Article Text

Abstract
Introduction Necrotising enterocolitis is a devastating gastrointestinal disease predominantly affecting preterm infants. In 40% of cases, its rapid progression renders conservative treatment insufficient, necessitating laparotomy as the sole viable option for survival. However, high perioperative and postoperative mortality rates, along with severe future potential disabilities and suffering, can complicate the decision of whether surgery is still in the infant’s best interest. In such cases, palliative care, aimed to minimise suffering, may be considered as an alternative to laparotomy, especially when the infant’s expected quality of life and overall prognosis are concerning. Depending on the sociocultural context, parents are increasingly involved in this decision. However, weighing the risks, benefits and uncertainties can be challenging for them. Therefore, we aim to develop a decision support tool using a novel combination of the Delphi technique and Q-methodology. Ultimately, we anticipate that this approach will contribute to improved family-centred care and optimised outcomes.
Methods and analysis The first phase of the study aims to identify key factors guiding Dutch parents’ decisions between laparotomy and palliative care (decision factors). Using a Delphi process, parents with varying perspectives and experiences will evaluate decision factors found in the literature and those self-suggested. The pertinent set of decision factors is defined during a consensus meeting.
During the second phase, parents are asked to compare statements about these decision factors using Q-methodology. A by-person factor analysis of these comparisons will identify different parental decision-making profiles, which allows for formulating advice tailored to those profiles.
Ultimately, we will build an online decision support tool which facilitates the classification of parent perspectives. The tool will then provide the parents with the relevant advice. In the last phase of the study, the tool’s effectiveness will be evaluated through an online questionnaire, asking parents to imagine using the tool in a real-world scenario.
Ethics and dissemination Ethical approval has been obtained from Central Ethics Review Committee of The University Medical Center Groningen (METc 2023/577, CTc UMCG 153660). Participants will be asked to provide their informed consent for the parts of the study that involve non-anonymous data gathering. Findings will be disseminated through academic journals and conferences. Options for long-term data preservation are under consideration.
- NEONATOLOGY
- Decision Making
- Paediatric surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study will use a combination of established methodologies, including the Delphi technique and Q-methodology, to explore parental decision-making in surgical necrotising enterocolitis, serving as a proof of concept for other medical-ethical decisions.
Engaging a diverse range of participants leads to the representation of various parental perspectives, thereby enhancing the study’s applicability and relevance across different demographic contexts.
The qualitative nature of employed methodologies such as Q-methodology introduces subjectivity in data interpretation, which is mitigated by the professional and rigorous oversight of the steering group.
Decision factors identified may evolve over time due to changes in medical knowledge, necessitating periodic reviews and updates of the tool.
Despite sociocultural contexts, the proposed method may provide a general framework to support parents in medical ethical decision-making, ultimately allowing for the development of universally applicable decision support tools.
Introduction
Necrotising enterocolitis (NEC) is a devastating gastrointestinal disease predominantly affecting preterm infants and is characterised by inflammation and necrosis of the intestinal tissues.1–3 The emotional toll on parents confronted with a diagnosis of surgical NEC for their child is immeasurable, as they navigate through the complexities of treatment decisions, potential long-term consequences and the uncertainty surrounding their infant’s health.4–7 In such challenging circumstances, the need for effective decision support tools becomes paramount, aiming to empower parents with comprehensive information and guidance to make more informed decisions about their child’s care that connect well to their norms and values.
This study protocol outlines the development of a decision support tool for Dutch parents coping with a child diagnosed with surgical NEC. Surgical NEC, which is defined by pneumoperitoneum and/or clinical deterioration despite maximal medical therapy,8 renders conservative treatment insufficient and makes laparotomy the only viable option for survival. However, given the high perioperativ and postoperative mortality rates, as well as the potential for long-term severe disabilities and suffering and impaired quality of life, there is significant uncertainty about whether surgery serves the best interests of the infant.8–14 Depending on the sociocultural context, physicians and parents might want to prioritise the child’s quality of life and choose palliative care as a more appropriate course of action. This is, for example, observed in clinical practice in the Netherlands, where there is a gradual shift towards patient-centred, shared decision-making.15–17
The Dutch Guideline for Necrotizing Enterocolitis and the Guideline Palliative Care for Children, established by the Dutch Association for Pediatrics, outline specific indications for surgical intervention in cases of NEC and criteria for palliative care, emphasising the importance of enhancing the quality of life for affected children.18 19 However, within these guidelines, a grey area persists regarding the estimation of (future) suffering and the anticipated quality of life. This highlights a need for structured frameworks and supportive tools to navigate the complexities of decision-making processes. General resources, such as the Neonatal Infant Pain Scale and Clinical Risk Index for Babies II, offer valuable quantitative assessments to help quantify risks and inform decisions regarding appropriate care.20 21 Our goal is to develop a tool that complements existing quantitative measures by providing a qualitative approach tailored to distinct parent profiles. Additionally, unlike parent decision aids that have recently been developed for end-of-life considerations for preterm infants at the limit of viability, our tool stands out by extending its focus beyond the prenatal stage.22 23 By concentrating on the more specific and critical scenario of NEC, our tool aims to guide and support parents facing the specific NEC-related intricacies of decision-making during the neonatal period.
The overarching aim of this initiative is to provide parents with a structured and accessible tool that effectively empowers parents and enhances collaboration with healthcare professionals, which improves active participation in the decision-making process.24–26 In order to do so, we will start by determining which factors parents consider important when it comes to the decision of laparotomy or palliative care in surgical NEC as well as identifying the different decision-making profiles that parents may have. Equipped with this understanding, we will construct an online decision support tool featuring advice tailored to the different profiles. Finally, a questionnaire will be conducted in which participants are asked to imagine using the tool in a real-world scenario to assess its effectiveness in the aforementioned aspects. Through this research endeavour, we envisage that this approach will contribute to the improvement of family-centred care for infants diagnosed with NEC, ultimately striving to optimise outcomes and support for both parents and their vulnerable infants. Finally, we aim to lay the groundwork for addressing similar medical-ethical dilemmas, where our approach may offer valuable insights and guidance.
Methods and analysis
The research design adheres to a systematic and encompassing process involving literature review, expert consultation, and notably, the integration of parental viewpoints. The methodological approach outlined here aims to ensure the effectiveness of the decision support tool in guiding Dutch parents through the challenging choice between laparotomy and palliative care for infants diagnosed with surgical NEC. The effectiveness of the decision support tool will be determined by parental feedback, particularly regarding its ability to facilitate well-informed decisions aligned with the parents’ values and preferences. Additionally, we will assess whether parents would feel empowered to collaborate effectively with healthcare professionals with the aid of this tool.
Design
A multidisciplinary steering committee has been established to ensure the proper execution of the study (comprising RV, EMWK, SAO-B, RG, NHML, AAEV and JBFH). All members of the steering committee have extensive experience with NEC. Notably, SAO-B serves as a representative of the Dutch neonatal parent and patient advocacy organisation Care4Neo. Care4Neo specialises in advocating for parents of preterm, dysmature or congenitally ill children, thereby offering valuable expertise in supporting parents and patients affected by NEC.
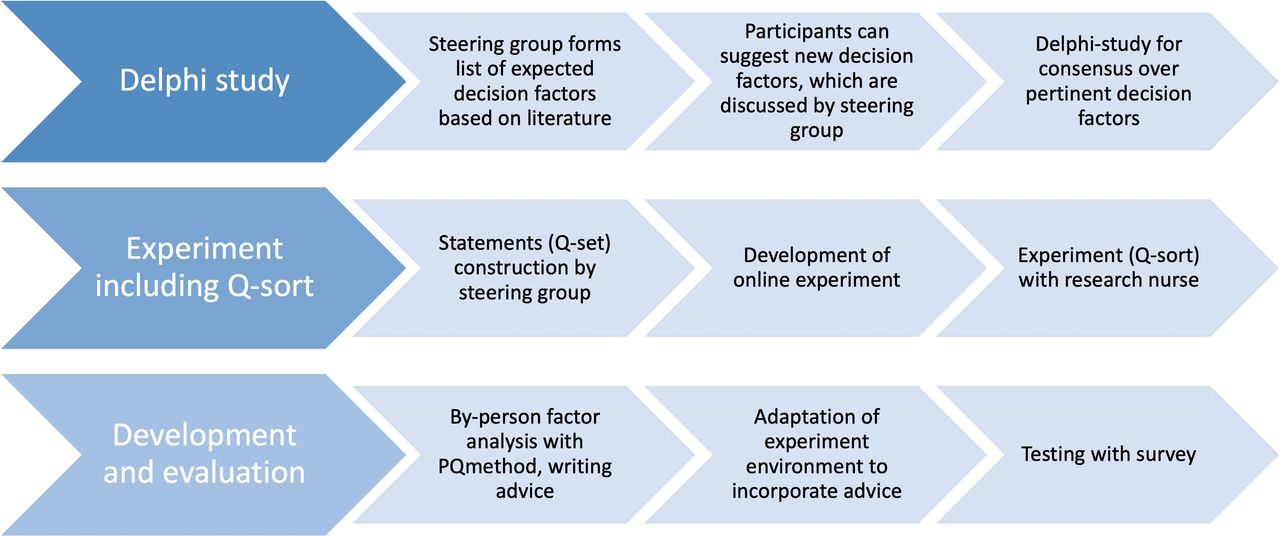
Ethical approval has been obtained from Central Ethics Review Committee of The University Medical Center Groningen (METc 2023/577, CTc UMCG 153660). Electronic informed consent will be obtained from all participants in those parts of the study for which non-anonymous data are collected. Steps to develop the parent decision support tool can be seen in figure 1.

{kind=link}
Overview study protocol. Including all steps that will be followed to develop the parent decision support tool.
Patient and public involvement
The involvement of parents in our study began during consultations with individuals facing the challenging decision between surgery and palliative care in surgical NEC. This decision may, for example, arise for a neonate born at 24 weeks gestational age with multiple severe comorbidities, including significant brain injury, sepsis and NEC that leads to bowel perforation. Given the poor prognosis and potential for long-term disabilities, palliative care may be considered as a compassionate alternative to invasive interventions, focusing on the infant’s comfort and quality of life. It was during such situations that the need for a decision support tool became apparent, prompting the initiation of our research. Throughout the entire study process, we are guided by representatives of patient organisations, ensuring that the research remains patient-centred and responsive to their needs.
Parents will play an active role in all three phases of the study, contributing valuable insights into the relevant decision factors, perspectives on the decision-making process and the evaluation of the final decision support tool. While they did not directly assist in the recruitment or conduct of the study, patient organisations are actively involved in the recruitment process. Additionally, parent representatives will be actively engaged in the dissemination of study results through their own networks, ensuring that findings reach the relevant communities.
Step 1: Delphi study
By means of a Delphi procedure, we aim to collectively gather input and feedback from several parent panels to synthesise a conclusive set of factors that are considered to affect parents who have to decide between laparotomy or palliative care for their infant.
Initial list of decision factors
First, the steering committee identified relevant decision factors by thoroughly reviewing existing literature pertinent to the topic. While our approach did not entail a systematic search, we adopted a comprehensive strategy to collect relevant studies and publications. This encompassed searching the electronic database PubMed, using keywords and phrases associated with short-term and long-term consequences of NEC7–13 27–31 and preterm births in general.32–34 In addition, the steering group has taken into account research on psychological and emotional impacts on parents facing (similar) critical medical decisions.35 36 We decided on an initial list of decision factors which can be found in table 1. This list will be used as a basis for the Delphi procedure.
Expected decision factors
Participants
Participants have been recruited through the network of Care4Neo. Their members include parents of patients who experienced NEC, but also parents of patients who experienced extreme preterm births without NEC or a child diagnosed with another disease early on in life. An invitation has also been shared with the parent panel of the Dutch Patient Federation. Next to this, we recruited through social media accounts of several neonatal intensive cares in the Netherlands and charity Strong Babies. Finally, we distributed posters at the University Medical Center Groningen’s paediatric nursing departments. Data recruitment for the Delphi study commenced on 23 October 2023 and concluded 10 April 2024.
Introductory survey
All registered participants will receive an invitation by email to fill out the first introductory survey. In this survey, participants are asked to provide their electronic informed consent and to provide some demographic information regarding their family situation and experiences. Based on this information, the participants will be separated into three panels to ensure that the perspectives and experiences of various groups of parents are comprehensively represented in the study:
Non-affected parents panel—parents who have not experienced preterm birth and/or NEC. Including this panel allows for gathering insights from parents who have not directly faced the challenges associated with preterm birth or NEC and might thus be less biased.
Affected parents panel—parents who have experienced preterm birth and/or NEC in their children. Their firsthand experiences offer crucial insights into the decision-making process, including the factors that influenced their choices, the challenges they encountered, and their perspectives on the care received.
Bereaved parents panel—parents who have experienced death as a result of preterm birth and/or NEC. Their experiences are unique and profoundly impactful, providing insights into the emotional, psychological and decision-making aspects of navigating these devastating outcomes.
After providing the demographic information, participants will be given the opportunity to review the initial list of decision factors and contribute additional factors based on their experiences and perspectives. The steering committee will engage in email discussions to deliberate on the proposed additional factors, aiming to reach a consensus on their inclusion before commencing the Delphi rounds.
Delphi round 1
Following the existing literature, we aim to include at least 10 participants in each panel, with a total minimum of 50 participants.37 The invitation letter to all potential participants contains a link to the first round of the Delphi study which has been developed in Qualtrics.38 In this round, participants will be presented with the list of decision factors compiled by the steering committee. Decision factors will be presented in separate categories. Participants will individually score the factors on a 9-point Likert scale, based on the perceived importance of the factor when making the decision between laparotomy or palliative care in surgical NEC, with 1 labelled as ‘very unimportant’, 5 labelled as ‘neutral’ and 9 labelled as ‘very important’. Clarifications for the terms are available in the questionnaire.
Participants will be reminded to fill in the questionnaire 1 week after the initial contact. If participants have not completed the questionnaire after 2 weeks, they will be contacted again to enquire if they are having difficulties in completing the questionnaire or if they have decided to end their participation in the study. Participants who do not complete the questionnaire within 3 weeks after the first email will be removed from the following phase to uphold data quality and to facilitate timely analysis.
Delphi round 2
The aggregated responses from all participant panels will be shared with the remaining participants, maintaining anonymity. Using this collective insight, participants will progress to the second round of the Delphi procedure, where they will have the opportunity to re-evaluate and potentially revise their scores. This iterative process aims to distill consensus among participants. Again, participants will receive a reminder after 1 week. After 2 weeks, participants who have not completed the questionnaire are asked if they require help or if they want to terminate their participation. Data collection stops 3 weeks after the first email.
Consensus definition
Consensus needs to be reached about the most important set of decision factors that is considered relevant for parents who are facing the decision between laparotomy or palliative care in surgical NEC. The steering group will meet up in a consensus meeting to evaluate the results of the second Delphi round. In particular, the results of decision factors that reached a median score of 6–9 (slightly important to very important) in at least one of the panels will be discussed and considered for inclusion in the pertinent set of decision factors. Other factors will be excluded. Depending on the scores and the professional opinions and experiences of the steering group, they will decide on the top ten to twenty factors to be included in this set.
Step 2: Q-methodology
After the pertinent set of decision factors has been determined, the steering group will convene to collaboratively formulate statements regarding these factors. This effort will include the participation of NHML, scientist in health communication and experts in communication within neonatal care. For example, if ‘learning disability’ turns out to be an important decision factor, one statement could be ‘I find it very important that my child will not have learning problems in school’. These statements will be used in the experiment to determine the parent profiles.
To do so, we will make use of the Q-methodology. This is a research technique used to study subjectivity and typologies within a group of participants.39 It involves a combination of qualitative and quantitative methods to systematically study individuals’ perspectives on a particular topic. By asking participants to rank the statements and subsequently performing a ‘by-person factor analysis’ we can learn more about the different views of parents on the decision they would have to make. With this information, we can formulate advice for the different parent decision-making profiles that can be incorporated in the final decision support tool.
Participants
We will target the same parent groups as for the Delphi study. Following the literature, we will aim to have a minimum number of 50 parents with varying experiences participating in this second part of the study.40 This target is selected with flexibility, recognising potential challenges in participant recruitment. A range of 40–60 participants is deemed pragmatic to accommodate these considerations. The participants will provide digital informed consent and demographic information in the same way as for the Delphi study. Once they have completed this part, they will receive an invitation by email to sign up for a timeslot in which they will perform the Q-sort together with a trained neonatal research nurse. Data recruitment for the Q-methodology commenced on 23 October 2023 and is expected to finish by 31 May 2024.
Experiment
At the commencement of the meeting, the research nurse will explain the procedure of the experiment to the participants. Subsequently, they will be provided with a hyperlink to the website for conducting the experiment while maintaining communication with the research nurse throughout the process. On this website, the parents are provided with a sorting grid, which is a predefined arrangement of spaces or categories. The grid will be in the form of a distribution pyramid, with a range from ‘most disagree’ to ‘most agree’. Participants read each statement and drag it to the position on the sorting grid that reflects their opinion or judgement about the statement. They may need to make trade-offs and prioritise statements based on their own perspectives. They can move the statements around and change their locations. The research nurse will remain accessible to address any questions or challenges encountered by the participants.
Analysis
The resulting data will be saved and analysed using the by-person factor analysis in order to identify underlying dimensions of factors that influence the participants’ sorting patterns. Each participant’s ranking of the statements is transformed into an array of numerical data, after which the array of one participant can be intercorrelated with the arrays of all the others. A resulting correlation matrix shows which participants are similar to others. By subjecting this matrix to factor analysis, we can obtain groupings of data arrays that are highly correlated. This determines the factors that represent clusters of participants with similar opinions (ie, profiles). Drawing from existing literature,41–50 we assume that we will observe at least three distinct parent profiles through our by-person factor analysis, in which each considers the decision factors in different ways:
Knowledge seekers: These parents are driven by the quest for comprehensive information regarding survival probabilities, potential short-term and long-term burdens for the child (including the impact of the treatment on neonate, potential physical and mental challenges, and quality of life).41–43 Furthermore, they seek insight into the effect on family dynamics considering the emotional toll on parents, repercussions on work/life balance.44
Subjective decision-makers: This group comprises parents who do not actively pursue information but rather entrust the decision-making process to their emotions. Their decisions are often influenced by factors such as religious beliefs, past experiences, a sense of hope or feelings of responsibility.45
Avoiders: This group includes parents who prefer not to take an active role in decision-making, opting instead to defer to the judgement of the physicians. While they desire the best for their child, they are hesitant to assume direct responsibility for the decision-making process.46–49
While the profiles described focus on different decision-making approaches (ie, ‘how’ parents decide), another distinction might be possible on the basis of underlying values or preferences (‘what’ is considered in the best interest of the child).50 While some parents might focus on short-term outcomes, others might prioritise the long-term well-being and future outcomes of their child; some might primarily consider their own emotions, needs and desires, while others might selflessly advocate for treatments and decisions that they believe will maximise their child’s health, happiness and quality of life, even if it means setting aside their own preferences or desires. The by-person factor analysis will reveal how we should best identify the distinct parent profiles, how many profiles should be distinguished, and whether the distinction between profiles is mostly based on the decision-making approaches, underlying values or both. It is essential for the steering committee to remain critical and open to identifying additional decision-making profiles when evaluating this by-person factor analysis.
Advice generation
For each distinct parent profile as identified by the by-person factor analysis, the steering group will draw up a tailored, comprehensive advice. We aim to employ the Ottawa Decision Support Framework as a comprehensive tool to generate tailored advice for the various parent profiles identified in our research. This framework will guide our analysis and enable us to address the unique decisional needs and preferences of each parent group.51 The goal of the advice is to provide parents with the kind of information that they are looking for. For example, if ‘information seeker’ turns out to be a profile, parents who are classified as such will mainly be presented with information on risks and benefits and the effect of clinical characteristics. Similarly, for subjective decision-makers, the advice will focus on addressing emotional and personal factors influencing their decision-making process, encouraging open communication with healthcare providers and considering the child’s best interests alongside their own feelings and beliefs. For avoiders, the advice will emphasise the importance of actively engaging in the decision-making process, seeking clarification on any concerns or uncertainties and advocating for their child’s needs and preferences, even if they may initially prefer to defer to healthcare providers. In the event that the identified parent types deviate from our initial expectations, we would need to reassess our assumptions and refine our approach accordingly. This underscores the crucial role of the steering committee in conducting thorough research into the identified parent profiles and their corresponding preferences.
Step 3: evaluation of the decision support tool
The final decision support tool functions like the website used to perform the experiment but also incorporates the advice for the different parent profiles. That is, once the user has sorted the statements, they will be classified into a specific profile and presented with the corresponding advice as drawn up by the steering group. The last part of this study will be an anonymous evaluation of the developed tool.
Participants
Once again, participants will be recruited through the previously mentioned networks. Following standard guidelines for usability evaluations, we aim to enlist a minimum of 10±2 participants for each panel.52 Using the same panels as in the Delphi procedure ensures a comprehensive representation of various experiences and perspectives. Ideally, we seek a total of at least 50 participants. Recruitment for the evaluation is expected to take place from August to September 2024.
Methods
The evaluation will be performed through an online survey in Qualtrics in which participants will be asked to engage with the decision support tool and to provide feedback on its effectiveness.38 To evaluate the user experience and usability of the decision support tool, we intend to employ a combination of the System Usability Scale (SUS) and the User Experience Questionnaire (UEQ). The SUS is a widely used questionnaire that provides a quick and reliable assessment of the usability of a system or product.53 On the other hand, UEQ is a tool designed to measure the overall user experience, capturing factors such as perceived usability, aesthetics and emotional response.54 Recognising the unique circumstances surrounding the decision-making process for surgical NEC, we will customise the survey to incorporate specific questions tailored to the context in which the decision support tool will be used. That is, by asking participants to imagine a real-world situation in which they would have to make a decision between laparotomy or palliative care for their child with surgical NEC, we can ask them to what degree the tool empowers them in making a decision between laparotomy or palliative care, and whether it facilitates communication with the healthcare professional. This adaptive approach ensures a more comprehensive evaluation, addressing not only general usability and user experience but also specific aspects relevant to the decision-making dynamics in the targeted medical scenario. By doing so, we can evaluate the alignment with the Ottawa Decision Support Framework and, consequently, assess the tool’s effectiveness in facilitating value clarification and enhancing decisional outcomes.
Analysis
Most questions in the questionnaire will be asked in the form of a 5-point Likert scale. Results will be presented as median (IQR), as customary.55 Contingency tables and χ2 tests can be used to assess interactions among answers.
Ethics and dissemination
Ethics and consent
Ethical approval has been obtained from Central Ethics Review Committee of The University Medical Center Groningen (METc 2023/577, CTc UMCG 153660). Participants will be asked to provide their informed consent for the parts of the study that involve non-anonymous data gathering.
Safety considerations
Throughout the Delphi and Q-methodology phases of the research, we will collect and analyse personal data essential for the analyses, including participants' demographic information. To safeguard participant privacy and confidentiality, all data will undergo pseudonymisation. Furthermore, demographic information will be stored separately from the research data, reinforcing the protection of participant identities. In the evaluation phase, no personal data will be solicited from participants, ensuring anonymity throughout this segment of the study. The handling and storage of data will comply with relevant regulations and guidelines governing data protection, including data protection laws and institutional research ethics policies.
Dissemination
We intend to disseminate the findings of our research through academic journals and presentations at relevant conferences. At this stage, we are evaluating potential publication venues that align with the scope and objectives of our study. Similarly, regarding the deposition and curation of research data, we are currently considering options for long-term preservation and accessibility. Further evaluation of data deposition options will be conducted as the research progresses.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank the Dutch Patient Federation, charity Strong Babies, Knowledge Center for Infant Mortality 'Stille Levens', and the NICUs of the Wilhelmina Kinderziekenhuis Geboortecentrum, Medisch Spectrum Twente Enschede and Maastricht University Medical Center for their dedication to distributing the participant invitation.
References
Footnotes
Contributors The work has been planned by RV, EMWK and JBFH. RV, EMWK, SAO-B, RG, NHML, AAEV and JBFH contributed to the conduct and reporting of the study. RV is the guarantor. OpenAI’s GPT-3 was used to assist in reviewing and clarifying the text.
Funding This work was supported by the For Wis(h)dom Foundation (Project 9, 2 February 2022) (Baarn, The Netherlands) and the Gratama-Stichting (Project 2023-02).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.