performed at Tianjin Hospital, the largest trauma centre in Tianjin, by applying a hospital-based time-stratified case-crossover study.
Participants The 12 241 patients admitted with unintentional injuries and meteorological data were collected in Tianjin, China in 2021.
Primary and secondary outcome The association between ambient temperature and unintentional injury hospitalisation was evaluated with a distributed lag non-linear model, further temperature-attributable economic burden of unintentional injuries was quantified, and adjusted for demographic characteristics, injury mechanism and injury location of injury.
Results The temperatures below 11.5°C were significantly associated with the increased risk of unintentional injury hospitalisation in Tianjin, in 2021. The effect was maximised on the current day. The relatively low temperature was responsible for 25.44% (95% CI 13.74, 33.09) of unintentional injury patients, and was associated with the number of unintentional injury patients (3114, 95% CI 1608, 4036). The relatively low temperature was associated with the excess economic burden for unintentional injury (¥197.52 million, 95% CI 102.00, 256.00; about 27.10 million dollars), accounting for 26.49% of the total economic burden. The cold temperatures generally had greater impacts on males (¥136.46 million, 95% CI 83.28, 172.42; about 18.67 million dollars) and the elderly (¥74.35 million, 95% CI 14.87, 102.14; about 10.24 million dollars).
Conclusion The temperature was associated with approximately 3000 unintentional injury patients and ¥200 million (27 million dollars), accounting for 26% of the total economic burden in Tianjin, 2021.
- PUBLIC HEALTH
- PREVENTIVE MEDICINE
- Trauma management
Data availability statement
Data may be obtained from a third party and are not publicly available. The datasets generated during and analysed in the current study are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A distributed lag non-linear model was used to investigate the association between temperature and unintentional injury hospitalisation.
The economic burden of temperature-attributable due to unintentional injuries was quantified by calculating attribute numbers.
The modification effects of different demographic and injury characteristics were explored using subgroup analysis.
Being a single-city study limited the generalisation of the findings.
Introduction
Unintentional injuries as a major public health issue increase disability and death, and also represent great economic costs.1 2 As defined by the WHO, unintentional injuries occur in the absence of predetermined intent. It has been estimated that more than 5 million people die each year due to injuries, and nearly 80% of injury deaths are due to unintentional injuries.3 Most unintentional injury cost estimates have been conducted in high-income countries. A study from the USA estimated unintentional injuries in the home to cost US$217 billion annually.4 Cost estimates for fall-related hospitalisations vary across regions of the world and within countries,4 according to Sartini et al in Italy ($7945),5 Roudsari et al in the USA ($17 483)6 and Stevens et al in the USA ($7355).7
It is widely recognised that increasing episodes of extreme weather are the phenomena associated with climate change and are currently accelerating.8 Ambient temperature is of great interest as a major environmental health risk factor.9 10 Previous studies determined the association between temperature and injuries associated with traffic accidents,11 and the number of total injury admissions.12 Luo et al found that hot extremes were associated with increased unintentional injury mortality risk in China.13 Lee et al found that low temperature as well as high temperature significantly affected the risk of injury in Seoul, Korea.2 There have been separate efforts to determine the association between ambient temperature and injury incidence. Nevertheless, the relationships between ambient temperature and the economic burden of unintentional injury have not been comprehensively investigated.
The current study used data of patients admitted with unintentional injury and meteorological data to evaluate the association between ambient temperature and unintentional injury hospitalisation, applying a case-crossover design with a distributed lag non-linear model (DLNM), and further quantify temperature-attributable economic burden of unintentional injuries. The findings will draw a comprehensive picture of the health impacts of temperature on unintentional injury hospitalisation in Tianjin, China.
Materials and methods
Study area and data collection
Tianjin was a megacity located in northern China with a population of approximately 13.8 million inhabitants and covered 11 946.88 km2, which was administratively equivalent to a province (online supplemental figure S1). Tianjin (117.2°E, 39.1°N) experienced a warm temperate monsoon continental climate with four distinct seasons, including a hot and wet summer (due to monsoons), and a cold and relatively dry winter (due to vast Siberian anticyclones).14 Given that Tianjin had a large population and a relatively wide range of ambient temperatures, it was an appropriate location for evaluating the association between ambient temperature and unintentional injury hospitalisation with adequate statistical power.
Supplemental material
This study was performed at Tianjin Hospital, the largest trauma centre in Tianjin. It was a level 2 trauma centre, and its emergency department (ED) provided 124 009 consultations per year. A retrospective study of all patients admitted with unintentional injuries (International Classification of Diseases, 10th Revision (ICD-10) codes: V00-X59) to Tianjin trauma centre from ED was conducted based on the electronic medical record system from 1 January through 31 December 2021. Information on patients included the date of onset, age, gender, injury mechanism, injury location, hospital length of stay and hospitalisation cost. Furthermore, daily meteorological data for Tianjin in 2021 were obtained from the China Meteorological Data Sharing Service System (http://data.cma.cn/) issued by the National Meteorological Information Centre of the China Meteorological Administration.
Outcome of interest
In the present study, the outcome of interest was the daily number of patients admitted with unintentional injuries. Data were collapsed by date to create time series of the daily number of patients admitted with unintentional injuries, and were stratified by gender, age, injury mechanism and injury location. Three age groups were considered (ie, <18 years, 18–64 years and ≥65 years). The injury mechanism and injury location were coded using ICD-10. Unintentional injury was divided into road traffic injury (V00-V99), falls (W00-W19), mechanical injury from exposure to mechanical forces (W20-W64) and other injuries (W65-W99, X00-X59). Injury locations were divided into head and neck (S00-S19), thorax (S20-S29), abdomen (S30-39), upper extremity (S40-S69), hip and thigh (S70-79), lower extremity (S80-S99), multiple locations in the body (T00-T14) and unspecified (T08-T14, T20-T35, T66-T88, T90-98). The diagnosis was verified by the ED physician.
Exposure assessment
Daily meteorological data included daily mean temperature, max temperature, min temperature, barometric pressure, relative humidity, precipitation, average wind velocity, rain day and snow day at climate stations across Tianjin in 2021. We averaged the daily available weather conditions measurements of climate stations to represent the exposure in the target populations in Tianjin area. To control for the effect of potential confounding factors, the data for other meteorological variables were also obtained.
The holidays (except Saturday and Sunday), day of the week, calendar time and the number of confirmed cases of COVID-19 as the epidemic indicator were considered as short-term covariates. Weekends were defined as Saturday and Sunday, and weekdays were from Monday to Friday. Holidays were defined as weekends and the Chinese statutory holidays (29 days per year), including New Year, Spring Festival, Qing Ming Festival, Labour Day, Dragon Boat Festival, Mid-Autumn Festival and Chinese National Day, and non-holidays as the other days.
Statistical analysis
Continuous variables were expressed as the mean±SD or the median (IQR). Categorical variables were sorted by frequency (percentages). Spearman’s correlation coefficients were used to summarise the similarities in daily meteorological variables. When the correlation coefficient between two variables was greater than 0.8, it indicated that there was a colinear relationship between the two variables. There were high correlations among these three temperature measurements (Spearman r=0.920 to 0.978). These temperature measurements were strongly correlated with barometric pressure (Spearman r=0.796 to 0.850) (online supplemental table S1). Since mean temperature was a better predictor of population health than barometric pressure, maximum or minimum temperatures, we selected the daily mean temperature as the exposure indicator of ambient temperature.15 Statistical analysis was performed using R software (V.4.2.1). All statistical tests were two-sided, and values of p<0.05 were considered statistically significant.
Assessing the association between ambient temperature and unintentional injury admission
A time-stratified, case-crossover design was applied to investigate the association between ambient temperature and unintentional injury. This case-crossover design is useful for controlling for time-invariant characteristics and for slowly varying factors, as each patient serves as his/her own control. In the present study, each ED visit day of patients admitted with unintentional injuries was matched to all control days within a stratum, defined as a three-way interaction term (year×month×day of the week). For instance, if a patient visited an ED with unintentional injuries on Thursday, 1 July 2021, all other Thursdays in July 2021 were selected as control days.
Daily mean temperature and the number of patients admitted with unintentional injuries were linked by date. A quasi-Poisson DLNM was employed to investigate their associations. DLNM is a modelling framework that simultaneously describes the non-linear expose-response relationship and delay effect. DLNM usually quantified the lag effect and non-linear effect of ambient temperature on injury risk.2 13 Because the daily number of patients admitted with unintentional injuries typically followed an over-dispersed Poisson distribution, a model of quasi-Poisson was applied. In order to flexibly account for the potential lagged and non-linear effect of mean temperature on the number of patients admitted with unintentional injuries, mean temperature was incorporated as a ‘cross-basis’ function using DLNM. We empirically decided on a maximum lag of up to 21 days according to previous large studies.16 17 A number of covariates were also incorporated as follows:

where t was the day of the observation; Yt was the count of patients admitted with unintentional injuries on day t; α represents the intercept of the model; cb(Tt) was a cross-basis of mean temperature; CWt was a binary variable for holidays (1 if day t was classified as part of a holiday, 0 otherwise); DOWt represented the day of the week which was modelled with six indicator variables through a dummy parameterisation; β and γ were the vectors of regression coefficients; s() was a smooth function; DOYt represented the day of the year specified through a natural cubic spline with 7 df per year to account for seasonality and long-term trends. W(i, t) meant covariates in meteorological variables without co-linear relationship on day t, including relative humidity, precipitation, average wind velocity, the number of COVID-19 confirmed cases, rain day and snow day, which was controlled by using natural cubic spline (ns) with 3 degrees of freedom (df) determined by the Akaike Information Criterion (quasi-likelihood for Akaike’s Information Criterion).
The relative risks (RRs) of extreme temperature (eg, 10th temperature percentile and 25th temperature percentile) were calculated compared with the referent temperature, that is, the temperature with the minimum counts of patients admitted with unintentional injuries. The lag effect refers to the fact that changes in unintentional injury hospitalisation are influenced not only by the current value of the ambient temperature, but also by its past values. Therefore, the lag structures in the effects of extreme temperature over lags of 0–21 days were also explored.2 18 19 Subgroup analyses were conducted to assess whether the associations between temperature and unintentional injuries differed by demographic characteristics (age and gender), mechanism of injury and location of injury.
R packages of ‘dlnm’ were used for the DLNM to explore the relationship between ambient temperature and unintentional injury hospitalisation, and ‘spline’ was used for the natural spline function to investigate the non-linear relationship between them.
Calculating economic burden of unintentional injuries due to ambient temperature
The attributable fraction (AF) and attribute numbers (AN), and their 95% CIs were calculated using the following formulas20 21:


where AFt referred to the attributable fraction of unintentional injury hospitalisation due to ambient temperature on t day; we considered that the risk at day t was the cumulative effect of the previous period (t−l0, …, t−L) of exposure; L was the maximum lag time for the exposure factor; δ(t−l) referred to the effect parameters of Beta at day t−l; ANt referred to the count of patients admitted with unintentional injuries attributable to ambient temperature on t day; nt was the total number of patients with unintentional injuries in the population at day t.
The economic burden of the unintentional injury admissions associated with ambient temperature was further assessed by the Cost of Illness method. Economic burden was defined by the direct cost and indirect cost due to unintentional injury during hospital length of stay.22 The direct cost relates to hospitalisation costs, and indirect cost was estimated by lost productivity during hospital length of stay in this study.23 Economic burden was shown as24:

where Ci denoted the economic burden of subgroup i; Hi was the average hospital cost of subgroup i; ANi referred to the count of patients admitted with unintentional injuries attributable to the ambient temperature of subgroup i; Hi referred to the hospitalisation cost; Hi×ANi referred to the direct cost; GDP′ referred to the daily GDP per capita per day; Ti was the average length of stay in hospital (days) of subgroup i; (GDP′×Ti)×ANi referred to the indirect cost. According to the Tianjin Statistical Yearbook, the GDP per capita per day was ¥101 614 in 2020.25
Sensitivity analysis
In addition, we conducted sensitivity analyses to confirm whether the main findings were robust to different model specifications by changing the lag period of 21 days for the lag-response association to 14 or 28 days.2 In addition, we conducted a sensitivity analysis excluding snow from the DLNM.
Patient and public involvement
Patients and the public were not involved in the design or conduct of the study, formulation of research questions and outcome measures, or the recruitment process.
Results
Descriptive analysis for meteorological variables and unintentional injury admission
Descriptive statistics for daily meteorological variables in Tianjin (2021) were summarised in online supplemental table S2. The median daily mean temperature was 14.2°C, with temperatures ranging from −14.2°C to 30.3°C. The median daily maximum and minimum temperatures were 20.5°C and 9.2°C, respectively. There were 114 (31.2%) rainy days and 8 (2.2%) snowy days.
The epidemiology of patients admitted with unintentional injuries by gender, age, injury mechanism and injury location was summarised in online supplemental table S3. A total of 12 241 patients with unintentional injuries were admitted to Tianjin Hospital in ED in 2021. Among these, 7360 (60.1%) were males, and 4881 (39.9%) were females. For each age group (<18, 18–64 and ≥65 years old), the numbers of patients with unintentional injuries by age were 1118 (9.1%), 7827 (63.9%) and 3296 (26.9%), respectively. Injury mechanisms were road traffic injury (1571, 12.8%), falls (7521, 61.4%), mechanical injury (2830, 23.1%) and others (319, 2.6%). The most common injury locations were upper extremity (4375, 35.7%) lower extremity (3373, 27.6%), and hip and thigh (2828, 23.1%). The leading diagnosis was fracture (9969, 81.4%). The hospitalisation costs were ¥60 907.12 per capita for unintentional injury patients. Online supplemental figure S2 showed daily counts of patients admitted with unintentional injuries during the study period.
Association between ambient temperature and unintentional injury admission on the current day
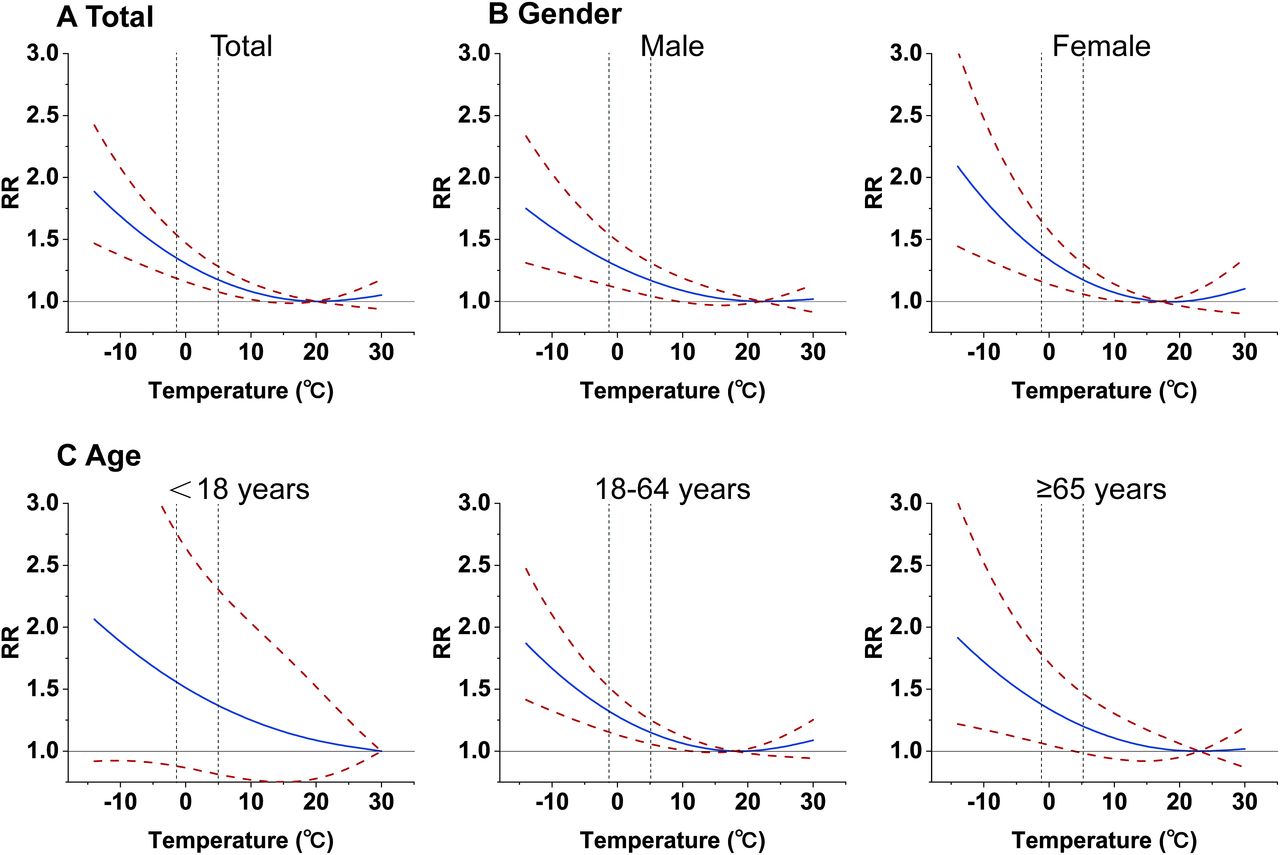
The impact of ambient temperature on the risk of hospital admission for unintentional injury was maximised on the current day (lag 0). The relationship between ambient temperature and hospitalisation for all unintentional injuries followed an L-shaped curve on the current day (figure 1A). Increased risks were found during cold days, with higher risks during more cold extreme temperatures. Significant effects of cold were observed among all unintentional injury patients, with an estimated RR at the 25th percentile (5°C) of 1.18 (95% CI 1.08, 1.28) and the 10th percentile (−1°C) of 1.34 (95% CI 1.18, 1.52) (online supplemental figure S3A and figure 2A). The risk of hospital admission for all unintentional injuries was statistically significant when the temperature was below 11.5°C. The results from this sensitivity analysis excluding snow from the DLNM were consistent with the main analysis.

Association between daily mean temperature and admission for unintentional injury according to age or gender on the current day. Dotted vertical lines represent the 10th temperature and 25th temperature. RR, relative risk.

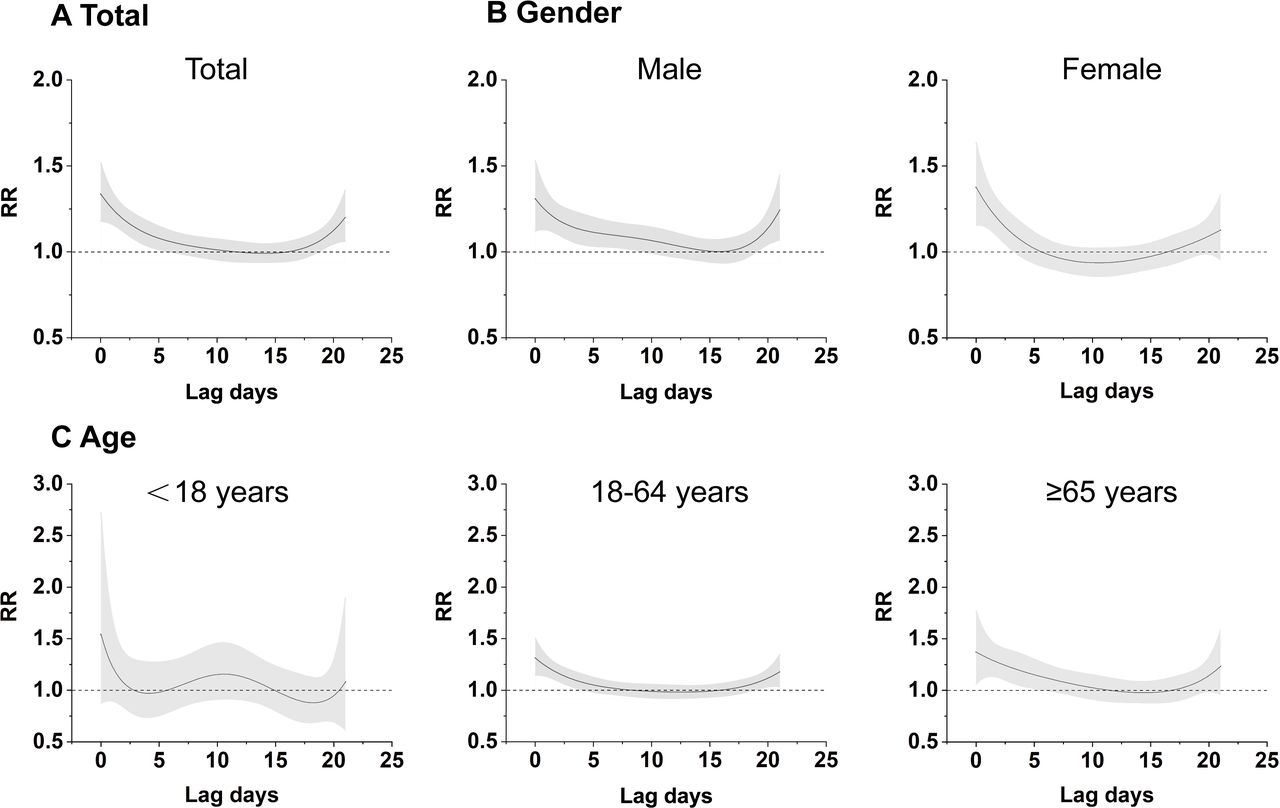
Associations between 10th temperature and unintentional injury over 0–21 lag days according to age or gender. RR, relative risk.
Results revealed that the risk was present for both males and females, with similar temperature-admission curves (figure 1B). Females tend to be more sensitive to cold weather than males. The RR at the 25th percentile on the current day (lag 0) was 1.17 (95% CI 1.04, 1.31) for males and 1.18 (95% CI 1.06, 1.31) for females (online supplemental figure S3B), and the RR at the 10th percentile was 1.31 (95% CI 1.12, 1.53) for males, compared with 1.38 (95% CI 1.16, 1.64) for females (figure 2B).
For age groups, the highest risks were found among people aged ≥65 years old at 1.92 (95% CI 1.22, 3.01), followed by people aged 18–64 years old at 1.87 (95% CI 1.41, 2.47) on the current day (lag 0) at the lowest temperature (figure 1C). RRs for the <18 years old group were not statistically significant. The RR at the 25th percentile on the current day (lag 0) was 1.15 (95% CI 1.06, 1.26) for people aged 18–64 years old and 1.21 (95% CI 0.99, 1.47) for people aged ≥65 years old (online supplemental figure S3C). The RR at the 10th percentile was 1.31 (95% CI 1.15, 1.50) for people aged 18–64 years old, compared with 1.37 (95% CI 1.06, 1.77) for people aged ≥65 years old (figure 2C). The risk of hospital admission for unintentional injury for people aged ≥65 and 18–64 years old was statistically significant when the temperature was below 3.5°C and 11°C, respectively.
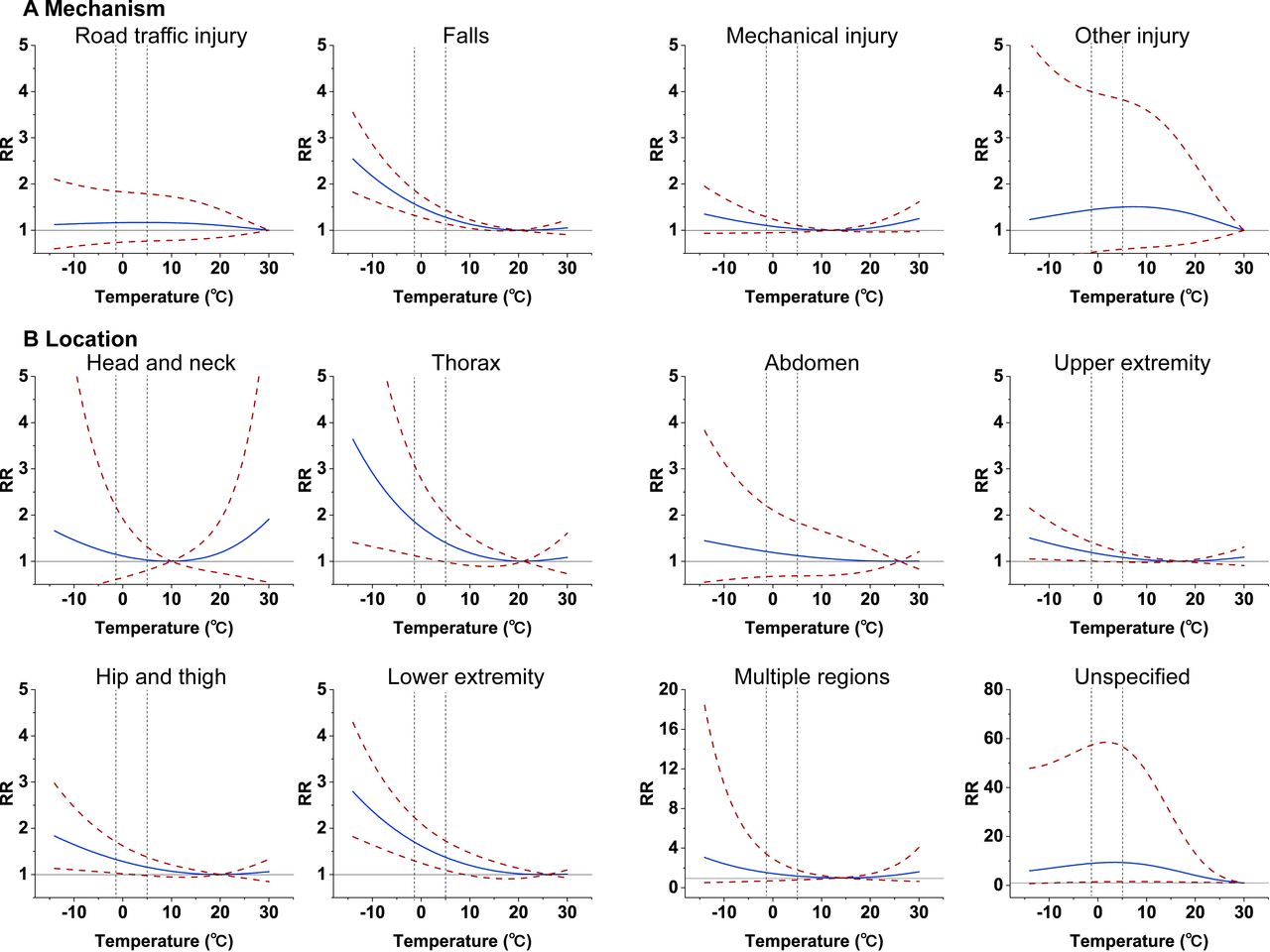
For injury mechanisms, only the risk of falls increased at relatively low temperatures (figure 3A). RR at the 25th percentile (5°C) was 1.28 (95% CI 1.14, 1.44) and the 10th percentile (−1°C) was 1.55 (95% CI 1.31, 1.83). For injury locations, the risks of thorax, upper extremity, hip and thigh, and lower extremity injuries increased at relative low temperatures (figure 3B). Significant effects of cold were observed in fracture patients, with an estimated RR at the 25th percentile (5°C) of 1.23 (95% CI 1.11, 1.36) and in the 10th percentile (−1°C) of 1.44 (95% CI 1.25, 1.66). When the temperature was below 12°C, the risk of fracture hospitalisation was statistically significant.

Association between daily mean temperature and unintentional injury among subgroups according to injury mechanism and injury location on the current day. Dotted vertical lines represent the 10th temperature and 25th temperature. RR, relative risk.
Associations between ambient temperature and unintentional injury admission over lag days
Figure 2 depicted the associations between 10th temperature and unintentional injury over 0–21 lag days. The effects of relative low temperatures on the risk of hospital admission for unintentional injury were presented to be acute (lasting for approximately 5 days), and maximised on the lag 0 days (figure 2A). As the lag increased, the RR of unintentional injury moved close to 1. When stratified by gender and age, the results revealed significant risks lasting for less than 9 days in males, 3 days in females, 4 days in people aged 18–64 years old and 6 days in people aged ≥65 years old (figure 3B,C). For injury mechanisms, significant risks lasted for 7 days for falls (figure 4A). For injury locations, significant risks of thorax, upper extremity, hip and thigh, and lower extremity injury lasted for less than 4, 0, 7 and 3 days. The risk of fracture lasted for less than 6 days. Online supplemental figures S3 and S4 showed the overall cumulative 25th temperature-injury associations over 0–21 lag days. The sensitivity analysis was conducted by changing the lag period of 21 days for lag-response association to 14 or 28 days. It did not alter the main results (online supplemental tables S4–S7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Associations between 10th temperature and unintentional injury over 0–21 lag days according to injury mechanism or injury location. RR, relative risk.
Economic burden of unintentional injuries attributed to relative low temperature
Relatively low temperature was responsible for 25.44% (95% CI 13.74, 33.09) of all unintentional injury patients during the study period, with higher AF for males (30.37%, 95% CI 18.27, 37.77) than that for females (15.54%, 95% CI −13.69, 29.41) (table 1). For age groups, the highest AF was found among people aged ≥65 years old (31.26%, 95% CI 6.78, 42.48), followed by people aged 18–64 years old (21.18%, 95% CI 4.15, 30.87). For injury mechanisms, the highest AF was observed in falls (31.65%, 95% CI 14.77, 40.62). For injury locations, the AF of the hip and thigh (39.92%, 95% CI 19.79, 49.70) was higher than the others. The AF of the fracture was 27.61% (95% CI 15.84, 35.63).
Attributable fractions (AF%), attribute numbers (AN) and economic burden of unintentional injuries attributed to relative low temperature across lag 21-day
Short-term cold exposures were associated with the number of unintentional injury patients (3114, 95% CI 1608, 4036) for several specific subgroups, accounting for 2235 (95% CI 1364, 2824) for males, 1658 (95% CI 443, 2445) for people aged 18–64 years old, 1030 (95% CI 206, 1415) for people aged ≥65 years old, 2381 (95% CI 1143, 3135) for falls, 1129 (95% CI 527, 1411) for hip and thigh injuries, 2753 (95%CI 1449, 3626) for fractures attributable to cold (table 1).
Short-term cold exposures were responsible for ¥197.52 million (95% CI 102.00, 256.00; about 27.10 million dollars) of all unintentional injury patients during the study period, accounting for 26.50% total economic burden, and were associated with the excess economic burden of unintentional injury for several specific subgroups, accounting for 136.46 (95% CI 83.28, 172.42; about ¥18.67 million dollars) million for males, ¥104.62 (95% CI 27.95, 154.27; about 14.34 million dollars) million for people aged 18–64 years old, 74.35 (95% CI 14.87, 102.14; about ¥10.24 million dollars) million for people aged ≥65 years old, ¥155.00 (95% CI 74.41, 204.09; about 21.37 million dollars) million for the falls, ¥93.24 (95% CI 43.52, 116.53; about 12.88 million dollars) million for hip and thigh injury, ¥185.39 (95% CI 97.58, 244.17; about 25.50 million dollars) million for fracture attributable to cold (table 1 and online supplemental table S7).
Discussion
In the current study, 12 241 patients admitted with unintentional injuries were analysed using a time-stratified case-crossover design with a DLNM. One interesting finding is that the risk of unintentional injury significantly increased at relatively low temperatures. Females were more vulnerable to cold weather than males, but the effect on males persisted longer. Relatively low temperatures were linked to an increased risk of unintentional injury in adults, more sensitive in the elderly. The mechanism-specific analyses showed that the risk of falls was significantly associated with relative low temperatures. The location-specific analyses showed that the risks of thorax, upper extremity, hip and thigh, and lower extremity injuries were significantly associated with relative low temperatures. The excess economic burden of unintentional injury associated with relative low temperatures was approximately ¥200 million, and fracture accounted for ¥185 million. The findings have provided a deeper insight into evidence that ambient temperature was associated with risks of unintentional injury admission. The findings have important implications for unintentional injury prevention and control in northern China.
Unintentional injuries increased at relative low temperatures
According to this research, unintentional injury risk was significantly associated with relative low temperatures, which was consistent with several studies. For example, a study conducted in Seoul, South Korea from 2008 to 2016 reported that patients with unintentional injuries who had visited EDs increased significantly at relative low temperatures.2 Another study conducted between 2015 and 2016 in Shenzhen China found that high RR was for traffic accident injuries during cold exposure. However, other studies found that an increase in temperature was only associated with a relatively high risk of injury.12 Therefore, the effect of relative low temperatures has been inconsistent and has not been observed as extensively. This discrepancy could be attributed to differences according to various geographical locations, temperature distribution, social factors and patients’ characteristics.2 For example, Tianjin has four distinct seasons with a freezing winter, and the minimum temperature during winter is below 0°C, which increases the risk of unintentional injury. Besides, the effect of high temperatures on unintentional injuries was not significant, likely owing to the small sample size.
Differences in relationship between unintentional injury risk and relative low temperatures in subgroups
The findings showed that cold temperatures generally had greater impacts on the elderly, which is in line with previous studies.13 26–28 The reason for the results may be that the elderly are more susceptible to injury, associated with their osteoporosis due to calcium loss, and their gradually weakening ability of balance,2 29 30 although older groups were positively associated factors of personal cold protection behaviours.31 The study also observed that people aged 18–64 years old were also more likely to suffer from unintentional injury. In addition, the increased risk of hospital admission for unintentional injury for people aged ≥65 and 18–64 years old is statistically significant when the temperature is below 3.5°C and 11°C, respectively. Young and middle-aged people are more likely and more frequently exposed to outdoor working conditions around 10°C in spring and autumn.32 33 While older people are more likely to fall in winter when the temperature is below 0°C. Therefore, in order to alleviate the injury burden of relatively low temperatures, policymakers need to account for the specific susceptible populations to unintentional injury when formulating targeted adaptation plans and priority protection.
As determined in this study, the increased risk of unintentional injury at relative low temperatures seems related to fall injuries. This finding supports evidence from previous observations.34 Hassi et al found an increase in slipping and falling injuries at low-temperature conditions.35 Therefore, it is likely that the increase in injuries observed, which are associated with relative low temperatures, is caused by one’s physical environment, such as snow or ice on the ground, freezing rain and freezing temperatures, during winter.36 The results from this sensitivity analysis were almost consistent with the main analysis. The reason could be that there were 8 (2.192%) snowy days in Tianjin (2021). As it is conceivable, considering the extremely small sample size, the study lacks statistical power and requires validation in larger sample.
Moreover, in the present study, the risk of fracture increased at relatively low temperatures. A study conducted in Tokyo, Japan over a 3-year period also found that fracture risk was the highest in the winter for some individuals.37 Tenías et al found that the weather series showed a positive tendency, with a greater occurrence of fracture cases in the autumn and winter months.38 Giladi et al, in their study of the population of the USA, observed that the risk of distal radius fractures was higher in the winter months.39 In particular, the risks of thorax, extremity, hip and thigh injury increase at relatively low temperatures in this study. Hip fractures among the elderly represent an important public health problem,40 both because of their high incidence and the serious consequences that derive from them: increased mortality, morbidity and high consumption of medical resources, especially considering the ageing trend of the population in China.
As determined in the study, the effects of relative low temperatures on the risk of hospital admission for unintentional injury present lasted for approximately 5 days, and the risk decreased as the lag days decreased, which is consistent with other evidence that has consistently noted that the effects of relative low temperatures on the injury risk present are acute.41 The lag days could be attributed to the following: (i) patient factors (eg, the time from onset to diagnosis); (ii) meteorological factors (eg, icy ground). These findings suggest that low-temperature warnings for trauma centres may need to last approximately 5 days to prepare for additional service demand pressures.
Economic burden of unintentional injuries increased at relative low temperatures
Previous studies have mainly focused on the economic burden of air pollution.42 To the best of our knowledge, little is known about the economic burden of relative low temperatures on intentional injury. The findings highlight that short-term cold exposures were associated with hospital admission (more than 3000 patients admitted with unintentional injuries) and economic burden (approximately ¥200 million; 27 million dollars) for unintentional injury, especially susceptible groups in males, aged ≥18 years old, the falls, the hip and thigh injury and fractures. The economic impacts of cold weather on males tend to be greater than on females. The reason for the results is the influence of cold weather on males for a longer period than on females, because they are more likely and more frequently exposed to outdoor working conditions.33 Though 83% of houses had central heating in winter in Tianjin, the majority of the population was potentially protected from the outdoor weather. Extremely cold days still posed some increased risks.15 The following prevention measures may be necessary to decrease substantial economic burden: (i) Stratified analyses by gender and age identify vulnerable subgroups and provide warning signals. Public health agencies should consider using these warnings to trigger initiation of injury prevention strategies. (ii) Public health initiatives focused on injury prevention through fall prevention, bike helmets, sport impact policy changes, and other public safety measures. (iii) In addition to standard calendar-related factors (holidays, day of the week, calendar time), incorporating weather into resource planning models can improve the daily allocation of resources and staff of hospital. (iv) Personalised health education is critical for improving prevention practices among vulnerable groups and sensitive disease groups.3
Limitations
The major limitations of this study need to be acknowledged. First, temperature effects could be modified by many factors, and this is a single-city study for 1 year, which limits the generalisability of the findings to other regions and times. Second, temperature data from fixed sites were used rather than individual exposures. In contrast, data from fixed monitoring stations can only reflect meteorological conditions at a particular location and cannot accurately reflect the actual exposure of an individual. The temperature data from fixed sites may cause some inevitable measurement errors. Third, the effects of immediate cold waves and possible interventions by a cold warning system were not considered in this study. Fourth, some factors, such as injury severity, occupation status and public accident, etc, that might confound the associations between ambient temperature and unintentional injury were not controlled. Fifth, COVID-19 pandemic may have had some impact on the results in 2021. Finally, considering the loss of productivity after discharge and intangible costs, the costs of unintentional injury admission attributed to relative low temperatures were underestimated in this research.
Conclusions
This study assessed the association between ambient temperature and economic burden of unintentional injury, and identified characteristics of the population and diseases with high risks. Research results suggest that the risk of hospitalisation for unintentional injury increased when it was below 11.5°C in Tianjin, China. The temperature risk of unintentional injury was presented to be acute and the highest in the absence of the delay effect. Relative low temperature was responsible for approximately 3000 unintentional injury patients, and the economic burden attributable to cold exposures was up to approximately ¥200 million (about 27 million dollars), approximately accounting for 26% of the total economic burden in Tianjin, 2021. People with male, aged above 18 years old, falls, hip and thigh injuries, and fractures were identified as particularly susceptible groups and sensitive diseases to relative low temperature. The findings may clarify the health impacts of temperature on unintentional injury economic burden. It is helpful for informing effective targeted public health interventions to prevent and control unintentional injury, and to increase resilience in response to climate change.
Data availability statement
Data may be obtained from a third party and are not publicly available. The datasets generated during and analysed in the current study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the ethics committee of Tianjin Hospital (2021-175). Data were analysed at the aggregate level, as agreed by the Ethical Committee, and no participants were contacted.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
YL and CY contributed equally.
Contributors YL: conceptualisation, methodology, writing-original draft preparation. CY: resources, data curation, writing-original draft preparation. TL: methodology, software. ZY: resources, data curation. FL: resources, data curation. JL: software, validation. HF: funding acquisition, supervision, writing-original draft preparation. CC: funding acquisition, writing-reviewing and editing. HF and CC are the guarantors.
Funding This work was supported by the National Key R&D Programme of China (grant number No. 2023YFF1204104).
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.