Article Text

Abstract
Objective To codesign and develop an intervention to promote participation and well-being in children and young people (CYP) with acquired brain injury (ABI) and family caregivers.
Design A complex intervention development study including a scoping review, mixed-methods study, co-design workshop and theoretical modelling.
Setting Community-dwelling participants in one geographical region of the UK.
Participants CYP with ABI (5–18 years) and their parents, health, education, social care and voluntary/third-sector practitioners.
Results The intervention development process using a theory-driven and evidence-informed approach, combining the Behaviour Change Wheel and the person-based approach is described. Findings from the scoping review and mixed-methods study were analysed and synthesised using the framework method and the International Classification of Functioning, Health and Disability and the Behaviour Change Wheel. Evidence of identified participation needs, barriers and facilitators was presented at the codesign workshop. The findings demonstrate the significant long-term impact of an ABI on CYP participation and both CYP and parent well-being with significant unmet family needs. Barriers and facilitators were identified, with key barriers being lack of knowledge and understanding, lack of parental and family support and a need for cross-sector collaboration and communication. Stakeholders identified potential solutions and intervention ingredients, such as the need for education for families and schools regarding long-term impact of ABI, and longer-term practical and emotional support for families. Findings from the workshop were analysed using the framework method and synthesised with previous findings using the Behaviour Change Wheel. Theoretical modelling enabled guiding principles to be identified and an intervention logic model to be produced. ‘ABI-Participate’ is a novel, multifaceted intervention, developed with CYP with ABI, their parents and professionals from across health, education, social care and charity sectors. Using a case coordination model, ABI-Participate aims to address the unmet needs and barriers of this population and includes needs assessment, goal setting, action planning, health coaching, practical and emotional support for families and multiagency liaison and collaboration, adopting an individualised needs-based approach.
Conclusion A systematic process using a theory-based, evidence-based and person-based approach resulted in a novel, codesigned, multifaceted intervention, grounded in an in-depth understanding of CYP with ABI participation needs, barriers and facilitators. Further development and refinement of the individual elements of ABI-Participate and the care pathway to support its implementation are now required prior to feasibility testing.
- PAEDIATRICS
- Adolescents
- Brain Injuries
- Quality of Life
- Psychosocial Intervention
Data availability statement
Data are available upon reasonable request. The data that support this study will be shared upon reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Involving children and young people, parents and stakeholders from across health, education, social care and voluntary/third sectors at every stage of this research ensured their views and needs remained at the centre of the process and the intervention.
Use of a theory, evidence and person-based approach ensured a detailed and rigorous intervention development process and a theoretically and contextually informed complex intervention.
The findings from this study may not be generalisable, however, understanding the specific needs within the region is important in planning services and delivering care close to home.
Feasibility and effectiveness testing are now required.
Background
Sustaining an acquired brain injury (ABI) as a child or young person as a result of trauma or non-traumatic causes (eg, infection, stroke, tumour) can lead to an array of physical, cognitive, emotional and behavioural sequelae.1 These sequelae can impact on well-being and participation in activities at home, school and the community.1 2 Outcomes within this population are heterogeneous with a range of influential factors such as injury severity, location, age at injury, premorbid abilities and personal, socioeconomic and environmental factors (eg, family functioning).2 3 Many children and young people (CYP) under the age of 18 experience persistent or life-long effects, which impact on physical and psychological development, quality of life, educational achievement and social inclusion. These continue to emerge months or years after the event as developmental, education and social demands increase.4–7
The International Classification of Functioning, Health and Disability (ICF) defines participation as involvement in life situations, which enhances well-being. It is both a fundamental right and essential part of child development.8 9 Research has shown that participation is associated with improved quality of life, social competence, educational success, future life outcomes and overall well-being of CYP with and without disabilities.10–12 CYP with ABI and their families have reported experiencing participation restrictions, negatively impacting on their well-being, with extensive unmet and unrecognised needs found to persist up to 12 years postinjury.1 13–16 The impact of sustaining an ABI on CYP and their family is well documented. Sudden change in roles, routines and lifestyle for families affected by ABI intensifies stress for the entire family, impacting family functioning and well-being.17 Participation restrictions for a CYP with ABI lead to loss of social interaction, isolation and marginalisation, impacting participation and well-being for the whole family unit.18 19 Additionally, sudden health literacy needs, increased caregiver burden, parental stress and financial hardship can impact the mental and emotional health of the whole family, including siblings.2 20 21 Rehabilitation interventions must consider the entire family’s needs, recognising the interconnectedness of family members’ and that addressing parental needs may improve CYP outcomes.16 21
Rehabilitation following an ABI aims to enable individuals to achieve optimal levels of participation by reducing the impact of difficulties and maximising well-being, activities of daily living, functional ability and social integration.22 23 However, international variability in paediatric rehabilitation provision and follow-up leads to uncertainty regarding long-term CYP with ABI outcomes and the best way to provide long-term support.7 24 Identifying and addressing individual family psychosocial and systemic issues is essential to ensure rehabilitation interventions can be effective.4 The literature recommends family-centred rehabilitation care models, collaborative multisystem interventions and long-term regular follow-up.25–29 However, it remains unclear what components should be included and how these should be delivered to meet the needs of CYP with ABI and their families, and optimise participation and well-being.
Rehabilitation interventions are typically complex with multiple needs and factors to be addressed.28 Complexity is defined by the number of interacting components, a range of possible outcomes, the need to tailor the intervention to different contexts and dependency on the behaviours of those delivering and receiving the intervention.30 31 This complexity makes complex interventions difficult to implement. Factors likely to affect implementation need to be understood and addressed during intervention development. When developing interventions that aim to result in a behaviour change (eg, increasing parental confidence to support their CYP with ABI), we need to understand the target behaviour, its influences, the context for delivery, as well as identify the mechanisms of change and resources required.32
The Medical Research Council’s framework for developing and evaluating complex interventions recommends the use of theory and evidence when designing an intervention.30 Drawing on existing theories, such as the Behaviour Change Wheel (BCW), can help identify important and relevant factors and inform the content and delivery of an intervention.33 34 Evidence from previous research can help define the problem, understand context and identify target behaviours. Uncertainties or gaps in the literature can be addressed using primary data collection, such as quantitative surveys to assess outcomes or qualitative interviews and focus groups to gain deeper understanding of needs, barriers and facilitators.32 Engagement with stakeholders through primary data collection is essential to ensure population needs and context are understood and guide intervention design and implementation into real-world practice.35
We describe the intervention development process for the ‘ABI-Participate’ intervention using an integrated theory-based, evidence-based and person-based approach.32 This approach ensured a pragmatic, systematic, rigorous intervention development process was adhered to. The process necessitates stakeholder engagement and an in-depth understanding of behaviour, its barriers and facilitators, and how implementation of an intervention could change behaviour.34 35 The aim was to codesign and develop an intervention to promote participation and well-being in community-dwelling CYP with ABI (all causes and severities) and family caregivers.
Theoretical frameworks
We integrated the BCW and person-based approach in our intervention development process. The BCW was selected as the most appropriate theory for developing our intervention for CYP with ABI as it provides a systematic process using theory and evidence to develop interventions.36 It incorporates the COM-B model of behaviour which aids description of how capability, opportunity and motivation influence behaviour, and the Theoretical Domains Framework which subdivides the COM-B components to aid greater understanding of barriers and facilitators at individual, organisational and community levels.36 37 Once these have been identified, the BCW leads developers through a process identifying the components required for the intervention. It aids identification of ‘intervention functions’ to target the behaviour and barriers and ‘policies’ to support intervention delivery. This leads to the selection of ‘behaviour change techniques’, specific strategies designed to change behaviour which are the active, observable, replicable and irreducible ingredient of an intervention—that is, the proposed mechanism of change36 (table 1).
BCW components and definitions36
The person-based approach, designed for the development of health-related behaviour change interventions, integrates well with the BCW and provides a process for combining stakeholder coproduction with mixed-methods research.38 It ensures that the views of individuals who will interact with the intervention (ie, key stakeholders such as CYP, parents, health, education, social care and charity practitioners) are included throughout, increasing the likelihood of the intervention being successfully implemented in real-world practice. Guiding principles are formulated, describing the key intervention design objectives which can be mapped to BCW intervention functions and behaviour change techniques (BCTs). This theoretical modelling process facilitated the development of a logic model to describe the intervention, planned mechanisms of change, resources required and impact on outcomes.39
Methods and results
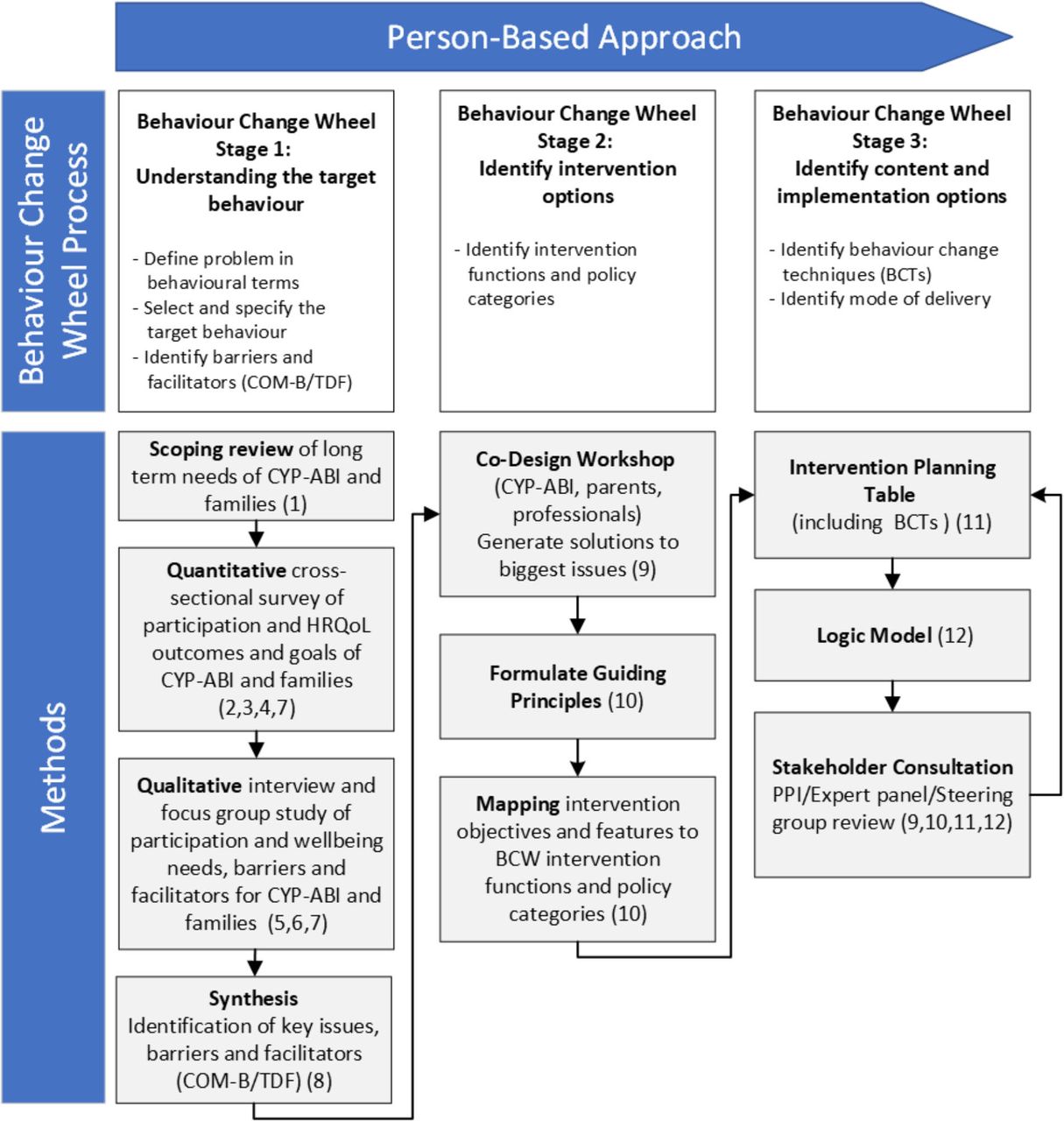
Using the GUIDED framework for reporting intervention development, here we describe the methods and results for each stage of the intervention development process following the process as depicted in figure 1.40

Intervention development process and methods employed. ABI, acquired brain injury; BCT, behaviour change technique; BCW, Behaviour Change Wheel; CYP, children and young people; TDF, Theoretical Domains Framework.
Patient and public involvement
CYP with ABI, their parents and stakeholders representing health, education, social care and voluntary/third sectors were involved throughout the study. Four families were involved in identifying the research question and design of the study. One young adult with ABI has assisted with the data analysis and synthesis and dissemination, including being a coauthor on this paper. Findings from each stage were disseminated to study participants during the codesign workshop. The findings and recommendations will be disseminated further via the production of a lay summary video.
Stage 1: understanding the target behaviour
To understand the target behaviour, the problem needs to be defined, target behaviour selected and specified and barriers and enablers identified. A scoping review of the literature and primary mixed-methods research was conducted to address this aim.
Synthesis of relevant literature: scoping review
We conducted a scoping review to identify relevant literature regarding the needs of CYP with ABI and their families, and whether needs were met, unmet or unrecognised. The methods and findings of this are reported elsewhere.13 Four themes were found regarding needs related to CYP’s impairments, parent and family support, return to school and long-term aftercare. Needs were mapped onto the ICF, with a substantial proportion of needs relating to participation and contextual factors. Key findings were the impact on parents and family and the lack of communication, collaboration and long-term follow-up. A lack of awareness and understanding underpinned all reported needs and led to many needs being unrecognised. Recommendations within the majority of the articles reviewed included the need for specialist follow-up and integrated care pathways that are CYP and family centred. However, there were gaps in the literature. The voices of CYP are limited, there is a lack of focus on personal factors such as psychological and emotional needs for the CYP and families, a lack of focus on community participation, including recreation and leisure activities, and a lack of data regarding outcomes and needs within a UK National Health Service context. These findings led to the development of a mixed-methods research study.
Mixed-methods research study
An exploratory sequential mixed-methods study was designed to explore the long-term participation and well-being needs of CYP with ABI (5–18 years) and their families, 1–4 years after injury, in one geographical region in the UK.
The study consisted of a quantitative cross-sectional survey which explored participation and well-being outcomes and goals of CYP with ABI and their parents. Qualitative interviews and focus groups were conducted with CYP with ABI, parents and stakeholders to explore needs, local context and barriers and facilitators in more depth. We began recruitment in March 2021 with all surveys, interviews and focus groups completed by November 2022. The methods and findings from each of these studies are summarised below and reported more fully elsewhere.16 41
Quantitative study
Survey results demonstrated the significant long-term impact of an ABI on CYP participation and both CYP and parent well-being; 72% of CYP had severely restricted participation, 67% had reduced health-related quality of life (HRQoL).16 Around half (53%) of parents reported reduced HRQoL and family functioning and 37% of parents screened positive for anxiety/depression. Relationships were found between CYP and parental outcomes. Higher CYP participation and HRQoL was related to higher parental HRQoL and family functioning. Higher levels of parental anxiety/depression were related to lower CYP participation and parental HRQoL and family functioning. CYP and parents reported goals that mapped to the activity and participation domains of the ICF, demonstrating the importance of these activities to their well-being.
Qualitative study
The qualitative study involved CYP with ABI and their parents who had participated in the survey and health, education, social care and voluntary/third-sector stakeholders. Significant unmet participation needs were found, impacting CYP with ABI and family well-being.41 Barriers and facilitators, mapped to the BCW, spanned ‘capability, ‘opportunity’ and ‘motivation’. The greatest barriers aligned to the TDF domains of knowledge, skills, social influences, environmental context and resources, social identity and emotion. Identified facilitators included increasing awareness and understanding, supporting parents, long-term access to specialist assessment and rehabilitation, peer support and integrated collaborative pathways.
Mapping of current service provision
Current service provision and pathways were mapped out of the information provided by stakeholders and members of the research team and study steering group who work within the clinical service (online supplemental file 1). The mapping demonstrated the complexity of communication and referral routes from acute to community health services, and between health, education and social care providers. Additionally, the lack of provision or capacity of long-term specialist support services and collaborative care pathways was clear.
Supplemental material
Synthesis of findings
Following the person-based approach and BCW intervention development process, the findings of the literature review and mixed-methods research were collated and synthesised using the Framework Method of analysis to map the findings and themes to the ICF, COM-B and TDF.42 43 This enabled us to define the problem in behavioural terms, identify the target behaviour and identify and specify barriers and facilitators (online supplemental file 2). This also allowed us to consider what needs to change and at what level. Specifying the barriers provided clarity regarding those that were individual factors (CYP/family), external organisational-level (health/education systems) and community-level (society) factors. Although there were individual factors with every CYP with ABI and family experiencing unique circumstances, there were many commonalities and a multitude of external factors that impacted on families in similar ways. Four key issues were identified and used to inform the design of the intervention:
Supplemental material
Reduced CYP with ABI and family participation and well-being—support needed to enable participation and improve well-being by addressing unmet needs.
Lack of practical, psychological and emotional support for parents—support needed for parents to enable them to navigate systems and processes and support their CYP.
Lack of understanding and awareness—training and education needed for those who support CYP with ABI across health, education, social care, voluntary/third and community sectors.
Lack of cross-sector collaboration—a need to improve communication and collaboration between sectors and access to support in the years after ABI.
A multifaceted intervention was required to target key issues that are common across the CYP with ABI population while also providing individually tailored support to meet the specific needs of CYP and their families.
Stage 2: identify intervention options
The next stage in the BCW process was to link the ‘behavioural diagnosis’ (online supplemental file 2) with intervention functions likely to be effective and policy categories that can aid implementation.36
As we had identified a large number of barriers and facilitators, there was a need to prioritise which were to be targeted. We therefore consulted CYP, parents and stakeholders on this and asked for their help in generating potential solutions.
Codesign workshop
An experience-based codesign workshop with multiple stakeholders (CYP, parents and health, education and voluntary/third-sector practitioners) was held in person in July 2023. The aim was to codesign and develop an intervention to promote participation and well-being in CYP with ABI and family caregivers. The objectives were to present and confirm the key issues identified, discuss priorities and generate possible solutions and identify local context-specific barriers/enablers to intervention delivery.39 The data collected informed the guiding principles and theoretical modelling of the intervention.
Procedure
Participants were recruited from those who participated in the interview and focus group study with an invitation to attend the workshop sent by email. Additionally, members of the research team, study steering group (healthcare professionals from the acute neurorehabilitation team) and a patient and public involvement representative were present at the workshop to assist with facilitating groups and contribute.
All participants provided written consent/assent prior to the workshop, with parents consenting for CYP under 16 years alongside their CYP’s assent. An external facilitator (AH) ran the workshop on the day, to allow the research team to listen and document discussions. The four main issues identified from the previous research, and the aims of the workshop were conveyed to the participants by the researcher (RK). Three break-out groups discussed solutions focused on the main issues, each group was facilitated by a member of the research team and study steering group (KR, JCM, DC, MD). Parents and professionals were divided between two groups, one focusing on parental support and the other on cross-sector collaboration/pathway. A separate group for the CYP was supported by a facilitator, patient and public involvement representative (VL) and play specialist (AP). A range of resources were provided to each group—paper, post-it notes, pens and Lego. The ‘draw, write, tell’ technique was used within the CYP group with the facilitators ensuring CYP’s artwork or verbal contributions were well described in written form.44 The groups reconvened and each fed back to the whole group, where potential solutions were discussed.
The workshop findings were collated and analysed by RK using content analysis to code and categorise the data to the COM-B/TDF using the framework method of analysis.42 43 The findings and themes were discussed with the research team and study steering group to ensure rigour by reviewing and triangulating the findings, validate the coding and reduce potential biases.
Findings
In total, 17 participants attended the workshop including four CYP aged 6–17, four parents (mothers), eight health, education, social care and voluntary/third-sector practitioners (including members of study steering group) and one young person PPI representative.
Ten themes emerged regarding possible solutions for the identified issues which were mapped to the COM-B/TDF (table 2). Within these themes the priorities for intervention were identified as ongoing monitoring of CYP needs and goal setting, a single point of contact and support for parents and communication and coordination between sectors. These findings were used to inform the theoretical modelling of the intervention.
Workshop findings mapped to COM-B/TDF
Theoretical modelling
Formulate guiding principles
Using the previously synthesised findings and the findings from the codesign workshop, we developed guiding principles. These detail the key issues to be addressed, and the intervention design objectives and distinctive features that are key to successfully addressing the issues (table 3).
Guiding principles/intervention planning table
Mapping intervention design objectives and features to BCW
Using the BCW, we mapped the intervention design objectives to the nine intervention functions. We identified the corresponding intervention functions that are likely to be effective in addressing the identified barriers and achieving the intervention objectives. Three intervention functions, ‘education’, ‘training’ and ‘enablement’ were identified that could address multiple barriers (online supplemental file 3).
Supplemental material
The next step was to consider which of the seven BCW policy options would support the delivery of the identified intervention functions.36 We identified three policy options that would be appropriate for supporting the delivery of the selected intervention functions—‘communication/marketing’ (using print, electronic, telephonic or broadcast media), ‘guidelines’ (creating documents that recommend or mandate practice) and ‘service provision’ (delivering a service) (online supplemental file 3).
Stage 3: identify content and implementation options
Behaviour change techniques
The next step was to identify which ‘behaviour change techniques’ are most appropriate for the intervention objectives and functions, and which mode of delivery was best suited. Using the BCT taxonomy (v1) we identified the BCTs required for each intervention objective and function, ensuring these also correlated with the COM-B/TDF domains that were originally identified as important to target.36 The guiding principles combined with the identification of BCTs and intervention components enabled a detailed intervention plan to be added to the guiding principles table (table 3).
Mode of delivery
Deciding on the mode of intervention delivery was important. Considering the workshop findings, participants wanted a range of options, including face-to-face as individuals or in group settings, and ‘distance’ meetings via telephone or virtual meeting platforms. As the target population have differing needs and reside across a large geographical region, covering five counties, a range of intervention delivery modes were needed. For example, education and training for a school could be delivered virtually or in a group face-to-face. It will be important to assess the acceptability, practicality and affordability of intervention delivery within feasibility testing to ensure it is effective for families living across the region.38
Logic model
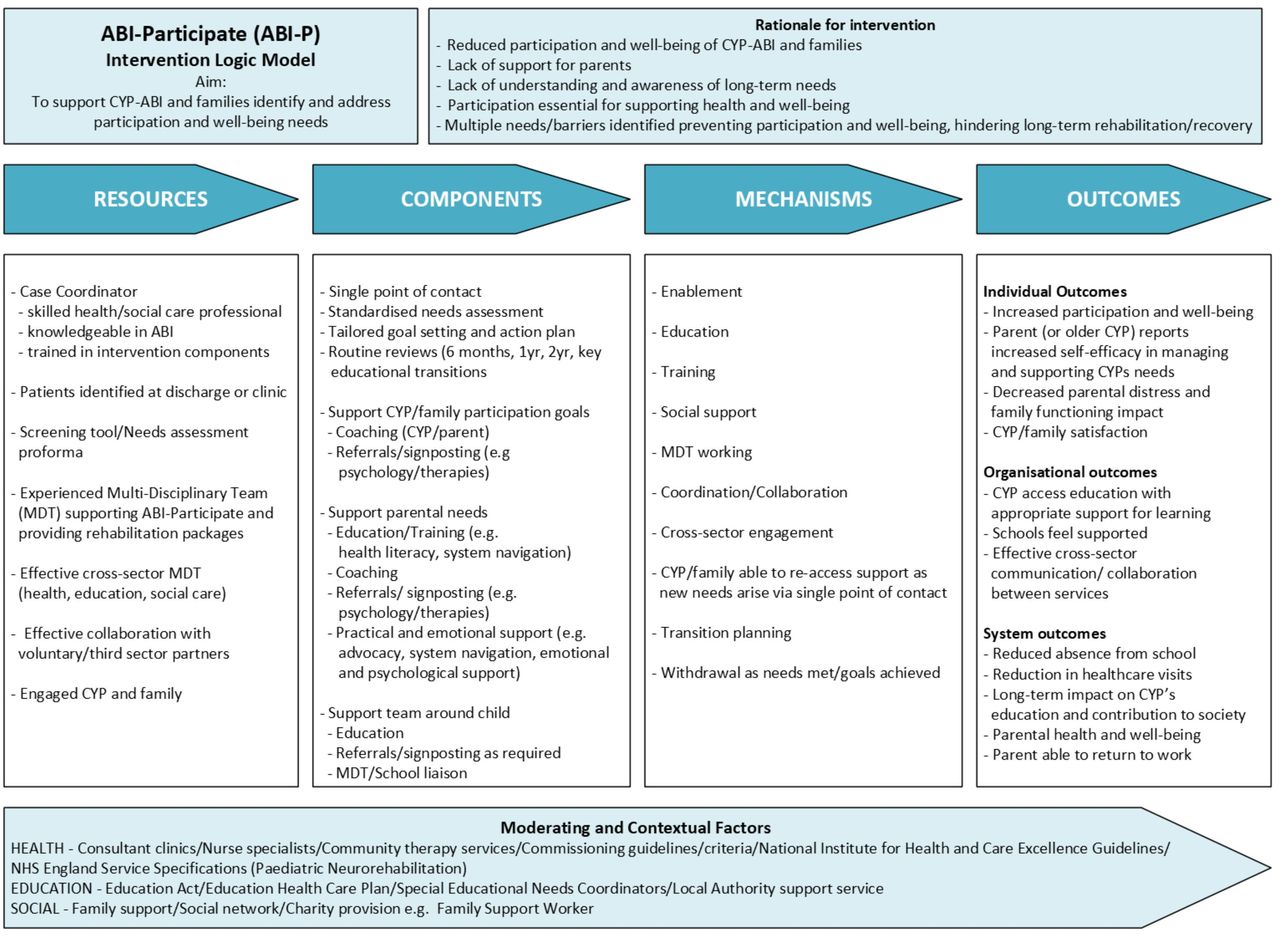
Following the systematic and detailed BCW intervention design process enabled the key objectives and active ingredients for the intervention to be identified leading to the production of a logic model that included a description of the core components, necessary resources, mechanisms of change and identification of short-term and long-term impacts and outcomes for the intervention (figure 2). This was developed iteratively, through review with the research team, study steering group and patient and public representative, and refinements made. The TIDieR Checklist informed the description of the intervention.45

{kind=link}
{kind=link}
ABI-Participate logic model. ABI, acquired brain injury; CYP, children and young people; MDT, multidisciplinary team.
The ‘ABI-Participate’ intervention aims to support CYP with ABI and their families to identify and address participation and well-being needs. Using a case coordination model, needs assessments and individualised goal setting and action planning would be completed with CYP and families, considering development stage and family context.46–48 This includes supporting participation goals through coaching CYP and parents and ensuring referrals for additional therapy or support are made where necessary. Families and professionals wanted a single point of contact and signposting to sources of information and support. ‘ABI-Participate’ also includes information sharing and team meeting coordination, liaison with CYP’s school/college and supporting parental practical, emotional and psychological needs. The intervention would continue until needs were met or goals achieved, with a single point of contact in the long-term, should families or those working with a CYP with ABI need advice or support. Other features included reassessment of needs at routine reviews in a follow-up clinic, ahead of key educational stage transitions or as new needs emerge. Coordination of transition to adult services would also be provided. The intervention would help to improve understanding and awareness of long-term needs. It would increase support for parents and CYP to improve their participation and well-being by identifying and addressing needs of the whole family. It would help families and health, education, social care and voluntary/third-sector practitioners working with CYP with ABI and their families to overcome barriers by helping to coordinate cross-sector communication and collaboration. The intervention needs to be situated within and supported by a multidisciplinary neurorehabilitation service. The multidisciplinary team would need capacity to support the assessment of needs and provide targeted rehabilitation interventions, when needs are identified, such as neurocognitive interventions or higher-level physical skills training required for return to sport.
Discussion
This paper has described how we used a theory-based, evidence-based and person-based approach to develop a complex intervention aimed at improving participation in CYP with ABI and their families. As recommended by the Medical Research Council’s guidance, underpinning the development of complex interventions with theory and evidence is essential to ensure interventions are evidence informed and grounded in a theoretical understanding of behaviour change.30 32 The addition of the person-based approach ensured an in-depth understanding of the life experiences of the population and stakeholders, their needs and views on acceptable solutions.39 As this approach focuses specifically on the development of complex behavioural interventions, it was well suited to be combined with the theory and evidence approach in this work.49
The intervention we have developed is founded on the biopsychosocial model of the ICF and multidisciplinary teamwork. It is multifaceted, family-centred and tailored to developmental stage, individual needs and contexts. It follows a rehabilitation process, involving assessment, goal setting, intervention delivery, monitoring and review.23 Based on a case coordination model, ABI-Participate also includes a therapeutic element of goal-oriented coaching, which aims to identify and address the participation needs of the whole family. As found in this study, and recommended by the WHO, there is an increasing acknowledgement of the need for care to be coordinated to support those living with long-term conditions and their family caregivers due to the complexity of coordinating care, ensuring needs are met and undue stress prevented.21 48 50–52
Gagnon et al 47 identified six key supportive roles that family members of adult traumatic brain injury survivors undertake—researcher, advocate, case manager, coach, activities of daily living supporter and emotional supporter. They concluded that family members require ongoing counselling, support and education about system navigation, accessing community programmes and workplace rights to prevent burnout. A scoping review by Gardiner et al 48 found a diversity of terminology and descriptions used for navigation-type models for children with neuro-disabilities. However, each was characterised by four central domains: facilitate—integration/coordination of resources, supports and services; provide—information, advice and education; intended outcomes—improved health, behaviour and capacity and reduced patient and family distress and guiding principles—client-directed, family-centred and collaborative. These findings align with the findings of our study and are incorporated into the proposed ‘ABI-Participate’ intervention.
An additional element identified in our study, and by Gagnon and colleagues,47 was coaching and supporting CYP and families in identifying and achieving participation goals. Palisano et al 53 proposed a conceptual framework for optimal participation of children with physical disabilities that considers the dynamic interaction of determinants (child, family and environment) and dimensions (physical, social and self-engagement) of participation. Their recommendation that interventions need to be goal-oriented, family-centred, collaborative, strengths-based and ecological also aligns with our findings. ABI-Participate could be used flexibly and at different time points, recognising that needs differ at different developmental stages and points of transition (ie, more intensive support needed during educational transitions, particularly into secondary school and transition to adult services and/or employment).
Health coaching is defined as ‘a goal-oriented, client-centred partnership that is health-focused and occurs through a process of client-enlightenment and empowerment’ (p24).54 Coaching can help patients and families identify and achieve their goals and has been shown to be effective in positively influencing health status, health behaviours and costs.21 There is increasing evidence supporting coaching in promoting parental self-management and empowerment, addressing parental health literacy and advocacy skills, and CYP participation in parents of CYP with chronic disabilities.21 55 Ogourtsova et al 21 systematic review of health coaching for parents of children with developmental disabilities found heterogeneity within the interventions with some being CYP-directed, some parent-directed and some mixed. They recommended further research exploring the outcomes of the different modes of delivery and the effectiveness of these on CYP and parental outcomes, recognising that these are linked with CYP outcomes improving when parent-related outcomes improve.
Existing interventions could be integrated with ABI-Participate. For example, goal-directed interventions (eg, PREP—Pathways and Resources for Engagement and Participation), coaching interventions (eg, CO-OP—Cognitive Orientation to Occupational Performance), parent interventions (eg, Stepping Stones Triple P) or psychological interventions (eg, Acceptance and Commitment Therapy).55–57 However further research is recommended to further explore the acceptability and effectiveness of integrating them in this intervention.
The technological advances enabling the widespread use of virtual meeting platforms for health consultations during the COVID-19 pandemic, have made telehealth delivery of some components of ‘ABI-Participate’ possible.58 59 Not only are most patients and families now familiar with these platforms, but workshop participants suggested them as plausible modes of delivery. This enables specialist rehabilitation in tertiary settings to be made accessible to people living at long geographical distances and also offers an opportunity to upskill and support local providers with education and training delivered virtually. This delivery mode is in use in Rohrer-Baumgartner et al’s ‘Child in Context’ study.28 A future feasibility study should include exploration of both its acceptability and utility, as well as how to deliver this to those without access to the internet.
Strengths and limitations
The strengths and limitations of the scoping review, survey and qualitative study are reported elsewhere.13 16 41 Involving CYP, parents and stakeholders from across health, education, social care and voluntary/third sectors at every stage of this research is a strength, ensuring their views and needs remained at the centre of the process and the intervention. To our knowledge, this is the first intervention development study within the CYP with ABI literature to have used a theory, evidence and person-based approach. This novel paper demonstrates the value of combining these approaches to develop a complex intervention for addressing participation needs in CYP with ABI and their families. By following the person-based approach and BCW process, a detailed and rigorous approach was employed to understand needs, identify barriers and facilitators and design the intervention (including the active ingredients/mechanisms). The mixed-methods design enabled us to define the problem further, understand the local context and, using theory, provide a detailed description of the barriers and facilitators to participation. The addition of the codesign workshop with stakeholders to prioritise and generate solutions was invaluable in ensuring the most pertinent targets were selected. The theoretical modelling process and use of guiding principles enabled us to clearly and systematically articulate and document the process of identifying the key objectives, features and functions of the intervention and selection of the policy options for implementing it. Finally, the logic model presented an overview of the intervention, the resources, core components and mechanisms as well as the contextual factors that must be considered and the outcomes that could be measured to assess effectiveness.
This study was conducted in one region within the UK and therefore findings may not generalisable, however, understanding the specific needs within the region is important in planning services and delivering care close to home. While every attempt was made to ensure diverse representation at every stage, this did not occur within the workshop, partly due to some participants being unable to attend on the day. However, the reported needs, barriers and facilitators align with those reported internationally and many of the themes from the qualitative study, which had more diverse representation, were repeated and affirmed at the workshop. This intervention has been developed iteratively, with CYP, parents and stakeholders. Further stakeholder and patient and public representative consultation and expert consensus development workshops are now required to refine, specify and confirm intervention components prior to feasibility testing.
Future directions
There is evidence of effectiveness for the different components of our intervention, but research is needed to test the feasibility of the intervention in our target population and context, and to investigate its acceptability, deliverability and effectiveness. Within this, identification of standardised outcome measures and methods of determining whether needs are met are required to measure effectiveness. Further consideration also needs to be given to the overall care pathway for CYP with ABI in which this intervention would be situated following hospital discharge. Given the barriers reported and lack of access to rehabilitation, other elements need to be developed and delivered alongside this intervention. For example, specialist rehabilitation and review clinics, particularly for those CYP whose needs cannot be met within primary care, mental health or community therapy services (eg, cognitive, neuropsychological or higher-level motor therapy needs that do not meet referral criteria). For ‘ABI-Participate’ to be effective, there needs to be referral pathways for CYP with these needs. The mapping of regional service provision demonstrated that these do not exist, except for a very limited regional ABI medical follow-up clinic and neuropsychology service, with long waiting lists, further delaying access to support.
Conclusions
This research has provided an in-depth understanding of the participation and well-being needs of CYP with ABI and their families. The findings demonstrate the significant long-term impact of an ABI on CYP participation and both CYP and parent well-being with significant unmet family needs. Barriers and facilitators that families and stakeholders face in accessing support and rehabilitation are identified. Key barriers identified were a lack of knowledge and understanding of the impact of ABI across every level of society, lack of parental and family support and a need for cross-sector collaboration and communication. Providing parental support, long-term access to specialist assessment and rehabilitation, peer support and integrated collaborative pathways were identified as facilitators.
We have iteratively developed a novel, multifaceted intervention the ‘ABI-Participate’ intervention with CYP with ABI, their parents and stakeholders from across health, education, social care and voluntary/third sectors with the aim of addressing the unmet needs and barriers of this population. Adopting a case coordination model and an individualised needs-based approach, ABI-Participate includes needs assessment, goal setting, action planning, coaching, practical and emotional support for families and multiagency liaison and collaboration. Further refinement of the components of ABI-Participate and development of the care pathway to support its implementation are now required prior to feasibility testing.
Data availability statement
Data are available upon reasonable request. The data that support this study will be shared upon reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by East Midlands-Nottingham 2 Research Ethics committee (REC-20/EM/0258) and University of Nottingham, Faculty of Medicine and Health Sciences Research Ethics Committee (FMHS 234-0323). Informed consent/assent was gained from all participants via survey completion and written consent forms.
Acknowledgments
The authors thank Denise Crozier and Melanie Dean for assisting with facilitating the workshop groups and with the intervention development, Angela Horsley for facilitating the codesign workshop and Alison Price for providing play specialist support to the CYP workshop participants. Our thanks go to the children and young people, their parents/carers and the stakeholders that took part in this study, our patient and public involvement families, the study steering group and clinical team for their ongoing support.
References
Footnotes
X @rachyk77, @rehab_research
Contributors RK conducted the scoping review, mixed-methods study and workshop, the primary data analysis, wrote the manuscript and is guarantor. KR, JCM, EB, VL assisted with the workshop in facilitating the groups, assisted with the data analysis and contributed to writing the manuscript. KR, JCM, JK, JW supervised the research, assisted with the data analysis, framework mapping and contributed to writing the manuscript. All authors assisted with the intervention development.
Funding This study is funded by the NIHR Applied Research Collaboration East Midlands (ARC EM). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Competing interests RK received PhD studentship funding from NIHR Applied Research Collaboration-East Midlands, University of Nottingham and Health Education England. JM receives funding from NIHR (UK) and NIH (US). KR receives funding from NIHR HTA grant funding (15/130/11), NIHR Programme Grant funding, NIHR HealthTech Research Centres, EPSRC Rehabilitation Technologies Network, NIHR School of Primary Care Research, MS Society. JM is a Data Monitoring Committee member—del Nido versus St. Thomas’ blood cardioplegia in the young (DESTINY) trial: a multicentre randomised controlled trial in children undergoing cardiac surgery (funded British Heart Foundation). RK is a Topic Advisor (Children and Young People) NICE Guideline Committee—Rehabilitation for Chronic Neurological Disorders. KR was an unpaid advisor to NHS England in the development of a toolkit for NHS professionals to support return to work after stroke. KR was a member of the NIHR HTA Clinical Evaluation and Trials panel between 2017– 2021, JM is current member of the NIHR RfPB East Midlands panel. JK, JW, EB and VL have no competing interests to disclose.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.