Article Text

Abstract
Objectives This study aimed to evaluate the effectiveness of the Trauma Rating Index in Age, Glasgow Coma Scale, Respiratory rate and Systolic blood pressure score (TRIAGES) in predicting 24-hour in-hospital mortality among patients aged 65 years and older with isolated traumatic brain injury (TBI).
Design A retrospective, single-centre cohort study.
Setting This study was conducted at a government-run tertiary comprehensive hospital.
Participants This study included 982 patients aged 65 years or older with isolated TBI, who were admitted to the emergency department between 1 January 2020 and 31 December 2021.
Interventions None.
Primary outcome 24-hour in-hospital mortality was the primary outcome.
Results Among the 982 patients, 8.75% died within 24 hours of admission. The non-survivors typically had higher TRIAGES and lower GCS scores. Logistic regression showed significant associations of both TRIAGES and GCS with mortality; the adjusted ORs were 1.98 (95% CI 1.74 to 2.25) for TRIAGES and 0.72 (95% CI 0.68 to 0.77) for GCS. Receiver operating characteristic (ROC) analysis indicated an area under the ROC curve of 0.86 for GCS and 0.88 for TRIAGES, with a significant difference (p=0.012). However, precision–recall curve (PRC) analysis revealed an area under the PRC of 0.38 for GCS and 0.47 for TRIAGES, without a significant difference (p=0.107).
Conclusions The TRIAGES system is a promising tool for predicting 24-hour in-hospital mortality in older patients with TBI, demonstrating comparable or slightly superior efficacy to the GCS. Further multicentre studies are recommended for validation.
- ACCIDENT & EMERGENCY MEDICINE
- TRAUMA MANAGEMENT
- Neurological injury
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
To our best knowledge, this is a pioneering investigation into the TRIAGES (Trauma Rating Index in Age, Glasgow Coma Scale, Respiratory rate and Systolic blood pressure score) system’s prognostic value specifically for older patients with isolated traumatic brain injury.
To enhance the efficiency of early triage, it is important to prioritise early decision-making and use trauma scoring systems in a rational manner.
The retrospective design of the study introduces inherent biases and limits the ability to establish causal relationships.
The study’s focus on a single-centre cohort may limit the generalisability of the results to more diverse healthcare settings.
Introduction
Traumatic brain injury (TBI) represents a considerable public health challenge worldwide, particularly within the older population. These injuries frequently result in severe neurological deficits, markedly increasing morbidity and mortality rates in this demographic.1 The vulnerability of older patients to TBI, exacerbated by their often suboptimal recovery outcomes and reduced post-injury quality of life, significantly differs from the recovery trajectories observed in younger patients.2 This disparity is attributable to various factors, including the presence of comorbid health conditions, heightened susceptibility to trauma and reduced physiological resilience in older individuals.3
The importance of prompt and precise triage for older patients with isolated TBI cannot be overemphasised. Effective triage facilitates rapid referral to specialised trauma centres for immediate intervention.4 Accurately predicting outcomes in these patients is crucial, as it assists clinicians in developing the most appropriate therapeutic strategies.5 An ideal prehospital trauma triage tool should be simple to use and capable of accurately assessing the severity of injuries. While the Glasgow Coma Scale (GCS) has been a longstanding tool for evaluating TBI, it falls short of addressing the specific challenges presented by older patients with isolated TBI.6
Addressing these challenges, the Trauma Rating Index in Age, Glasgow Coma Scale, Respiratory rate and Systolic blood pressure score (TRIAGES), designed initially for general trauma cases, has gained prominence. This system integrates variables such as age, systolic blood pressure, respiratory rate and the GCS to provide a comprehensive bedside evaluation tool.7 Our recent studies have shown that TRIAGES matches the predictive ability of the GCS in terms of short-term outcomes.8 Moreover, our subgroup analysis indicates that TRIAGES may surpass the GCS regarding area under the receiver operating characteristic (AUROC), though this difference did not achieve statistical significance.8
Building upon this groundwork, the present study aimed to evaluate the efficacy of the TRIAGES system in prognostic assessments for older patients with isolated TBI. Through a retrospective analysis of medical records, our focus was on predicting 24-hour mortality. Our objective is to address a significant gap in the existing literature by examining the predictive value of TRIAGES for short-term mortality in this population. The implications of our findings could significantly influence clinical decision-making, paving the way for a more refined and accurate approach to prognosis and thereby enhancing the overall quality of patient care.
Methods
Population and study design
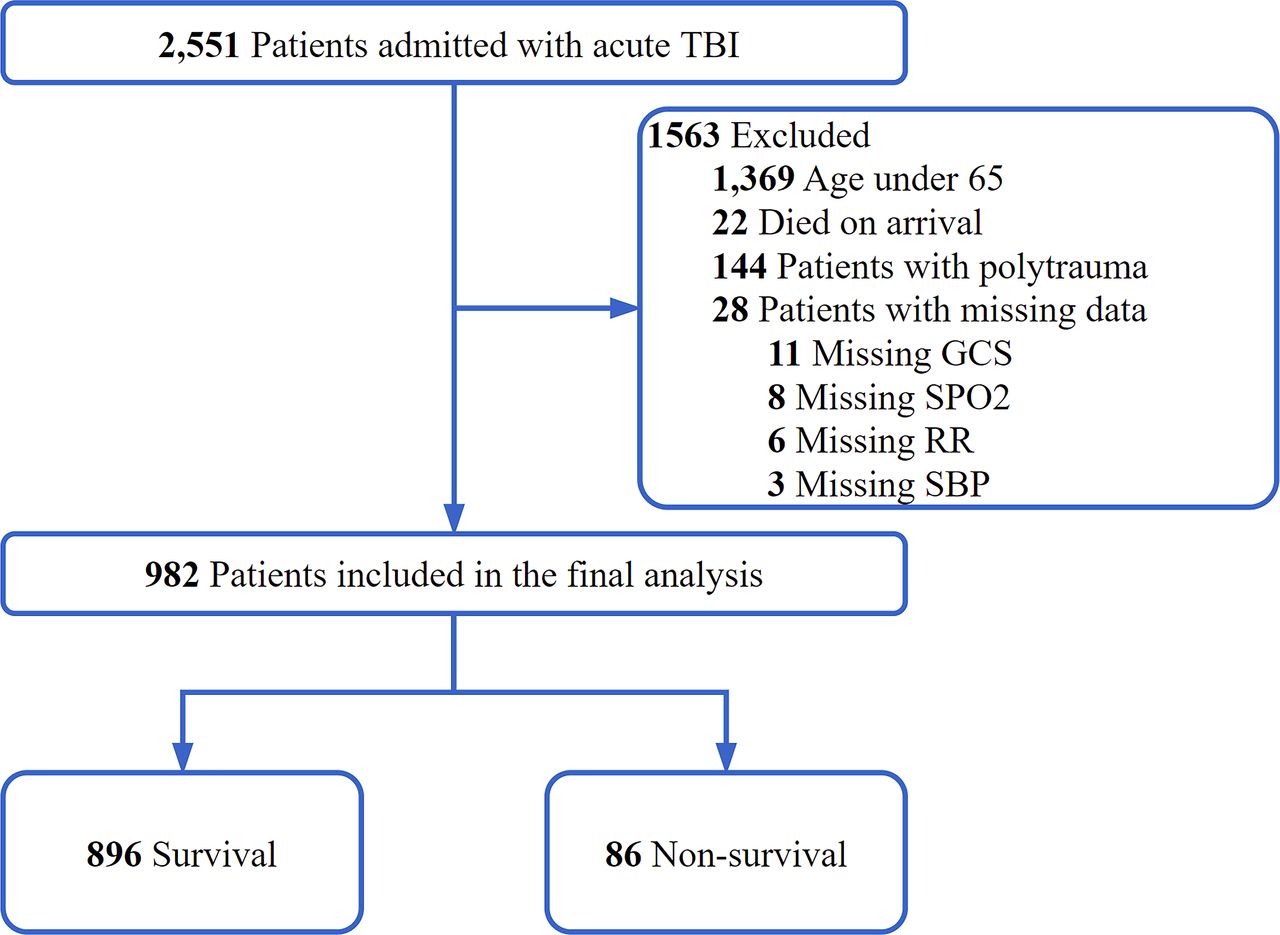
This retrospective single-centre cohort study entailed a sequential gathering and examination of clinical data from 2271 patients with isolated acute TBI admitted to Nantong University Hospital’s emergency department (ED). The data spanned from 1 January 2020 to 31 December 2021. The study focused on 982 patients aged 65 years and above. Its primary aim was to evaluate the predictive efficacy of the TRIAGES system for 24-hour in-hospital mortality in this cohort.
The hospital in focus is a government-run tertiary comprehensive healthcare centre with a history spanning over 110 years. It is a major medical hub in Eastern China, annually handling over 40 000 trauma cases. The hospital is notably well equipped, boasting a specialised resuscitation room, emergency theatre and emergency intensive care unit, thus providing an ideal environment for trauma care and research.
Data collection and enrolment criteria
We meticulously collected patient data from electronic medical records at the ED admission, including age, gender, heart rate, respiratory rate, systolic blood pressure, diastolic blood pressure, oxygen saturation (SpO2), GCS scores, accident type, medical history of hypertension and diabetes mellitus, and use of anticoagulants. Upon patient admission to the emergency resuscitation room, nurses promptly recorded vital signs and GCS data. The imaging data collection was done in the ED before transferring the patient to the ward. Team members TC and YY verified these data for consistency. ED staff, each with at least 3 years of experience and emergency specialty certifications, continuously monitored patient progress. The study included patients aged 65 years and above. We excluded cases involving admission in a deceased state, incomplete data or multiple injuries (figure 1). The data sourcing occurred through the DoCare Emergency Clinical Information System.

Flow chart of patient enrolment. GCS, Glasgow Coma Scale; RR, respiratory rate; SBP, systolic blood pressure; TBI, traumatic brain injury.
Definitions and endpoints
TBI was defined as trauma identified through CT scans and clinical symptoms. The primary endpoint was 24-hour in-hospital mortality. We computed each subject’s TRIAGES using medical record variables from the database for statistical analysis. Our study concentrated on short-term prognoses and did not include long-term follow-up on patient survival.
Predictive value of the Trauma Rating Index in Age, Glasgow Coma Scale, Respiratory rate and Systolic blood pressure score
The TRIAGES scoring system, intended for initial triage and prognosis prediction in emergency trauma patients,7 incorporates four critical factors: age, GCS score, respiratory rate and systolic blood pressure. This system assigns a score to each variable, ranging from 0 to 14. Online supplemental table 1 provides a detailed breakdown of these scores.
Supplemental material
Statistical analysis
Continuous variables were summarised using medians and IQRs, employing non-parametric techniques to ensure robust comparisons irrespective of data distribution. To assess differences in continuous measurements, we used the Mann-Whitney U test. Categorical variables were expressed as frequencies and percentages, and their comparisons were conducted using either the Χ2 test or Fisher’s exact test.
Logistic regression analysis assessed the association between TRIAGES and GCS scores and 24-hour mortality. To mitigate confounding influences, we meticulously tailored the adjusted model. For TRIAGES, adjustments were made for factors not covered in the score: sex, heart rate, diastolic blood pressure, SpO2, hypertension, diabetes mellitus and anticoagulant use. The GCS model additionally accounted for age, respiratory rate and systolic blood pressure. We used restricted cubic splines (RCS) with five knots, corresponding to the 5th, 35th, 50th, 65th and 95th percentiles, to explore the relationship between each component of TRIAGES and outcome.
To evaluate the effectiveness of TRIAGES and GCS scores in discriminating between survivors and non-survivors, we employed receiver operating characteristic. Considering the potential imbalance due to the infrequent occurrence of mortality, we also performed a precision–recall curve (PRC) analysis. The overall predictive accuracy was determined by calculating the AUROC and the area under the PRC (AUPRC). We employed a non-parametric bootstrap method with N=1000 bootstrap samples to estimate the distribution of the AUROC and AUPRC.
Data analysis used Python V.3.8.10 (with SciPy V.1.7.1 and sci-kit-learn V.0.24.2), R (http://www.R-project.org, The R Foundation) and Free Statistics Software (V.1.9). Statistical significance was set at p<0.05 for two-tailed tests. The reporting of this study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.9
Results
Baseline characteristics
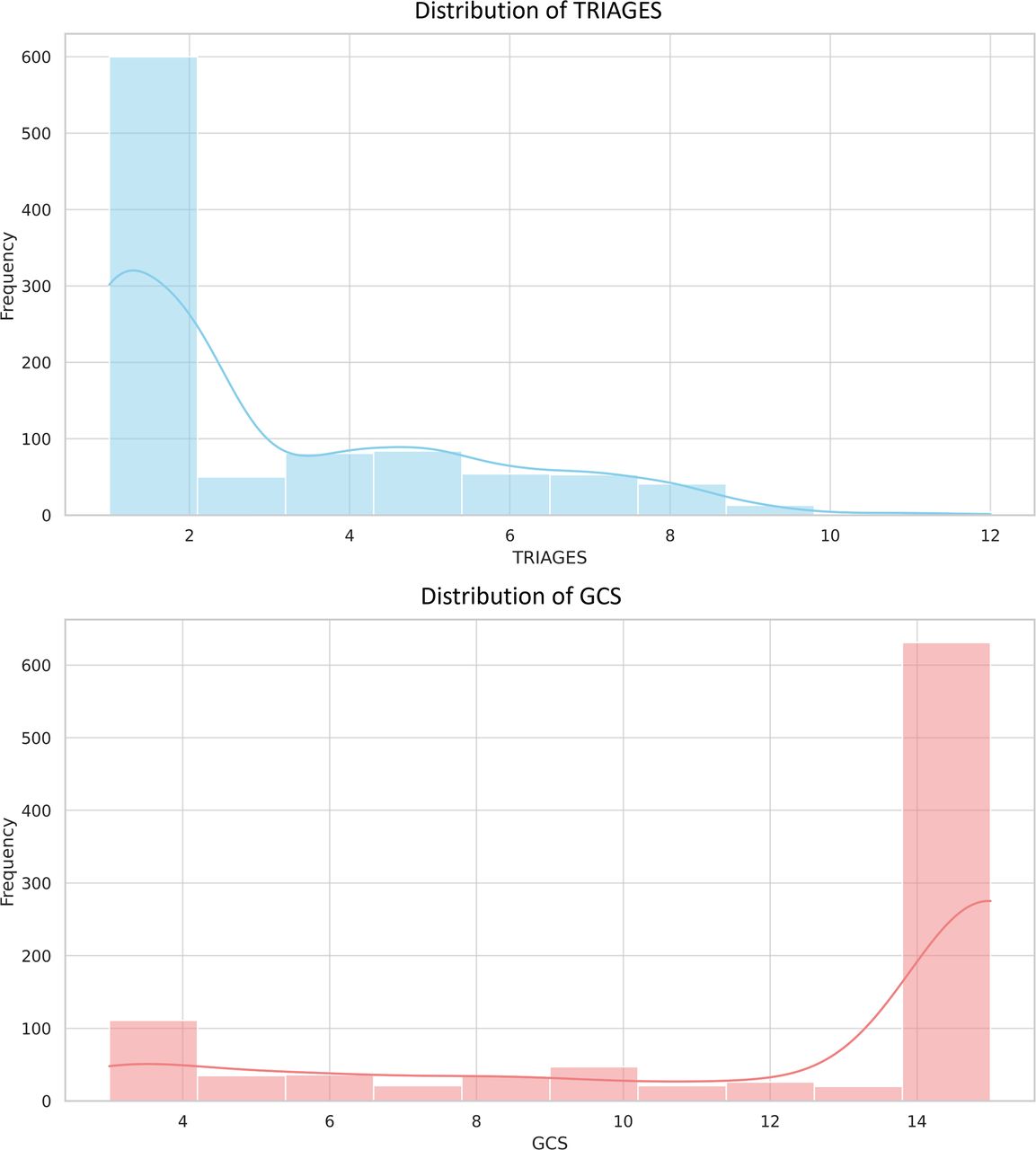
A total of 982 patients, all transported via ground ambulance, were included in the analysis. Among them, 86 patients (8.75%) experienced mortality within 24 hours of admission. A comparison between the survival and non-survival groups revealed several notable differences. Non-survivors more frequently used anticoagulants (p<0.001), had lower systolic blood pressure (p=0.042), reduced SpO2 (p<0.001) and more occurrences of occipital lobe (p=0.018) and subarachnoid haemorrhages (p=0.046). Furthermore, the non-survival group displayed higher TRIAGES and lower GCS scores than the survival group (p<0.001 for both). The distribution of TRIAGES and GCS scores among the study population is illustrated in figure 2. No statistically significant differences were observed between the two groups regarding other examined characteristics (table 1).

Distribution of TRIAGES and GCS. The histogram reveals the prevalence of different TRIAGES (blue) and GCS (red) levels. The smooth line overlaid on the histogram represents a kernel density estimation, offering a continuous probability density curve of the TRIAGES (blue) and GCS (red). GCS, Glasgow Coma Scale; TRIAGES, Trauma Rating Index in Age, Glasgow Coma Scale, Respiratory rate and Systolic blood pressure score.
Clinical characteristics of survival and non-survival groups
Associations between TRIAGES and GCS and 24-hour mortality
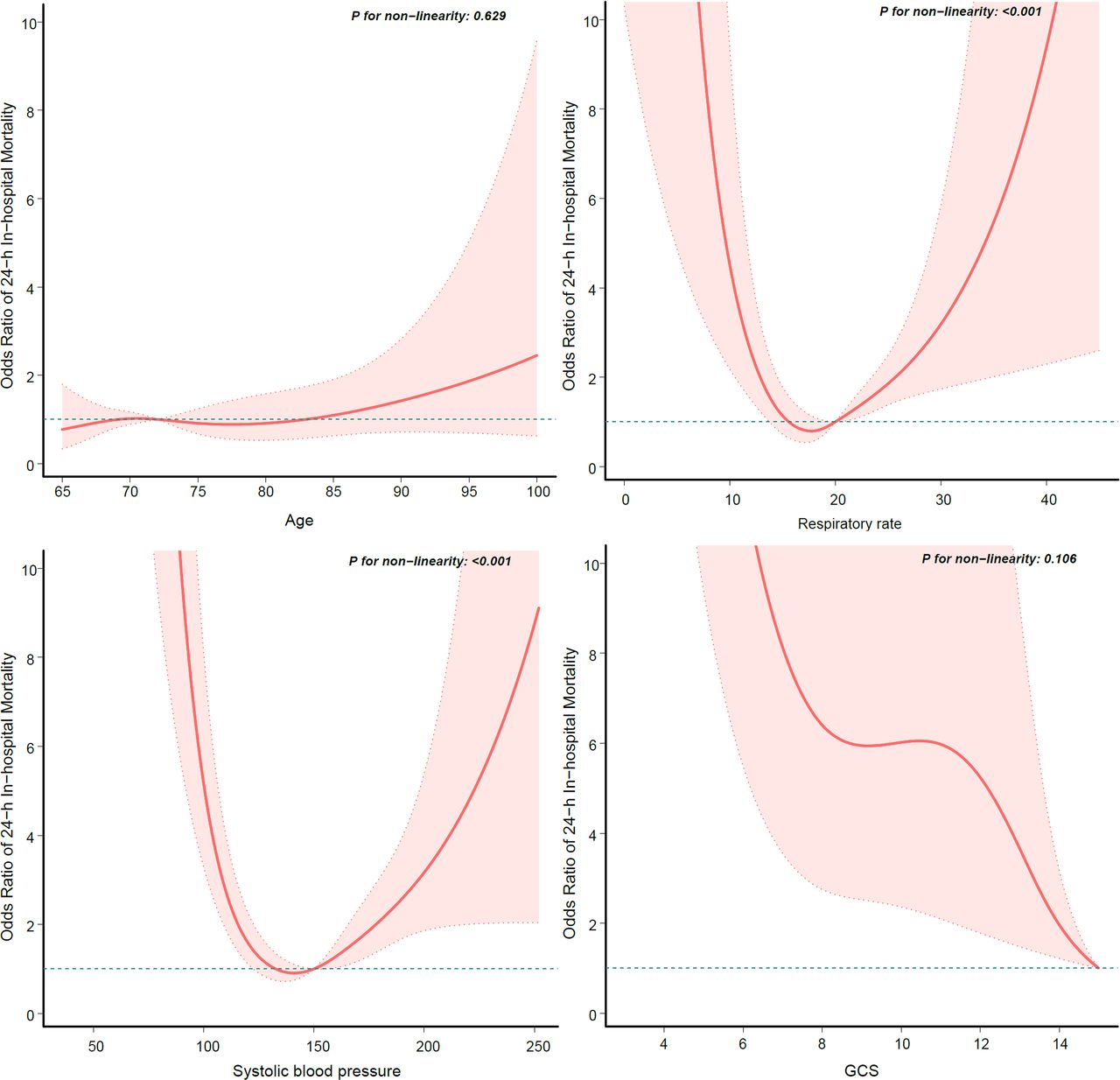
The RCS curve analysis demonstrated the OR of 24-hour in-hospital mortality in elderly patients with TBI for each TRIAGES component variable. The results revealed a linear association of age and GCS scores with short-term poor prognosis. In contrast, systolic blood pressure and respiratory rate displayed a U-shaped, non-linear relationship with short-term prognosis (figure 3).

Restricted cubic spline curves for TRIAGES component variables. This figure comprises four subplots, each depicting the non-linear relationship between a key component of the TRIAGES score and mortality. GCS, Glasgow Coma Scale; TRIAGES, Trauma Rating Index in Age, Glasgow Coma Scale, Respiratory rate and Systolic blood pressure score.
The crude and adjusted ORs for TRIAGES were 1.96 (95% CI 1.74 to 2.21) and 1.98 (95% CI 1.74 to 2.25), respectively. The crude and adjusted ORs for GCS were 0.73 (95% CI 0.69 to 0.77) and 0.72 (95% CI 0.68 to 0.77), respectively (table 2).
Logistic regression model with 24-hour mortality
Predictive value of TRIAGES and GCS for 24-hour mortality
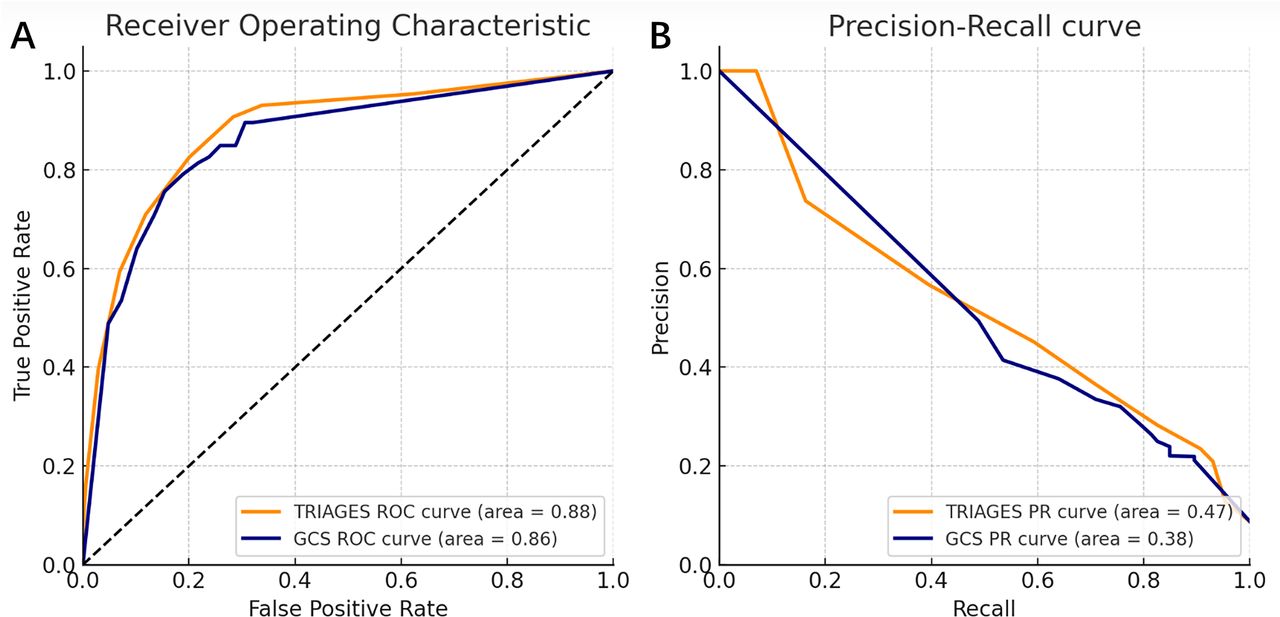
The AUROC for GCS was 0.86, while for TRIAGES, it was 0.88. A bootstrap resampling method revealed a statistically significant difference between the two scores with a 95% CI for the difference ranging from 0.0028 to 0.0415 (p=0.012) (table 3 and figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Performance evaluation of predictive models using receiver operating characteristic (ROC) and precision–recall curve (PRC). (A) ROC curve: the diagonal dashed line represents a no-discrimination classifier. The yellow line is the ROC curve for TRIAGES, and the blue line is the ROC curve for GCS. (B) PRC: The area under the PRC indicates the model’s performance in terms of precision and recall across different decision boundaries, which is especially valuable when dealing with imbalanced datasets. The yellow line is the ROC curve for TRIAGES, and the blue line is the ROC curve for GCS. GCS, Glasgow Coma Scale; TRIAGES, Trauma Rating Index in Age, Glasgow Coma Scale, Respiratory rate and Systolic blood pressure score.
Predictive value of TRIAGES and GCS for 24-hour mortality
Given the potential class imbalance with the rare event of death, a PRC analysis was also conducted. The AUPRC for GCS was 0.38, and for TRIAGES, it was 0.47. Although TRIAGES exhibited a higher AUPRC value, a bootstrap analysis showed that the difference between AUPRC was not statistically significant (p=0.107) (table 3 and figure 4).
Discussion
Our results indicate that TRIAGES effectively predicts short-term adverse outcomes in elderly patients with isolated TBI. This discovery holds considerable clinical importance, as it assists ED physicians in rapidly assessing older patients with TBI, directly influencing their prognosis.
Prognostic prediction in TBI remains a highly debated topic in the academic discourse. The GCS has traditionally served as a primary risk assessment tool for patients with TBI.10 Given its widespread use as a measure of neurological status, various trauma scoring systems, including TRIAGES, have incorporated the GCS into their algorithms. Moreover, modified versions of the GCS, like the GCS-P, exhibit enhanced predictive accuracy for TBI prognosis.11 12 Recent studies employing machine learning-based prognostic models for TBI identify GCS motor scores as reliable predictive indicators.13 In our prior study, we also observed that the GCS exhibited good predictive power, with a slightly higher AUROC than TRIAGES. This finding emphasises the essential role of the GCS in the TRIAGES scoring system. However, despite TRIAGES considering additional factors beyond the GCS, our analysis did not reveal significant improvements in predictive performance.8 This further underscores the importance of the GCS as a critical prognostic factor in patients with TBI, deserving heightened attention during triage assessments. However, it is essential to acknowledge its limitations due to confounding factors such as pharmacological sedation, paralysis, tracheal intubation and intoxication.14 15 In our present investigation, TRIAGES and GCS demonstrated favourable predictive capabilities for short-term prognosis. Notably, we observed a statistically significant difference in AUROC between TRIAGES and GCS, with TRIAGES exhibiting a higher AUROC, confirming our previous hypothesis.
Mortality rates in TBI cases are profoundly affected by patient age, a trend observed across all levels of injury severity.5 A study conducted in France revealed a notable age-related increase in the mortality rate among patients with TBI, ranging from 15% in the 15–24 age group to a substantial 71% in those aged 85 years and older.16 Our recent study observed a similar pattern, where the mortality rate among older individuals (8.75%) slightly exceeded that of the overall population in the previous study (7.53%).8 A parallel finding was observed in the study of the Base deficit, International normalized ratio, and Glasgow Coma Scale (BIG) scores, where integrating an age-adjusted BIG model significantly improved the predictive accuracy for TBI prognosis.17 In a study on machine learning of prediction models for patients with TBI, age was similarly considered a significant predictor.13 This phenomenon could be attributed to the more significant brain atrophy and intracranial space observed in older individuals, rendering them more vulnerable to intracranial haemorrhage.18 Interestingly, despite similar levels of intracranial injury severity, older patients often present with higher GCS.19 Consequently, older adults with TBI are frequently assigned higher grading levels, even when experiencing relatively minor trauma and presenting with higher GCS scores upon arrival at the ED.20 These observations highlight the potential limitations of relying solely on GCS assessments for older patients with TBI, as age has been recognised as a significant variable influencing the prognosis of patients with TBI in various predictive models.21
We further evaluated our models using the PRC analysis in the present study. PRC, which focuses exclusively on the positive class, is particularly insightful for imbalanced datasets.22 The higher AUPRC for TRIAGES underscores its superior performance in terms of precision and recall, although the difference was not statistically significant when compared with GCS. It is noteworthy that TRIAGES, despite its comprehensive nature, did not demonstrate a significant advantage over the GCS in our study. Several factors may have contributed to this outcome. First, our cohort’s small proportion of abnormal respiratory rates and systolic blood pressure values may have limited TRIAGES’ advantage over the entire assessment. Second, despite including the GCS in TRIAGES, it has been categorised, which may have affected the GCS effectiveness prediction compared with continuous variables.
Strengths and limitations
The primary strength of our study lies in its pioneering investigation into the prognostic value of the TRIAGES scoring system, specifically among older patients with TBI. However, we must admit that our study has several limitations. First, while valuable for our investigation, the retrospective design inherently introduces biases and precludes the establishment of causal relationships. Future studies could employ prospective designs with predefined criteria, offering more robust insights into causal relationships. Second, our study’s exclusive focus on a single-centre cohort may restrict the generalisability of our results to more comprehensive healthcare settings. This limitation calls for prudence when applying our findings to diverse patient populations. Collaborative multicentre investigations could address this limitation by providing more comprehensive and representative data. Third, our study only evaluated short-term outcomes, limiting our ability to assess long-term recovery trajectories among older patients with TBI. Future studies with extended follow-up periods could provide a more comprehensive understanding of prognosis. Lastly, our study employed specific exclusion criteria that may have influenced the composition of our sample. Conducting sensitivity analyses or relaxing these criteria in future research can enhance our findings’ robustness and applicability to broader patient groups. These limitations, while inherent, provide valuable avenues for future research to refine predictive models for older patients with TBI, enhancing their clinical validity and relevance.
Conclusion
In summary, our research indicates that the TRIAGES scoring system could be an effective predictor of short-term mortality in older patients with isolated TBI, demonstrating predictive accuracy comparable with GCS. However, to further validate TRIAGES’ predictive capability for both short-term and long-term prognoses in this patient group, prospective, well-designed multicentre studies are essential.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Our study received approval from the Research Ethics Committee of the Affiliated Hospital of Nantong University, with the approval number 2021-K084-01. The committee waived the need for participant consent, as the research solely employed observational methods without any interventions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DJ and TC contributed equally.
Contributors DJ and TC contributed equally to this paper. DJ—writing (original draft), software, methodology, formal analysis and conceptualisation. TC and YY—validation, resources, investigation and data curation. XY—writing (review and editing). YS—writing (review and editing) and supervision. ZH—supervision and project administration and takes full responsibility for the work and the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.