Article Text

Abstract
Background Following the COVID-19 pandemic, there was an increase in teenage pregnancies nationally, however, limited data exists regarding the same among girls living in refugee settlements.
Objectives We evaluated the prevalence of teenage pregnancy and associated factors in Palorinya and Bidi Bidi refugee settlements in Obongi and Yumbe districts of northern Uganda, in the post-COVID-19 era.
Design We conducted a cross-sectional study.
Setting Refugee settlements in northern Uganda.
Participants We included 385 teenage girls aged 15–19 years.
Methods We used convenience sampling techniques between March and May 2023. Prevalence of teenage pregnancy was assessed by self-reported pregnancies between January 2020 and May 2023 among participants. We conducted Pearson’s χ2 and Fisher’s exact tests for bivariate analysis. All variables with a p value<0.2 at bivariate analysis were included in multivariable regression. We applied a modified Poisson regression model at the multivariable level to evaluate independent associations. The level of statistical significance was set at p<0.05.
Primary and secondary outcome measures The primary outcome measure was the prevalence of teenage pregnancy, assessed through self-reported pregnancies among participants. Secondary outcome measures included factors associated with teenage pregnancy, such as living with a husband, lack of formal education, peer pressure and history of sexual abuse.
Results Overall, the mean age was 17 (IQR: 15–18), and sexual debut was at 16 (IQR: 15–17) years. Lifetime modern contraceptive use was 13.8% (n=53/385) and current use was 7.5% (n=29/385). Teenage pregnancy period prevalence was 34.0% (CI: 29.4% to 38.9%). Factors independently associated with teenage pregnancy were: living with a husband (aPR: 3.8, 95% CI: 2.51 to 5.84, p<0.001), lack of formal education (Adjusted Prevalence Ratios - aPR: 2.3, 95% CI: 1.26 to 4.35, p=0.007), peer pressure (aPR: 2.1, 95% CI: 1.54 to 2.86, p<0.001) and history of sexual abuse (aPR: 1.5, 95% CI: 1.07 to 1.99, p=0.018).
Conclusion Our study revealed that around 1 in 3 adolescent girls in northern Uganda’s refugee settlements experienced pregnancy during the COVID-19 pandemic, with only 1 in 13 currently using modern contraceptives. To address this, targeted strategies by relevant authorities are crucial, including legal actions against sexual abuse, promoting girl child education and enhancing access to long-term contraception to reduce teenage pregnancy and associated health risks in these settings.
- Adolescents
- Pregnancy
- Cross-Sectional Studies
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study’s inclusion of only two refugee settlements may limit generalisability to all refugee settlements in Uganda, affecting external validity.
Randomly selecting settlements and using a substantial sample size within each strengthens the statistical reliability of our conclusions.
Conducting a cross-sectional analysis without pre-pandemic data prevents establishing causal relationships between variables.
Future research could adopt longitudinal approaches to track changes over time and incorporate historical data for a comprehensive assessment of causal associations.
Background
Teenage pregnancy is defined as a pregnancy in girls 13–19 years of age.1 Teenage pregnancies can have negative consequences for the mother’s health such as unsafe abortion attempts leading to mortality, as well as economic and social outcomes, exacerbated by stigmatisation, school dropout and isolation from family.2 Complications from teenage pregnancy and childbirth are the leading cause of death in girls aged 15–19 years worldwide.3
The incidence of teenage pregnancy is increasing and has become a worldwide concern. It is estimated that about 16 million girls 15–19 years old give birth each year, contributing to nearly 11% of all births worldwide.1 Globally, in 2022, an estimated 13% of adolescent girls and young women gave birth before the age of 184 5
In Africa, more than 20% of women aged 15–19 have given birth to at least one child.1 Sub-Saharan Africa (SSA) is home to more than one million teenage girls with pregnancy.5 SSA additionally experiences some of the highest rates of gender inequality in the world, resulting in unequal access to education and high rates of violence against girls, early pregnancy and child marriage.6 It is estimated that 608 000 girls are thought to be at risk of child marriage and 542 000 additional girls are at risk of early pregnancy.7
The regional teenage birth rate in SSA is more than double the global average, with 101 births per 1000 girls aged 15–19; ranging from 39 births per 1000 girls aged 15–19 in Rwanda to 184 births per 1000 girls aged 15–19 in Nigeria.4 Child marriage is widespread in West and Central Africa, where 42% of women are married as children, and in East and Southern Africa, where child marriage affects 37% of girls.8
Despite Uganda’s commitment to ending child, early and forced marriages and teenage pregnancy by the year 2030 through co-sponsoring the 2013 and 2014 UN General Assembly and 2013 Human Rights Council resolutions on early and forced marriages,9 one in four (24%) teenage girls in Uganda report having given birth for the first time by the age of 18.10 According to UNICEF (2021) estimates, a total of 354 736 teenage pregnancies were registered in 2020 and 196 499 in the first 6 months of 2021 amidst the COVID-19 pandemic.11
The COVID-19 pandemic wreaked unprecedented havoc on children, families and communities around the globe, disrupting vital services like girl-child education and putting millions of lives at risk. The United Nations estimated that nearly 11 million primary and secondary school learners worldwide—5.2 million of whom are girls—did not return to education following school closures amidst COVID-19 due to teenage pregnancy and related outcomes.12
For the most vulnerable children, especially girls living in refugee settlements, accessing education and staying in school are hard enough. The pandemic caused additional, unanticipated disruption, compounding their vulnerability to teenage pregnancies by many folds.7 Moreover, teenage girls living in refugee settlements face challenges accessing sexual and reproductive health services, including sex education and modern contraceptive methods.13 These girls are at a significantly higher risk of early pregnancy, a situation that worsened due to the COVID-19 pandemic. According to a recent study by the Forum for African Women Educationalists (Uganda Chapter), the rate of teenage pregnancy among girls in refugee settlements rose from 3.3% to 4.1% during the pandemic. In one Palabek settlement, the proportion of refugee girls who reported being pregnant during the COVID-19 period reached 4.8%, compared with the national average of 1.8%.13 Additionally, statistics on the uptake of modern contraceptive methods among this population is unknown.
Teen pregnancies in refugee and humanitarian settings are influenced by several factors including poverty, lack of education, cultural norms, etc., further driven by limited access to healthcare, lack of social support and increased risk of sexual violence.13 14 Addressing these issues requires targeted interventions that consider the unique challenges faced by teenage girls in these settings.
We therefore aimed to estimate the prevalence and associated factors of teenage pregnancies in the post-COVID-19 era in Palorinya and Bidi Bidi refugee settlements of the West Nile region, northern Uganda.
Methods
Study design and rationale
We conducted a community-based, cross-sectional study between March and May 2023. We followed the Strengthening The Reporting of Observational Studies in Epidemiology (STROBE) guidelines to design this manuscript in order to ensure attention to detail.14
Study setting and rationale
We conducted this study in Palorinya and Bidi Bidi refugee settlements of the West Nile region, northern Uganda. According to data from the Office of the Prime Minister (OPM) and United Nations Higher Commissioner for Refugees, Uganda is now home to 1 622 738 refugees living in 13 refugee settlements across the country, and almost half (6) of these are in the west Nile region.15 Women and girls constitute over 80% of this population, and the settlements are arranged in blocks and zones. Palorinya refugee settlement has four zones and 9 level three health centres, meanwhile Bidi Bidi has 6 zones and 16 level three health centres. None of the refugee settlements has a higher-level health centre; however, there are several referral sites, for example, Yumbe Health Centre IV, Midigo Health Centre IV and Yumbe Regional Referral Hospital. All these facilities provide family planning services to adolescents. This setting was chosen because it hosts the biggest number of refugee settlements, proposed to provide a big pool of potential respondents for sampling.
Study population, inclusion and exclusion criteria
Our study targeted teenage girls living in the refugee settlements of northern Uganda. We included only respondents between 15 and 19 years old, who provided written informed consent or assent with a consent from parent/guardian, and were living in the refugee settlements before the beginning of COVID-19. Those who did not provide informed consent or assent were not included.
Sample size determination
We used the Kish Lisle (1965) formula for the calculation of sample size for an unknown population. At 95% CI, we used an error of 5%, alpha risk was expressed with a z score of 1.96 and a conservative assumption of a 50% population proportion was made to ensure robustness. We obtained a sample size of 385. These choices were guided by standard practices, aiming to balance precision and practicability.
Sampling method
We used convenience sampling to select study participants from Bidi Bidi and Palorinya refugee settlements. Convenience sampling in our study involved selecting participants who were readily available and willing to participate in the study. We approached individuals in many community spaces, targeting various times and days to ensure diversity. The participation acceptance rate was 100%, with no declines. This method allowed us to gather data from a broad participant base.
Research instruments
We developed a semi-structured questionnaire including both open and closed-ended questions. The data collection tool was developed in English and translated into three languages: Acholi, Kuku and Arabic. We pretested the tool among respondents of similar characteristics outside the study area, after which we refined and fine-tuned the tool for reliability and validity. The tool was then exported into KoboToolbox installed on mobile phone devices which was used for data collection. We asked about demographics, household characteristics, pregnancy history between January 2020 and May 2023 and intentions, marriage status, modern contraceptive use between January 2020 and May 2023, sex education and sexual and physical abuse among others. Abuse was measured by asking ‘Have you ever experienced physical abuse?’ and ‘Have you ever experienced sexual abuse?’ with timeframes specified as ‘in the past 12 months’ and ‘in your lifetime,’ respectively. Contraception use was assessed by asking ‘Have you ever used any form of contraception?’. Those who had ever used were further asked to specify the method of contraception used. Peer pressure was measured by asking ‘Have you ever experienced any form of peer pressure to get pregnant?’ Alcohol consumption was assessed by asking ‘Do you take alcohol?’. These responses were recorded as binary outcomes (yes/no). The tool was developed de novo, adhering to established guidelines and drawing from relevant literature. This tool had not been previously used in this setting, and it was tailored specifically for this study.
Data collection procedures
A private and comfortable room was acquired and used during the process of data collection to ensure a private and confidential environment for respondents. We recruited research assistants, who were given a 1 day training for acquaintance with the tool and were taken through research ethics and good clinical practice. The research assistants carried out the collection of data. Although gender matching between participants and data collectors was not implemented, all research assistants underwent comprehensive training on ethical principles. This training highlighted the importance of maintaining privacy and confidentiality, especially when handling sensitive information related to abuse. They explained the purpose of the study to each of the respondents identified and obtained informed consent, followed by administration of the questionnaire using an electronic form stored in the KoboToolbox mobile application, which is a free open-source tool for mobile data collection.
Data management
The phone devices that were used to collect the data were fully charged at every moment the research team set off to collect data, and the data captured on the phone were regularly saved to avoid loss of data. We safely kept the devices under key and lock before and after data collection, and access was limited. We exported the data into STATA V.15, where analysis was done.
Data analysis
The prevalence of teenage pregnancy was assessed by self-reported pregnancies from January 2020 to May 2023. We conducted Pearson’s χ2 and Fisher’s exact tests for bivariate analysis. The level of statistical significance was set at p<0.05. Variables with a p value<0.2 from these tests were included in the multivariable analysis. We applied a modified Poisson regression model at the multivariable level to evaluate independent associations. The level of statistical significance was set at p<0.05. Modified Poisson regression was chosen over logistic regression because the outcome was common (ie, the prevalence rate was high), because in such cases, the OR from logistic regression can significantly overestimate the relative risk. We considered variables with p<0.2 from bivariate analysis to be included in the multivariable regression since their power of association is ≥ 80%.
The research questions tested in statistical analysis were, ‘what is the prevalence of teenage pregnancies in the study population?’ and ‘what are the associated factors of teenage pregnancies in the study population?’
The data were then computed in percentages and frequencies and finally presented in figures (pie chart, bar graph) and tables.
Patient and public involvement
The public was involved in this study. Dissemination of findings was done to key stakeholders.
Results
Participant characteristics
Table 1 summarises the general characteristics of 385 teenage girls living in refugee settlements of the West Nile region, in northern Uganda. The mean age was 17 (IQR: 15 to 18), years, and 99.5% were Christians, 316 (82.1%) had attained primary education as the highest level, 85.6% were not working, median monthly income was 0 (IQR: 0 to 1000), Uganda shillings, 56.1% did not live with both parents, 54.8% of household heads were women and 22.1% of household leads were husband/spouse.
Individual characteristics of 385 teenage girls living in Palorinya and Bidi Bidi refugee settlements of West Nile region, northern Uganda
Overall, 178 (46.2%) were sexually active, the mean age of sex debut was 15.8 (SD: 1.44) years and sexual abuse was reported by 5.2% of respondents, of whom 75% were sexually abused by strangers; meanwhile, physical abuse was reported by 21.6% of respondents, 37.1% of teenage girls experienced peer pressure and alcohol consumption was reported by 8.8% of respondents.
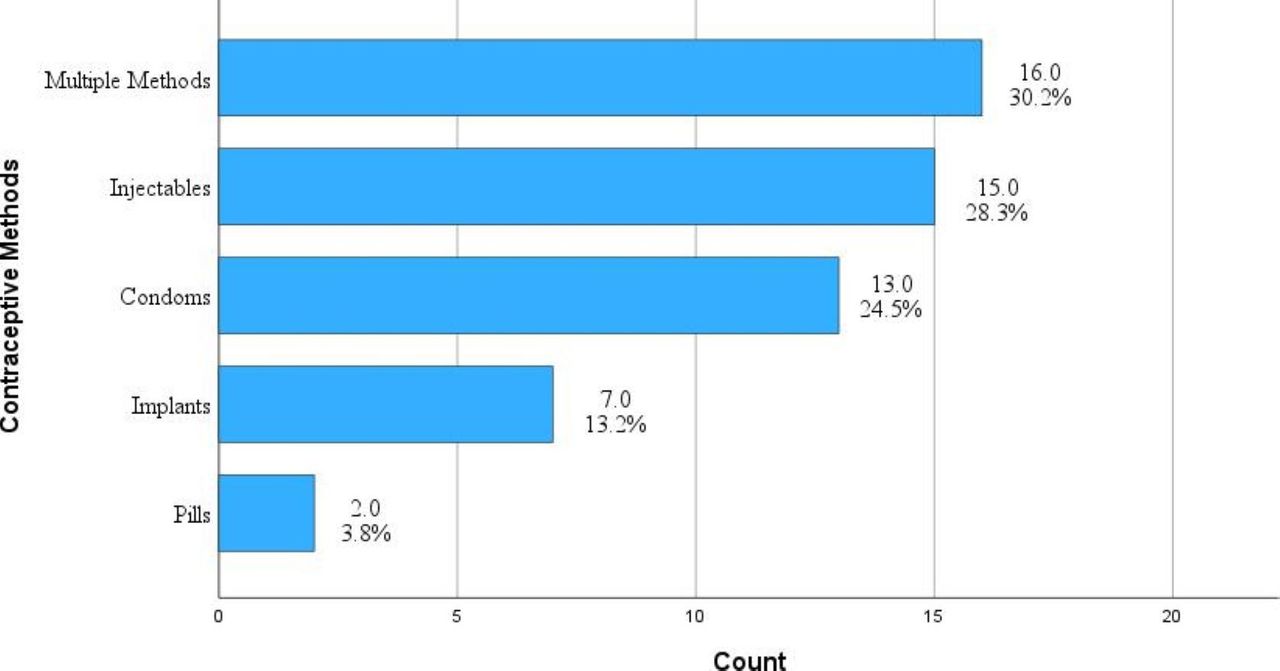
Figure 2 summarises modern contraceptive methods used by teenage girls living in refugee settlements of the West Nile region, in northern Uganda. Among the teenage girls, 13.8% had never used modern contraceptives in their lifetime, only 7.5% were currently using modern contraceptives, of whom only 13.2% reported to have ever used long term contraceptive methods and 30.2% reported to have ever used multiple methods (including long-term and short-term methods). Overall, 17.9% received contraceptive use counselling from home, and 36.1% received home sex education, while 55.1% had received sex education from school, 40.5% had received contraceptives use counselling from school and 64.7% had never been health educated on the dangers of teenage pregnancy.

The different contraceptive methods used by teenage girls living in Palorinya and Bidi Bidi refugee settlements of West Nile region, northern Uganda (n=385; n=53).
Among the respondents, 5.7% had the intention of getting pregnant in the next 12 months, whereas 52.0% had friends who were pregnant and 24.9% were married, of whom 38.5% were forced/arranged. Up to 9.8% of the respondents had ever had an abortion and 22.0% had had a caesarean section.
Period prevalence of teenage pregnancy among 385 teenage girls living in Palorinya and Bidi Bidi refugee settlements of West Nile region, northern Uganda
Figure 1 shows the prevalence of teenage pregnancy among 385 teenage girls living in refugee settlements of west Nile region, northern Uganda. We found out that up to 34.0% of respondents reported to have never gotten pregnant between 2020 to 2023 (CI: 29.4% to 38.9%), and the median number of pregnancies was 1, with a minimum of 1 and maximum of 3.

{kind=link}
{kind=link}
Prevalence of teenage pregnancy among 385 girls aged 15–19 living in Palorinya and Bidi Bidi refugee settlements of West Nile region, Northern Uganda.
Predictors of teenage pregnancy among 385 teenage girls living in Palorinya and Bidi Bidi refugee settlements of West Nile region, northern Uganda
Table 2 summarises the factors associated with teenage pregnancy among 385 teenage girls living in refugee settlements of west Nile region, northern Uganda. At the bivariate level, factors, such as lack of formal education (Prevalence Ratio-PR: 3.1, 95% CI: 2.64 to 3.64, p<0.001), male house hold head (PR: 2.3, 95% CI: 1.72 to 3.13, p<0.001), living with a husband/spouse (PR: 5.4, 95% CI: 4.11 to 7.17, p<0.001), intention to get pregnant (PR: 1.1, 95% CI: 1.03 to 1.15, p=0.003), peer pressure (PR: 3.7, 95% CI: 2.73 to 5.05, p<0.001), being married (PR: 6.6, 95% CI: 4.95 to 8.82, p<0.001), history of contraceptive use (PR: 3.2, 95% CI: 2.55 to 3.94, p<0.001), lack of home sex education (PR: 1.6, 95% CI: 1.16 to 2.24, p=0.005), health education on dangers of teenage pregnancy (PR: 1.8, 95% CI: 1.25 to 2.49, p=0.001), sexual abuse (PR: 2.7, 95% CI: 2.14 to 3.46, p<0.001), physical abuse (PR: 2.3, 95% CI: 1.80 to 2.99, p<0.001) and alcohol consumption (PR: 2.3, 95% CI: 1.77 to 3.03, p<0.001), were positively associated with teenage pregnancy.
Factors independently associated with teenage pregnancy among 385 teenage girls living in Palorinya and Bidi Bidi refugee settlements of West Nile region, northern Uganda
We then performed modified Poisson regression on all variables that had a p value<0.2, while controlling for occupation, media exposure and living with both parents. Teenage girls with no formal education were 2.3 times more likely to be pregnant (aPR: 2.3, 95% CI: 1.26 to 4.35, p=0.007) as compared with those who had a formal education, those who were living with a husband/spouse were 3.8 times more likely to be pregnant (aPR: 3.8, 95% CI: 2.51 to 5.84, p<0.001) as compared with those who lived with their parents, teenage girls who experienced peer pressure were 2.1 times more likely to be pregnant (aPR: 2.1, 95% CI: 1.54 to 2.86, p<0.001) as compared with those who did not, those who had a history of contraceptive use were 1.8 times more likely to be pregnant (aPR: 1.8, 95% CI: 1.31 to 2.33, p<0.001) as compared with those who did not and teenage girls who experienced sexual abuse were 1.5 times more likely to be pregnant (aPR: 1.5, 95% CI: 1.07 to 1.99, p=0.018) as compared with those who did not.
Discussion
This study reveals a high prevalence of teenage pregnancies (34.0%) among teenage girls living in refugee settlements in northern Uganda. Several factors were independently associated with teenage pregnancies in this context, including living with a spouse or husband, lack of formal education, peer pressure and inconsistent use of modern contraceptives. Additionally, 9.8% of the respondents had experienced an abortion, highlighting the potential risks of maternal morbidity and mortality in this vulnerable population. Furthermore, the study identified concerning levels of sexual abuse, with 25% of the perpetrators being relatives, emphasising the challenges faced by these girls in seeking support and justice.
Notably, there is a gap in the literature on sexual and reproductive health issues in humanitarian settings in general, and teenage pregnancy statistics in similar settings is not widely studied. Our study reveals a comparatively higher prevalence of teenage pregnancy in the refugee settings of northern Uganda, way higher than that in other studies. The high prevalence of teenage pregnancy in our study could be because our study only considered teenage girls between 15 and 19 years old, meanwhile the other studies considered teenage girls between 13 and 19 years old. We found a close relationship between sexual abuse and teenage pregnancy, which was similarly observed in Malawi.16 Our study found that up to 25% of the perpetrators of sexual abuse among teenage girls are relatives. This makes it particularly hard to seek support from community and cultural leaders, necessitating the involvement of higher authorities. Several factors were independently associated with teenage pregnancies in our study. Importantly, living with a spouse/husband presented fourfold likelihood of teenage pregnancy compared with those who lived with their parents. Other studies agree with our findings.17 Moreover, we also found out that most of the child marriages in the refugee context were forced (38.5%), similarly observed in different studies.17 Forced and early/child marriage in Bidi Bidi refugee settlement and among Ugandan refugees is a complex issue driven by various factors such as poverty and economic hardship, gender norms and cultural practices, stigma and social pressure.18 Providing education and vocational training for girls, engaging community leaders and members in dialogue and strengthening and enforcing laws against child marriage can provide a legal deterrent, meanwhile offering comprehensive sexual and reproductive health services and support for survivors of child and/or forced marriages can mitigate some of the adverse effects.18
Our study also found that 9.8% of the respondents had ever had an abortion. The limitation is that our study did not explore whether this was induced or spontaneous. Furthermore, we do not know whether this abortion was in the watch of a qualified health service provider. This poses a greater risk of severe morbidity and mortality among teenage mothers in these settings.
Additionally, teenage girls without a formal education stood at a 2.3 times higher risk of teenage pregnancy compared with those with at least a primary education. Similarly, another study conducted in Malawi noted an inequality in teenage pregnancy which worsened to the disadvantage of the less educated.19 Another important predictor of teenage pregnancy in our study was peer pressure. This is related to another study carried out in Kibuku district, Uganda, that pointed out that bad peer groups were an outstanding cause of teenage pregnancy among the respondents.20 ,21 Addressing the challenge of peer pressure requires a multi-sectoral collaboration, involving the Ministry of Health, and education among other ministries.
Paradoxically, our study found out that teenage girls who had a history of using modern contraceptives stood at 1.8 risk of teenage pregnancies as compared with those who did not. These findings were unlike those observed in Malawi,22,13 which otherwise found that the history of contraceptive use was a protective factor. Unfortunately, our study did not distinguish between the use of long-term and short-term contraceptives, in relation to pregnancy. We observed that 13.8% of teenage girls living in refugee settlements reported having ever used a modern contraceptive method in their lifetime. Despite this, given the relatively low average age of sexual debut (15.8 years), only 7.5% were currently using modern contraceptives, with just 13.2% having ever used long-term contraceptive methods. Noting the inconsistencies in the use of modern contraceptives among the study participants makes it possible that these inconsistencies contribute to the high prevalence of teenage pregnancy in this setting. Additionally, the proportion of respondents who had ever used long-term methods is relatively low, leaving a wider window for teenage pregnancies in this setting.
Conclusions and recommendations
Our study found out that about 1 in 3 adolescent girls in refugee settlement of northern Uganda experienced pregnancy during the COVID-19 pandemic. Only 1 in 13 of the adolescents was currently using modern methods of contraception.
Relevant refugee authorities and government stakeholders must develop targeted strategies to address teenage pregnancy in refugee settings, which contributes to the broader issue of maternal morbidity and mortality. This includes exploring legal actions against perpetrators of sexual abuse and implementing measures to combat forced child marriages, such as forming support groups, promoting girl child education and protecting the rights of girls in refugee settlements.
The Ministry of Health, in collaboration with the OPM, should implement measures to combat sexual violence against teenage girls in refugee contexts. This could include enhancing education access for girls, which not only reduces teenage pregnancy but also helps in the fight against HIV. Encouraging the uptake of long-term contraceptive methods and fostering inclusive education solutions will help lower the incidence of teenage pregnancy and address associated challenges.
In as much as this study provides important insights into the sexual and reproductive health challenges faced by adolescent girls in the Bidi Bidi refugee settlement, the findings must be interpreted within the context of the study’s limitations. Future research should aim to include a larger, more diverse sample to further validate these findings and explore the broader applicability of the results.
Supplemental material
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Gulu University Research and Ethics Committee (GUREC), (approval number: GUREC-2022-291). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We acknowledge the Refugee Welfare Councilors (RWCs) and the Office of the Prime Minister (OPM) for allowing us conduct this study in the refugee settlements. Similarly, we thank the participants for taking part in this study. We also appreciate the research assistants; Anthony Ogwang, Geoffrey Okello, Harron Struggle Kojjoki and Lojjo Isaac Jackson for the tremendous work they did. Pre-Publication Support Service (PREPSS) supported the development of this manuscript by providing author training, as well as prepublication peer-review and copy editing.
Footnotes
X @Pebalo Pebolo
Contributors OD is the guarantor. Conceptualisation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Writing—original draft, Writing—review and editing. GO: Project administration, Supervision, Writing—original draft. BOL: Writing—review and editing. RMMM: Writing—original draft, Writing—review and editing. FB: Supervision, Writing—review and editing. FPP: Funding acquisition, Supervision, Writing—original draft, Writing—review and editing.
Funding This research was funded with support from Center for International Reproductive Health Training at University of Michigan (CIRHT-UM).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.