Article Text

Abstract
Objectives The objectives are to assess smoking abstinence and its effects on vascular risk and to report tobacco-cessation counselling and pharmacotherapy use in patients who had a recent minor stroke or transient ischaemic attack (TIA).
Design and setting The TIA registry.org project is a prospective, observational registry of patients with TIA and minor stroke that occurred in the previous 7 days with a 5-year follow-up, involving 61 sites with stroke specialists in 21 countries (Europe, Asia, Latin America and Middle East). Of those, 42 sites had 5-year follow-up data on more than 50% of their patients and were included in the present study.
Participants From June 2009 through December 2011, 3847 patients were eligible for the study (80% of the initial cohort).
Outcomes Tobacco counselling and smoking-cessation pharmacotherapy use in smoking patients were reported at discharge. Association between 3-month smoking status and risk of a major cardiovascular event (MACE) was analysed with multivariable Cox regression model.
Results Among 3801 patients included, 835 (22%) were smokers. At discharge, only 35.2% have been advised to quit and 12.5% had smoking-cessation pharmacotherapy prescription. At 3 months, 383/835 (46.9%) baseline smokers were continuers. Living alone and alcohol abuse were associated with persistent smoking; high level of education, aphasia and dyslipidaemia with quitting. The adjusted HRs for MACE at 5 years were 1.13 (95% CI 0.90 to 1.43) in former smokers, 1.31 (95% CI 0.93 to 1.84) in quitters and 1.31 (95% CI 0.94 to 1.83) in continuers. Using time-varying analysis, current smoking at the time of MACE non-significantly increased the risk of MACE (HR 1.31 (95% CI 0.97 to 1.78); p=0.080).
Conclusion In the TIAregistry.org, smoking-cessation intervention was used in a minority of patients. Surprisingly, in this population in which, at 5 years, other vascular risk factors were well controlled and antithrombotic treatment maintained, smoking cessation non-significantly decreased the risk of MACE.
- Stroke
- Risk Factors
- PREVENTIVE MEDICINE
- Cardiovascular Disease
- Adult neurology
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study was prospective, limiting recall bias and included a large number of participants in 21 countries and 3 continents.
Multiple individual data were taken into account in the multivariable logistic regression model to limit confounder variables.
As smoking status can vary from time to time, we used time-varying analysis to assess the association between smoking and major cardiovascular event occurrence.
As smoking status was declarative and not confirmed by objective measurement such as CO2 measurement of expired air carbon monoxide, the association between smoking status and occurrence of major cardiovascular event could have been biased.
As patients were enrolled in specialised stroke centres, results of this study could be not representative of the general stroke population.
Introduction
Despite a decrease in the use of tobacco products, about one in five adults are currently smoking worldwide.1 Cigarette smoking is a well-established major risk factor for ischaemic stroke,2–6 with a population-attributable risk of approximately 15%.5 Observational studies have suggested that smoking cessation could reduce the risk of first and recurrent stroke over and above the effect of strictly controlled vascular risk factors and antithrombotic drug use and is associated with lower risk of vascular mortality.7–12 It has been estimated that for every 43 patients who quit smoking after a stroke, 1 stroke recurrence could be avoided annually.13 For these reasons and despite the lack of randomised trial evidence, the American Heart Association and other regulatory authorities list smoking cessation after a stroke as a Class I recommendation.14 However, only a third of smokers quit smoking after a cerebrovascular event.15 Smoking cessation can be challenging due to the highly addictive nature of tobacco. It requires willpower and sustained support, which can be provided by healthcare professionals through a combination of behavioural therapy and pharmacological interventions.16 However, it is largely unknown to what extent appropriate programmes and cessation advice, including smoking cessation pharmacotherapy, are implemented in stroke units. Given the serious consequences of smoking continuation after a stroke, identifying patients most in need of smoking cessation assistance is crucial. Several single-centre studies with limited sample sizes have identified predictors of tobacco abstinence after a stroke, including motivation, immediate disruption after stroke, residual handicap, high educational and socioeconomic levels, and absence of a smoking partner at home.17–19 On the other hand, male sex, living alone, high nicotine dependence assessed by the Fagerström test and depression were associated with an increased risk of persistent smoking.19–22
However, data from large multicentre registries are lacking.
In a large international prospective cohort of patients with recent transient ischaemic attack (TIA) and minor ischaemic stroke, we aimed to describe stroke neurologists' involvement in smoking cessation, to identify predictive factors for smoking cessation, and to estimate the impact of smoking cessation on the risk of recurrent major vascular events.
Methods
Study design and participants
We used data from the TIAregistry.org registry. A description of the study rationale and design has been published earlier.23 Briefly, the TIA-registry.org study is an international, prospective, observational registry of patients with recent TIA or minor ischaemic stroke, designed to assess the 5-year risk of major vascular event (stroke, myocardial infarction (MI), vascular death or other atherothrombotic events) that enrolled 4789 patients between June 2009 and December 2011. Eligibility criteria were age 18 years or older, TIA or minor stroke (modified Rankin scale (mRS), scores of 0, no symptom, or 1 no disability) that occurred within the 7 days of stroke specialist evaluation. Sites from 21 countries were selected on the existence of a dedicated TIA patient care system staffed by stroke specialists, with a volume of at least 100 patients annually during the previous 3 years. Data were prospectively collected, using a standardised web-based case report form, at the time of evaluation of the qualifying event (baseline) of the patient, then at 1, 3 and 12 months after baseline and every 12 months thereafter for 5 years. At baseline, information was obtained on medical history, clinical symptoms of the qualifying event and sociodemographic characteristics; investigations (including brain and cerebral-artery imaging and cardiac investigations) and management of care were recorded. Influenza vaccination status was collected as a marker of good health behaviour. Aetiological subtype was assigned to each patient according to the TOAST (Trial of Org 10172 in Acute Stroke Treatment) classification.24 Patients were evaluated at follow-up for major vascular event occurrence, adherence to standard preventive therapies and main risk factors (smoking status, blood pressure and lipid profile).
Smoking status
At baseline, smoking behaviour was classified into four categories: ‘never smokers’, ‘former smokers’ and ‘current smokers’. Current smokers were also asked daily consumption of cigarettes (≤10; 11–20; 21–30 or ≥31) and delay between wake up and first cigarette smoked (≤5 min, 6–30 min, 31–60 min, ≥60 min) (shortened Fagerström test). Asking for advising to quit by healthcare professional and prescription of smoking cessation pharmacotherapy at discharge were specifically investigated by dedicated questions. Smoking status was recorded at each follow visit. Patients were further classified as quitters and continuers according to their smoking status at the 3-month follow-up visit.
Statistical analysis
Categorical variables were expressed as number (percentage). Quantitative variables were expressed as mean (SD) in case of normal distribution and median (IQR) otherwise. The normality of distribution was assessed graphically and using the Shapiro-Wilk test.
We identified factors associated with smoking cessation at 3 months using univariable and multivariable logistic regression models. Multivariable model was done by including all candidate factors associated with the study outcome with nominal p value <0.10 in univariate analyses and by using a backward-stepwise selection procedure with a removal criteria of 0.05. We forced motor deficit (as symptoms of qualifying event) in the model.
We compared the 5-year event rates (primary and secondary outcomes) between tobacco status (never, former, quitter and continuer) using the Cox proportional hazard regression model (for vascular death and all-cause death) or using a Fine and Gray regression model with non-vascular death as a competing event.
Before developing the multivariable model, we examined the proportional subhazard assumptions for each candidate factor of recurrent major cardiovascular events by using the Schoenfeld residual plots, the log-linearity assumption for continuous candidate predictors by using restricted cubic spline function25 and the absence of colinearity between candidate predictors to multivariable analysis by calculating the variance inflation factors.26
To avoid case deletion in multivariable analyses due to missing data in candidate factors, multivariable analysis was performed after handling missing values by multiple imputations using a regression-switching approach (chained equations with m=10). The imputation procedure was performed under the missing-at-random assumption using all baseline characteristics and outcomes with a predictive mean matching method for continuous variables and logistic regression model (binary, ordinal or polynomial) for categorical variables. Estimates obtained in the different imputed data sets were combined using Rubin’s rules.27 Finally, because tobacco status can change over time, we examined the relation between smoking status and 5-year major vascular event rate by using time-varying variable into univariable Cox proportional hazard regression model.
Statistical testing was conducted at the two-tailed α-level of 0.05. Data were analysed using the SAS software V.9.4 (SAS Institute).
Patient and public involvement
Patients and the public were not involved in the design, conception and conduct of this study.
Results
Study population and baseline data
From June 2009 through December 2011, 61 sites in 21 countries enrolled 4789 patients in the TIAregistry.org project. Of the 61 sites, 42 had follow-up data on more than 50% of their patients at 5 years, who represented 3847 patients eligible for the present study, that is, 80% of the initial cohort (online supplemental file). The median percentage of patients with 5-year follow-up in these selected centres was 92.3% (IQR 83.4%–97.8%). Of these, 46 patients with no information about their baseline smoking status were excluded. Therefore, a total of 3801 patients (79.4% of the original cohort) were analysed in this study. At baseline, 2024 (53.2%) were never smokers, 942 (24.8%) were former smokers and 835 (22%) were current smokers. Among current smokers, according to their 3-month smoking status, 383 were defined as quitters and 434 as continuers (online supplemental figure 1). Baseline characteristics of these patients are summarised in table 1.
Supplemental material
Baseline data among quitters and continuers with smoking status at 3 months (18 patients have missing data)
Use of tobacco cessation therapy after discharge
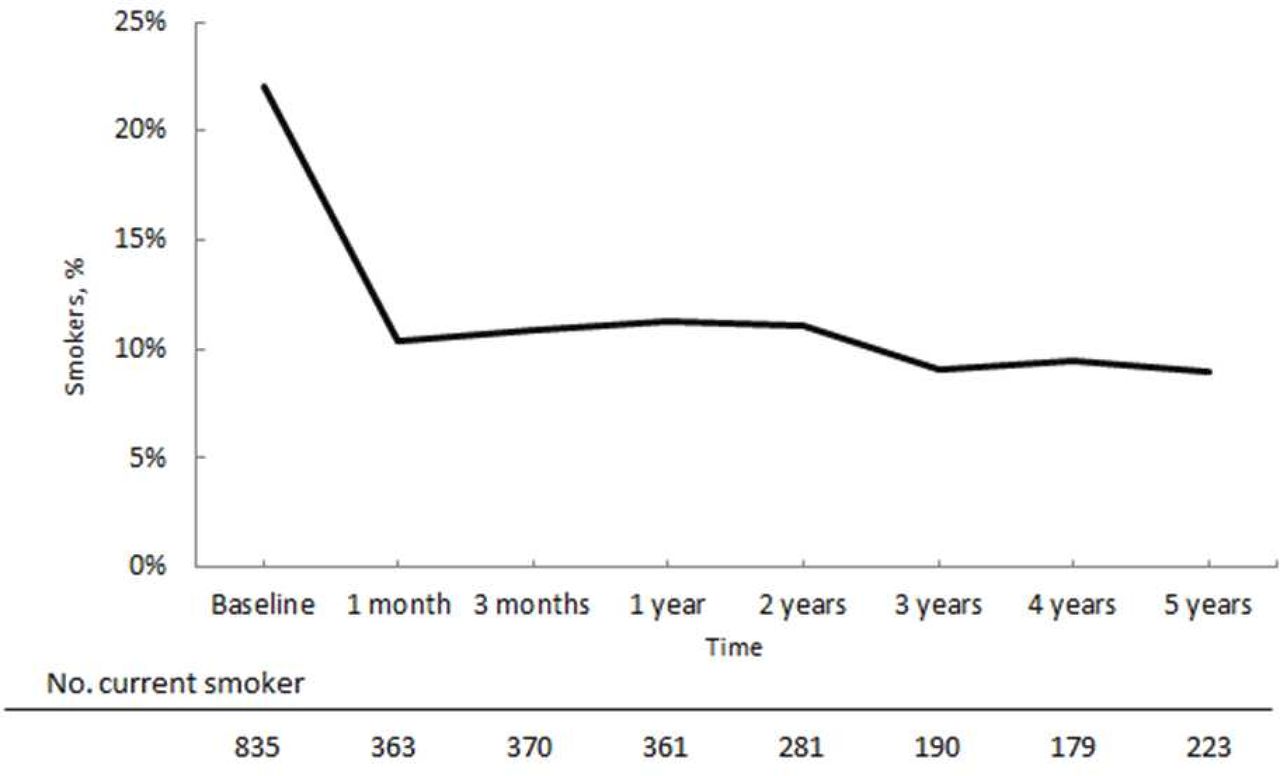
At discharge, 61.8% of current smokers had been advised to quit by a health professional (including a stroke neurologist), 21.6% had been prescribed smoking cessation pharmacotherapy (nicotine replacement 95.2%, varenicline 4.9% and other 3.8%) and 383 patients had quit smoking at 3 months (table 2). After inclusion, the percentage of smokers decreased dramatically 1 month after the qualifying cerebrovascular event, but only slightly over the next 5 years (figure 1). Three-month smoking status was missing for 18 patients, and the percentages of continuing smokers among the 817 patients with available data were 42.6%, 45.2%, 44.5%, 44%, 36.0%, 36.1% and 33.7% at 1 month, 3 months, 1, 2, 3, 4 and 5 years, respectively.
Smoking cessation at 3 months and smoking care

{kind=link}
Evolution of smoking status over time.
Factors associated with smoking cessation
In an univariate model, short delay between wake up and first cigarette smoked, high intake of alcohol consumption, living alone, low level of education, stroke event related to small vessel disease (SVD) and motor and speech disorders symptoms were significantly more frequent in continuers whereas visual symptoms, unsteadiness/vertigo and stroke related to large artery atherosclerosis or from cardioembolic origin were more frequent in quitters. Baseline blood pressure was slightly higher and baseline high density lipoprotein (HDL) level lower in quitters than in continuers. However, in multivariable analysis, only living alone and high alcohol consumption remained significantly associated with continuation (OR for smoking cessation 0.56 (95% CI 0.41 to 0.77) and 0.64 (0.44 to 0.93), respectively), whereas only high education, speech impairment and dyslipidaemia remained associated with quitting (table 3).
Multivariable analysis for factors associated with smoking cessation at 3 months
Major cardiovascular outcome events
After a median follow-up of 5.01 years (IQR 4.84–5.26), stroke, MI or death had occurred in 425 patients, 207 (10.9%) in never smokers, 126 (14.1%) in former smokers, 43 (11.7%) in quitters and 49 (12%) in continuing smokers. After adjustment for age, history of cardiovascular disease and vascular risk factors, blood pressure, low density lipoprotein (LDL) level at 1 year and baseline body mass index, smokers had a higher but not significant risk of a major vascular event at 5 years compared with never smokers, with no difference between continuing and quitting smokers. Regarding secondary outcomes, the risk of MI and vascular death was non-significantly decreased in quitters in comparison to continuers but not the risk of stroke. All individual components of the primary outcomes were non-significantly higher in patients who were smokers at baseline in comparison to non-smokers with no difference between quitters and continuers, except for MI that was significantly lower in quitters (table 4). Similar results were found when analysis was restricted to patients with cerebrovascular events related to either SVD, large artery atherosclerosis, cardiac causes or to other causes (online supplemental file). There were significantly more non-vascular deaths in smokers, quitters and continuers than in non-smokers (table 4).
Adjusted HR and sub-HR for primary and secondary outcomes in overall population
Using time-varying analysis, current smoking at the time of event was associated with a non-significant higher risk of major cardiovascular events (HR 1.31 (95% CI 0.97 to 1.78); p=0.080).
Discussion
In our study, we found that 45.2% of smokers at the time of the qualifying TIA or minor ischaemic stroke event continued to smoke 3 months after, that abstinence at 1 month was a strong predictor of long-term smoking cessation, and that beyond this period the probability of quitting was much lower. The qualifying stroke event seems to act as a ‘wake up call’ that leads to a reappraisal of health values but that quickly fades as previously reported by others.17 20 Further studies are required to assess if acute stroke period is effectively a teachable moment to act as a catalyst for quitting.
As previously reported,15 20 21 28–30 smoking cessation remains a major therapeutic challenge in patients who had a stroke. In our international prospective registry, patients who had a minor stroke or TIA were followed up during 5 years by stroke specialists that are especially concerned about the management of vascular risk factors. As a result, patients were particularly well treated for the duration of the study. At 5 years, mean LDL cholesterol was 92 mg/dL (2.38 mmol/L), 66% of the patients had LDL <1 g/dL and 63.9% had lipid-lowering therapy; mean blood pressure was 132/77 mm Hg, 93% of the patients had blood pressure <140/90 mm Hg, 70.5% had blood-pressure lowering therapy, 71.1% antiplatelet therapy and 17.0% anticoagulant therapy (online supplemental figure 2). Despite this apparent risk factor optimal control, one can be disappointed by the low level of attention paid to smoking cessation. Indeed, only 35.8% of patients had healthcare counselling to stop smoking and only 12.5% received smoking cessation pharmacotherapy.
Given the serious consequences of smoking continuation in stroke survivors, identifying patients most in need of help is important in order to strengthen smoking cessation support. We hypothesised that the wake-up effect might depend on the intensity of the stroke experience: the more disabling the deficit, the more it might lead to smoking cessation. We found that aphasia was associated with an increased chance of smoking cessation, whereas sensory or visual symptoms, which could be probably less distressing, had no impact. However, the association between transient language disturbance and smoking cessation may be more complex due to the insula’s involvement in both smoking addiction31 and language articulation.32 It is possible that aphasia was only a confounding factor and that the association observed was the consequence of a lesion of the insula. Conversely, the presence of motor deficits, longer duration of symptoms and presence of acute cerebral infarction on brain MRI, usually considered as alarming symptoms, was not associated with quitting. As motor deficits include a large range of handicap experiences (eg, partial to complete weakness, hand paresis to hemiplegia), it is possible that among patients with motor deficits, some had small deficits and a positive effect has been missed. Socioeconomic conditions play a role in smoking habits18 21; in our study, we confirmed that living alone, low level of education and alcohol abuse are important factors associated with persistent smoking after stroke. Previous studies have noted variable effects of age and sex15 20 on the subject. However, in our population, age and sex did not have any impact. Good health behaviour markers, such as previous influenza vaccination and regular physical activity, were not predictors of smoking cessation. Similarly, past smoking-related diseases (cardiac or peripheral artery disease or stroke) and vascular risk factors, except for those with dyslipidaemia, were not predictors of smoking cessation. Reasons for this association were not clear and could be due to chance. Nicotine dependence is a major factor predicting long-term cessation in smokers.22 In our cohort, this association was not significant after adjustment. However, it is important to exercise caution as information on the Fagerström test was missing in 65% of cases.
As previously mentioned, our study highlights the lack of sufficient healthcare professional support for smoking cessation in patients with TIA. While both physician advice and pharmacotherapy have been shown to be effective in smoking cessation,16 our study found that only 1 out of 10 smokers were prescribed smoking cessation pharmacotherapy, compared with 90% who were treated with antiplatelet agents, 16% with anticoagulants, 70% with antihypertensive agents and lipid-lowering therapies. These findings suggest a need for a paradigm shift among stroke physicians in their approach to education about smoking cessation. The findings also emphasise the importance of creating fast track access to specialised smoking cessation facilities for patients who had a stroke. The performance of patients in smoking cessation should also be now mandatorily and systematically reported in clinical trials and registries along with achieved blood pressure, lipid and glycated haemoglobin (HbA1c) levels and weight.
Unlike previous observational studies,7 8 10–12 we found that smoking cessation was not associated with a decrease in the 5-year risk of major cardiovascular events compared with patients who continue to smoke, this risk remaining higher in patients who were smokers at baseline than in those who never smoked. The same result was found with a time-based analysis, or when we restricted the analysis to aetiological stroke subtypes that are associated with smoking such as atherosclerosis or SVD, or in patients with recent ischaemic stroke on brain imaging, excluding patients with possible TIA mimics (online supplemental figure 3). However, these subgroup analyses should be taken with caution considering the small sample size. Importantly, the rate of patients with antithrombotic treatment, blood pressure <140/90 mm Hg was similar in continuers, quitters, never and former smokers. Only LDL level control was less satisfactory in continuers as in the other smoking groups, especially in the first 3 years (online supplemental figure 2).
These results could have several explanations. First, we cannot exclude that the effect of smoking cessation could have been underestimated. Indeed, tobacco abstinence was self-reported and not objectively confirmed by CO2 measurement of expired air carbon monoxide or dosage of cotinine in saliva. This is an important issue as the rate of misreporting smoking cessation could be as high as 40%,33 especially in patients with smoking-related conditions.34 Second, it is possible that the benefit of smoking cessation on the occurrence of major vascular events may be less significant in a population where vascular risk factors are well controlled. The impact of smoking on vascular risk could have been less important in our cohort as the rate of baseline current smokers was relatively low. Compared with a recent Chinese study that found a positive effect of smoking cessation on stroke recurrence after a median follow-up of 2.4 years, smoking rate at baseline in our cohort was twice as low.11 It is also plausible that the positive effect of smoking cessation could take more time to be observed as a non-significant reduction of MI and vascular death was observed in quitters, and also of stroke in non-smokers and former smokers. Third, as smoking status was determined 3 months after the qualifying event, we were unable to assess the effect of smoking cessation before this period when the risk of ischaemic stroke is highest. Fourth, as quitters often compensate for their addiction by eating more, which can lead to weight gain, it is possible that the benefit of quitting was outweighed by a consequent weight gain (with the corollary of increased insulin resistance and inflammation). However, a large community-based cohort study found that weight gain occurring after smoking cessation did not modify the association observed between smoking cessation and lower risk of cardiovascular events.35 Fifth, it is possible that factors beyond quitting cigarettes, such as inflammation, should be taken into consideration. Ongoing trials investigating inflammation after stroke may provide insight into this important factor, including its effects on smokers. Finally, we cannot ascertained that the number of patients lost to follow-up, however small, has affected our results.
Conclusion
In our study, smoking cessation interventions by stroke specialists in smokers with recent TIA or minor stroke were very low and the rate of smoking remains high. Most of the patients who stopped smoking did so during the first month post stroke. Surprisingly, no significant association was observed between smoking abstinence and the risk of MACE at 5 years. Despite this and considering the global devastating of smoking, considerable effort needs to be made to educate stroke specialists to help patients quit smoking.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Ethics Committee(s) or Institutional Board(s) has been contacted in each country that required an authorisation for this kind of prospective registry. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors All authors: substantial contributions to the conception and design of the work and interpretation of data for the work; draft the work; final approval of the version to be published; agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. PL is the guarantor of the paper.
Funding Supported by an unrestricted grant from Sanofi and Bristol-Myers Squibb. The funders had no involvement in the study design, the collection, the analysis and interpretation of the data; in the writing of the report; and in the decision to submit the paper for publication.
Competing interests PL has nothing to disclose. PA reports receipt of research grant support from Pfizer, Sanofi, Bristol-Myers-Squibb, AstraZeneca, Boston Scientific, AltheraPharmaceutical, and from the French government, and consulting fees from Pfizer, BMS, AstraZeneca, Johnson and Johnson, Kowa, Amgen, and lecture fees from Amgen, Pfizer, Sanofi. P-JT reports royalties from IP in IMT Company and is a stockholder in IMT. GWA reports equity interest: iSchemaView, and consultant fees from Medtronic, iSchemaView, Janssen, and Biogen. GAD reports unrestricted research grant from Sanofi, speaker and advisory board fees from Boehringer Ingelheim, Bristol Myer Squibb, Pfizer and Bayer companies. JMF reports having received fees as speakers bureau from Boehringer-Ingelheim, consultant fees from GSK, Ferrer and Servier. PGS discloses the following relationships: research grants: Amarin, AstraZeneca, Bayer, Sanofi, and Servier Clinical Trials (Steering committee, CEC, DSMB): Amarin, AstraZeneca, Bayer, Bristol-Myers Squibb, Idorsia, Janssen, Novartis, PhaseBio, Pfizer, Sanofi, Servier Consulting or speaking: Amarin, Amgen, BMS, Novo-Nordisk, Regeneron Senior Associate Editor at Circulation Bayer, Boehringer-Ingelheim, BristolMyersSquibb, Idorsia, Mylan, NovoNordisk, Novartis, Pfizer, Regeneron, Sanofi, Servier. HC has nothing to disclose. JL has nothing to disclose. MGH has nothing to disclose. SU reports receipt of research grants, consultancy fees, and lecture fees from Sanofi, Bayer, Otsuka, Boehringer-Ingelheim, and Daiichi-Sankyo, and research grants from the Japanese Ministry of Health, Labour, and Welfare and Japan Cardiovascular Research Foundation. EV reports Consulting/speaking honoraria from Abbott, Amgen, BMS, Fresenius, GSK, Medtronic, Pfizer, Sanofi, Stallergenes. LKSW reports honoraria as a member of a steering committee for Johnson & Johnson, Astra Zeneca and Bayer; honoraria for participation in clinical trials, contributions to advisory boards, or oral presentations from Bayer, Sanofi-Aventis, Bristol-Myers Squibb, Boehringer Ingelheim, and Pfizer. CAM serves in the Steering Committee of CLOTBUST-ER trial (Cerevast); SOCRATES (AstraZeneca), IMPACT-24b (Brainsgate), REVASCAT (Fundació Ictus Malaltia Vascular). He has received honoraria for participation in clinical trials, contribution to advisory boards or oral presentations from: Astra Zeneca: Boeringher Ingelheim, Daichii Sankyo, BMS, Covidien, Cerevast, Brainsgate. CAM has no ownership interest and does not own stocks of any pharmaceutical or medical device company. PR has received Advisory Board fees from Pfizer, Sanofi, Bristol-Myers-Squibb, AstraZeneca, Boehringer-Ingelheim, Bayer and Daiichi-Sankyo.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.