Article Text

Abstract
Background Anaemia is a severe and common complication in patients with aneurysmal subarachnoid haemorrhage (aSAH). Early intervention for at-risk patients before anaemia occurs is indicated as potentially beneficial, but no validated method synthesises patients’ complicated clinical features into an instrument. The purpose of the current study was to develop and externally validate a nomogram that predicted postacute phase anaemia after aSAH.
Methods We developed a novel nomogram for aSAH patients to predict postacute phase anaemia (3 days after occurrence of aSAH, prior to discharge) on the basis of demographic information, imaging, type of treatment, aneurysm features, blood tests and clinical characteristics. We designed the model from a development cohort and tested the nomogram in external and prospective validation cohorts. We included 456 aSAH patients from The First Affiliated Hospital for the development, 220 from Sanmen People’s Hospital for external validation and a prospective validation cohort that included 13 patients from Hangzhou Red Cross Hospital. We assessed the performance of the nomogram via concordance statistics and evaluated the calibration of predicted anaemia outcome with observed anaemia occurrence.
Results Variables included in the nomogram were age, treatment method (open surgery or endovascular therapy), baseline haemoglobin level, fasting blood glucose level, systemic inflammatory response syndrome score on admission, Glasgow Coma Scale score, aneurysm size, prothrombin time and heart rate. In the validation cohort, the model for prediction of postacute phase anaemia had a c-statistic of 0.910, with satisfactory calibration (judged by eye) for the predicted and reported anaemia outcome. Among forward-looking forecasts, our predictive model achieved an 84% success rate, which showed that it has some clinical practicability.
Conclusions The developed and validated nomogram can be used to calculate individualised anaemia risk and has the potential to serve as a practical tool for clinicians in devising improved treatment strategies for aSAH.
- Clinical Decision-Making
- Change management
- Risk management
- Stroke
- Nursing Care
Data availability statement
Data are available on reasonable request. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Novel nomogram: The study introduces a novel nomogram that integrates various patient characteristics and clinical features to predict postacute phase anaemia after aneurysmal subarachnoid haemorrhage (aSAH), filling a crucial gap in predictive tools for this condition.
Robust predictive ability: The study’s substantial cohort of 456 aSAH patients, alongside external and prospective validation cohorts, strengthens the generalisability of the findings, with the predictive model exhibiting a high c-statistic of 0.910 in the validation cohort, signifying robust predictive performance for postacute phase anaemia.
Comprehensive variables: The nomogram incorporates a wide range of variables, including demographic information, imaging, treatment type, aneurysm features, blood tests and clinical characteristics, providing a holistic approach to prediction.
Generalisability: Although the study includes external validation, the cohorts are from specific hospitals, potentially limiting the generalisability of the nomogram to broader patient populations.
Prospective validation and clinical Implementation: While including a prospective validation cohort, the practical implementation and impact on clinical decision-making may require further real-world evaluation.
Introduction
Despite significant advances in endovascular intervention and microneurosurgical clipping for the treatment of ruptured intracranial aneurysms, patients with aneurysmal subarachnoid haemorrhage (aSAH) still face many postprocedural complications. Anaemia is a severe complication that occurs in 30%–50% patients with aSAH.1–5 Anaemia after aSAH worsens cerebral oxygen delivery, leading to a higher rate of cerebral infarction and is associated with unfavourable poor long-term neurological outcome and mortality.6 7 Conversely, elevated haemoglobin levels in patients with aSAH correlate with improved outcomes.7 8 Physiological and preclinical evidence shows that anaemia affects a secondary brain injury after aSAH, which is potentially modifiable.1
Post-aSAH anaemia has been treated by red blood cell (RBC) transfusion but significant transfusion-related risks result in poorer outcomes and increased complication rates.9However, packed RBC transfusion has been shown to improve brain tissue oxygen delivery after SAH.10–12 Several clinical trials have demonstrated that erythropoietin increases brain tissue oxygen tension and reduces vasospasm and delayed ischaemic deficits in patients with post-SAH anaemia.13–15 A recent randomised, double-blind, placebo-controlled phase 2 clinical trial revealed that patients with delayed ischaemic neurological deficits after aSAH were more susceptible to complications of anaemia.1 Additionally, packed RBC transfusion was beneficial for patients with no prior anaemia. The authors emphasised that blood transfusion in critically ill patients could frequently serve as an independent risk factor for poor outcomes. This suggests that individuals who are already anaemic may have passed a critical threshold for adverse outcomes and mortality, rendering blood transfusion ineffective as a late intervention.
Based on current evidence, there is significant clinical value in identifying at-risk patients before anaemia occurs and it may be beneficial to reserve treatment aimed at increasing brain oxygen delivery for those patients. Anaemia following aSAH arises from complex and multifaceted causes, extending beyond surgical intervention. There is currently no tool to integrate patients’ complex clinical profiles and multiple conflicting predictors into an objective, comprehensive, validated risk assessment.
In this study, we aimed to develop and validate a nomogram (a statistical tool that incorporates numerous variables to assess the occurrence rate of a specific outcome), to predict postacute phase anaemia (3 days after aSAH).16 This phase was selected because vasospasm and delayed cerebral ischaemia usually arise 3–4 days after aSAH, whose devastating consequences can be exacerbated by anaemia.17 18
Methods
Study design, patients and procedures
A nomogram was developed from a patient cohort from the Department of Neurosurgery, The First Affiliated Hospital, Zhejiang University School of Medicine (Hangzhou, China). A retrospective cohort study of aSAH patients admitted between 1 March 2009 and 31 December 2018 was conducted. Patients were eligible if they were admitted within 2 days of aSAH, confirmed by CT angiography or digital subtraction angiography within 24 hours of admission. Patients with a history of trauma, vascular malformation or other non-aneurysmal bleeding, and patients who died within 5 days of diagnosis were excluded.
All ruptured aneurysms were treated according to institutional guidelines by open surgery or by endovascular methods within 2 days of admission, and if patients or relatives denied permission for both therapies, conservative treatment was administered (including simple external ventricular drainage when necessary). Vasospasm and delayed cerebral ischaemia usually appear about 1 week after onset of aSAH and gradually resolve after 2 weeks. After that, patients received dynamic head CT periodically to detect vasospasm and delayed cerebral ischaemia. Nimodipine was used in all patients to prevent complications.19
Anaemia was tolerated unless haemoglobin level was <70 g/L.6
Data collection
The following data were extracted from the electronic medical record system: demographic information including age, sex, body weight, body mass index, history of hypertension, diabetes, heart disease, smoking, alcohol consumption and history of stroke. Severity of clinical status on admission was evaluated by Glasgow Coma Scale (GCS) score, and severity of haemorrhage on admission was graded on CT scans using the modified Fisher score20 and Graeb score.21 The presence of hydrocephalus requiring ventricular drainage or serial lumbar puncture on admission was also recorded. On-admission haematological variables including haemoglobin, white cell count, C reactive protein level, international normalised ratio (INR), prothrombin time, D-dimer, fasting blood glucose, alanine and aspartate aminotransferases, alkaline phosphatase and creatinine were extracted. The on-admission systemic inflammatory response syndrome (SIRS) score was also assessed according to the number of following standard criteria met22: heart rate >90 bpm, respiratory rate >20 breaths/min, body temperature >38℃ or <36℃, white cell count <4.0 or >12.0×109/L. On-admission vital signs including heart rate and systolic/diastolic pressure were recorded. Location and size of the ruptured aneurysm were recorded. Details of open surgery, endovascular intervention or other methods (eg, conservative therapy with or without ventricular drainage) were extracted.
Study outcome was postacute phase anaemia, which was defined as haemoglobin <10 g/dL 3 days after occurrence of aSAH, prior to discharge.
To validate the nomogram, we used data collected at the neurosurgical department of another provincial regional medical centre (Sanmen People’s Hospital) from 1 January 2004 to 31 March 2019. These data shared identical clinical characteristics and adhered to the same inclusion and exclusion criteria as the development cohort. A uniform protocol for data entry between two collaborating centres was achieved by the development of comprehensive instructions defining variables and outcomes used in the study.
In addition to the previously mentioned medical centres, we expanded our validation efforts by incorporating data from patients treated at the Hangzhou Red Cross Hospital. This prospective validation included patients who received medical care at the hospital from 12 March 2024 to 2 April 2024. The aim of this additional dataset was to strengthen the robustness and ability to generalise our findings.
Statistical analysis
SPSS V.22 (SPSS) and R V.3.5.3 (R Foundation for Statistical Computing, Vienna, Austria) were used for statistical analysis. All values were expressed as mean and SD or median and IQR. Baseline factors were analysed in relation to development of anaemia using univariate logistic regression and variables with p<0.10 were entered into a backward stepwise analysis using multivariate logistic regression. The conventional threshold for inclusion is often set at p<0.05, but a threshold of p<0.10 was used in this study to ensure that potentially relevant variables were not overlooked, thus allowing for a more comprehensive assessment of potential predictors within the model. The significance of the variables in the model was also determined by statistical measures such as p values, CIs and other relevant statistical metrics. These measures were used to assess the strength and reliability of the associations between the variables and the outcomes within the model. We also considered several interactions with surgery or non-surgical treatment in the models if significant. Area under the receiver operating curve was calculated. The Hosmer-Lemeshow test was performed to validate the goodness of fit for logistic regression models. The Mann-Whitney test was used for comparison of factors in the final model, such as age and baseline haemoglobin in the development and validation cohorts. The χ2 test was used for comparison of aneurysm size and treatment and anaemia. The expectation-maximisation algorithm was used to input missing values. Body weight was not included in the final model because it was not available for >25% of patients and its inclusion would have excluded all these patients.
Significant interaction term in statistics refers to a term in a model (eg, regression model) where the effect of one variable on the dependent variable is modified by another variable. When this interaction term is statistically significant, it indicates that the relationship between the independent and dependent variables changes in accordance with the level of the moderating variable. In essence, it suggests that the combined effect of the variables is not simply additive, but rather affects the outcome in a way that cannot be explained by the individual effects of each variable alone.
The calibration of the model was evaluated visually with the calibration curve, which measured the matching degree between the observed outcomes in the current cohort and the outcomes predicted by the models. Perfect calibration, when the predictive model perfectly matched the patient’s real risk, was indicated by a 45° line while any deviation above or below the line demonstrated underprediction or overprediction, respectively.
Patient and public involvement
In this study, patient and public involvement was pivotal in shaping the research. As this was not a randomised controlled trial, assessment of intervention burden by patients did not apply. Because of that, patient consent was not required as the study relied on anonymised data from medical records.
Although this is a retrospective study, efforts were made to ensure that patient perspectives were considered in the interpretation of historical data. Their historical experiences have been instrumental in shaping the approach of this study, ensuring that it remains considerate of their unique circumstances. Through direct engagement and dialogue, we gained insights into the challenges and concerns faced by individuals affected by aSAH.
The results of this study will be disseminated to all relevant study participants, where possible. We are committed to sharing the findings in a manner that is accessible and understandable to those who contributed to the research. Additionally, we will seek feedback from participants to ensure that the results are effectively communicated and that their perspectives are considered.
The patient advisers were acknowledged for their contributions to the institution’s research efforts, although they were not directly involved in this specific study. Patients and the public were not directly involved in the conduct of this retrospective case–control study.
Results
Demographics and clinical characteristics
For the development cohort, 617 patients with aSAH were screened. We excluded patients admitted >2 days after occurrence of aSAH (n=55), and patients with a combination of a history of trauma (n-37), vascular malformation (n=26), other non-aneurysmal bleeding (n=13), or death within 5 days/length of hospital stay <5 days (n=30), leaving a final sample of 456 patients. The same procedure was used to screen patients in the validation cohort, and 220 patients were eventually included.
We preliminarily collected the following data from the electronic medical record system: age, aneurysm size, GCS score, treatment plan and on-admission haematological variables including haemoglobin level, prothrombin time, fasting blood glucose, SIRS score and heart rate. Treatment was categorised into three groups: open craniotomy with clipping; intravascular interventional therapy; and non-surgical treatment and drainage for patients with acute hydrocephalus. Endovascular interventional therapy was further divided into simple and stent-assisted coil embolisation.
Demographics and clinical characteristics were comparable between the development and validation cohorts (online supplemental table 1). The proportion of patients who developed postacute phase anaemia during hospitalisation was 34% in the development cohort and 44% in the validation cohort.
Supplemental material
Model construction
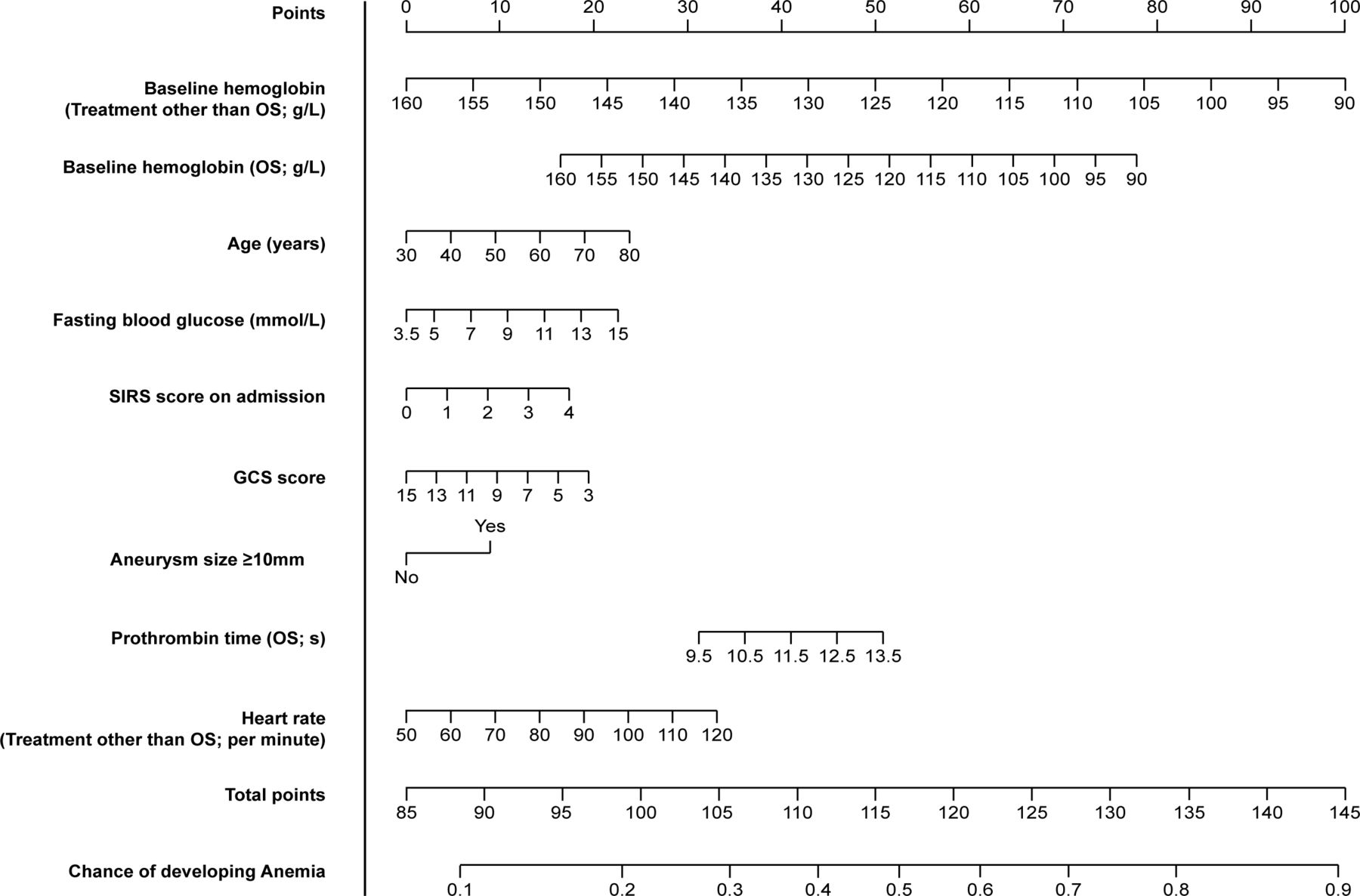
After determining the homogeneity of patients in the development and validation cohorts, we collected the demographic and clinical characteristics of the patients. Univariate risk factors for screening of candidate clinical variables were assessed. ORs and p values of all variables tested are listed in online supplemental table 2. For the purpose of identifying the most robust predictors and eliminating potential collinearities, multivariate logistic regression analysis was performed. The final model contained 7 of the 21 initially investigated variables and 3 interaction terms (table 1). The Hosmer-Lemeshow test indicated no lack of fit (p=0.795). The nomogram to predict the probability of postacute phase anaemia after aSAH was created from this model (figure 1).

Nomogram to predict postacute phase anaemia after aSAH. Instructions: record the patient’s age and draw a vertical line upwards from the variable to determine the points the patient receives for their age. Repeat the process for fasting blood glucose, SIRS score and aneurysm size (whether ≥10 mm or not). Specifically, for patients receiving OS or other treatment, respective variables should be used: OS, baseline haemoglobin (OS, g/L) and prothrombin time (OS, s); treatment other than open surgery, baseline haemoglobin (treatment other than OS) and heart rate (treatment other than OS, per minute). Locate the final sum on the total points axis and draw a vertical line to the chance of developing anaemia axis to predict the probability of developing postacute phase anaemia after aSAH. aSAH, aneurysmal subarachnoid haemorrhage; GCS, Glasgow Coma Scale; OS, open surgery; SIRS, systemic inflammatory response syndrome.
Significant variables in nomogram in the development cohort
Reliability verification
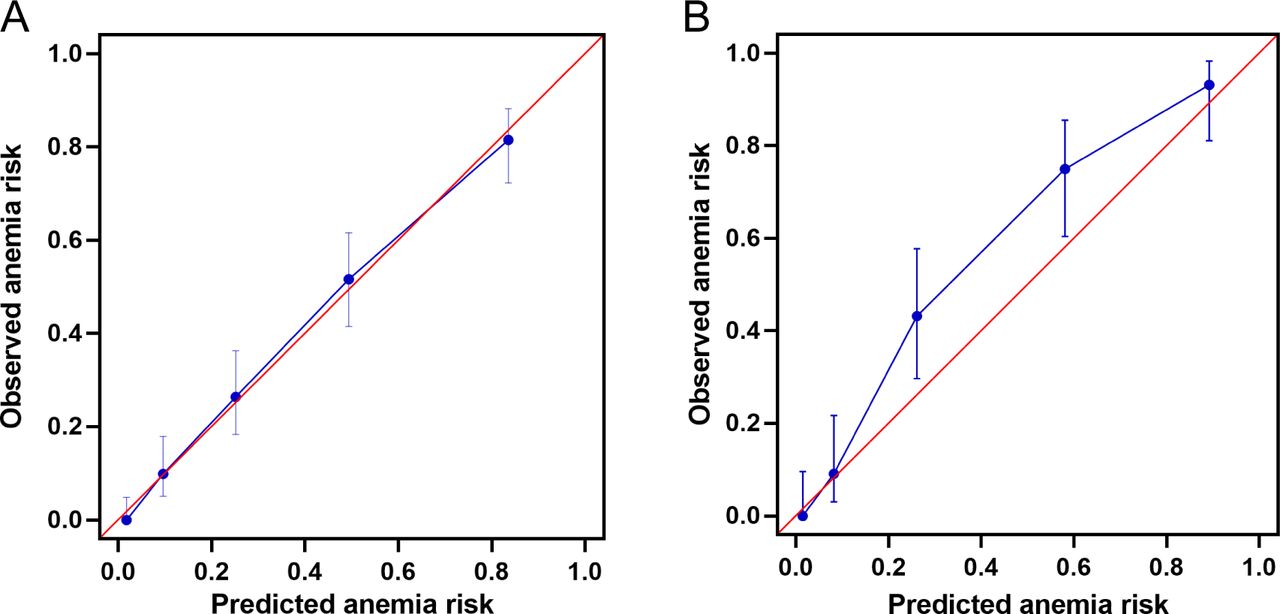
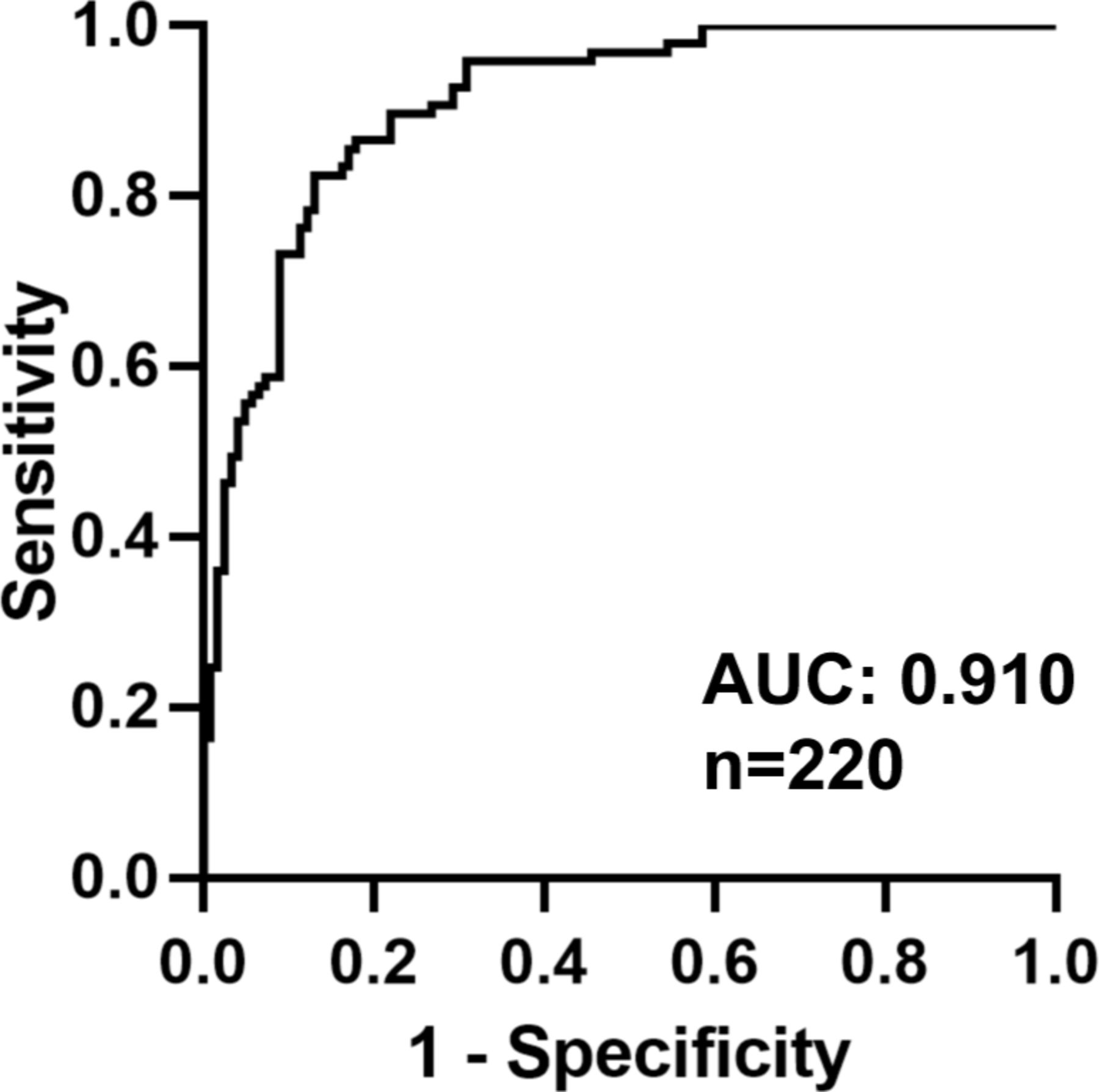
Internal validation via calibration plot for the probability of postacute phase anaemia showed a good correlation between the observed and predicted outcomes (figure 2A). The external validation cohort consisted of 220 patients. 97 patients (44%) developed postacute phase anaemia during hospitalisation. The model for prediction of postacute phase anaemia had a c-statistic of 0.910 (figure 3), with satisfactory calibration for the anaemia risk (figure 2B).

Calibration curves for internal (A) and external validation (B) of the prediction of postacute phase anaemia.

{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curve analysis of nomogram for predicting postacute phase anaemia in the external validation cohort. AUC, area under the curve.
In addition to the internal and external validation described above, we conducted a prospective cohort study (online supplemental table 3). Of the 13 patients included in the cohort, 5 developed anaemia during treatment and the rest did not develop anaemia. The overall predictive success rate was 84%.
Discussion
Postacute phase anaemia in patients with aSAH is caused by a variety of factors, but primarily blood loss is caused by disease and treatment and is an obstacle to regenerating RBCs. Aneurysm surgery can cause anaemia by intraoperative blood loss and by inhibiting the response of bone marrow to erythropoietin due to activation of systemic inflammation by aSAH. In this study, we developed and validated a novel nomogram for aSAH patients to predict postacute phase anaemia, which showed satisfactory predictive accuracy. The key variables identified from the development cohort and recognised in the validation cohort were age, treatment method (open surgery or endovascular therapy), baseline haemoglobin level, fasting blood glucose, SIRS score on admission, GCS score, aneurysm size, prothrombin time and heart rate. Several studies have been published on anaemia outcomes and targeted treatment after aSAH,1 23–27 yet there is still a lack of evidence for proper management of post-aSAH anaemia. Current aSAH treatment guidelines recommend RBC transfusion in anaemic patients with risk of cerebral ischaemia, although no thresholds for transfusion are suggested.28–30 Two significant concerns impede the widespread application of anaemia-targeted RBC transfusion. (1) Whether transfusion is genuinely effective in improving outcomes for all aSAH patients with anaemia, or if its effectiveness is limited to a specific subgroup. (2) When is the proper timing for the transfusion? The answer to these concerns remains unclear, yet accumulating recent evidence indicates that aSAH patients are likely to benefit from transfusion when facing delayed cerebral ischaemia, and RBC transfusion is particularly beneficial for patients before anaemia actually occurs.1 31
Given the potential benefits of treating patients at risk of anaemia, several risk factors for anaemia outcomes have been identified. The conflicting results between anaemia and adverse outcomes may be due to the fact that previous studies were usually retrospective, single-centre, observational cohort studies, resulting in small sample sizes that made it difficult to draw firm conclusions.32 These findings underscore the unmet need to incorporate these predictors into patient decision-making processes. However, there is no instrument to synthesise patients’ complicated clinical features into a comprehensive and objective prediction of anaemia outcome, particularly when the decision in question is as important as how the anaemia would be treated.
In accordance with prior research,33 we collected data across seven key categories for our analysis. (1) Demographic information: age and sex; (2) medical history: hypertension, diabetes mellitus, smoking, alcohol use, stroke and heart disease; (3) clinical scores: GCS score, SIRS score on admission, Modified Fisher scale score, and Graeb score; (4) laboratory tests: baseline haemoglobin, INR, prothrombin time, D-dimer, fasting blood glucose, alanine and aspartate aminotransferase, alkaline phosphatase, creatinine, systolic and diastolic blood pressure, heart rate, white cell count, body weight and BMI; (5) aneurysm related details: treatment (open surgery, endovascular, other), size ≥10 mm and location (eg, posterior circulation); (6) length of hospital stay and (7) postoperative outcomes: symptomatic vasospasm, mortality and high-sensitivity CRP. This comprehensive dataset allowed a thorough analysis across various dimensions.
Many risk factors are associated with the development of anaemia. After univariate risk factors analysis, age, sex, smoking history, alcohol consumption, GCS score, SIRS score on admission, modified Fisher scale score, baseline haemoglobin, treatment, INR, prothrombin time, D-dimer, fasting blood glucose, aspartate aminotransferase, alkaline phosphatase, heart rate, body weight and aneurysm size were closely related to the occurrence of anaemia. Occurrence of anaemia was associated with morbidity and mortality, even after controlling for age, bleeding severity and other clinical factors such as surgical treatment or angiographic vasospasm. In our research, patients who developed anaemia tended to have longer hospital stay, higher levels of inflammation and greater mortality. In addition, they were more likely to suffer blood vessel spasms. Although there was a strong association between anaemia and adverse outcomes, it was difficult to establish causation in retrospective analyses.32 Some researchers have questioned the clinical significance of the occasionally small differences in haemoglobin concentrations observed between patients with good or poor outcomes.8 34
Based on univariate risk factors, we finally identified 7 of the 21 initially investigated variables and 3 interaction terms by multivariate logistic regression analysis. Our nomogram is a practical instrument to offer patient-centred and individualised prediction of anaemia after aSAH. Our model consists of easily ascertainable clinical characteristics to provide prediction of anaemia outcome at a period of greatest susceptibility for poor outcome (postacute phase after aSAH).
Our study had several strengths. First, to our knowledge, this is the first tool for predicting anaemia complication in patients with aSAH. Given that the accuracy of anaemia estimation is crucial for early intervention, our results, derived from an externally validated nomogram, provided improved accuracy in estimating nomogram performance. This enhances our ability to generalise the study findings and broadens applicability of the nomogram in different populations. Second, the nomogram was based on readily available clinical characteristics, making it suitable for diverse applications. Consequently, this tool might be particularly helpful and encouraging when early treatment for post-aSAH anaemia is intended. Third, the instrument accounts for different types of operation and various interactions were evaluated.
The decision to manage anaemia after aSAH is still complicated and challenging, which is definitely not solely based on the risk of anaemia occurrence. For example, an early intervention that leads to complete avoidance of post-aSAH anaemia at the expense of infarction or infection might still be considered a failure. Therefore, our nomogram is not intended to replace clinical decision-making, but rather to enhance it by providing objective and quantifiable evaluation of post-aSAH anaemia outcome, which is a pivotal factor influencing clinical decision-making.
There were some limitations that should be considered. First, although our nomogram was derived from a large development cohort, the validation cohort consists of only one external institution with limited datasets. In spite of the high c-statistic on the absolute scale, further work is needed to validate the instrument in a diverse, multicentre international cohort. Second, our nomogram did not include other critical post-aSAH outcomes of interest including vasospasm, delayed cerebral ischaemia and clinical prognosis. Third, other than open surgical clipping, we did not specify diverse types of endovascular treatment; however, endovascular interventions to treat aSAH are becoming increasingly common, with rapidly advancing technologies and many treatment strategies. Fourth, although we conducted external and prospective validations, our study was confined to the East Asian population. Future research should involve multicentre studies encompassing samples from different ethnicities and geographical regions to validate and expand the generalisation of our findings. Such research can help ascertain whether the risk factors identified and predictive models developed remain robust across diverse populations, providing more comprehensive guidance for clinical practice.
Conclusions
We developed and externally validated a nomogram for predicting postacute phase anaemia after aSAH. The proposed nomogram represented a satisfactory predictive accuracy for postacute phase anaemia. It can be used to calculate individualised anaemia risk, and although further studies are necessary, this nomogram could become a practical tool, providing valuable information and clinical evidence for clinicians to enhance treatment of aSAH.
Data availability statement
Data are available on reasonable request. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Both Ethics Committee of The First Affiliated Hospital, Zhejiang University School of Medicine, Sanmen People’s Hospital and Hangzhou Red Cross Hospital approved the use of prospectively collected data and as all data were deidentified, waivers for individual patient consent were obtained from both institutions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
FW, HC and ZL contributed equally.
Correction notice This article has been corrected since it was first published. Affiliation for 'Huai Chen' has been updated.
Contributors FW was a major contributor in planning and design of the study, data analysis, interpretation and writing of the manuscript. HC, ZL, DY, and XW collected and analysed the data. LZ, ZX and DW contributed to data collection. JS and RZ contributed to the planning and design of the study. YZ was a major contributor to the planning and design of the study and reviewing of the manuscript. YZ and FW are responsible for the overall content as guarantor. All authors read and approved the final manuscript.
Funding National Nature Science Foundation of China (No. 81701208) supported this study in the design process. The Medicine and Health Research Foundation of Zhejiang Province (2019KY395) and the Key Research & Development Plan of Zhejiang Province (No.2019C03034) supported this study in design, data collection, analysis and interpretation of data.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.