Article Text

Abstract
Introduction Research with urban refugee youth in Uganda has documented co-occurring social (e.g., poverty) and health (e.g., depression) disparities associated with HIV vulnerabilities. Benefits of HIV self-testing (HIVST) in increasing HIV testing uptake among youth are well established, yet limited interventions have examined if combining HIVST with mental health promotion, or with mental health promotion alongside poverty reduction, is associated with greater improvements in HIV prevention and testing outcomes.
Methods and analysis The aim is to evaluate the effectiveness of: (1) HIVST alone (standard of care); (2) mobile health (mHealth) and graphic medicine (comic) programme for mental health alongside HIVST; and (3) the combination of HIVST, a livelihoods programme, and mHealth mental health programme, in advancing the primary outcome of HIV testing uptake and secondary outcomes (HIV status knowledge, linkage to confirmatory testing and HIV care, HIV knowledge, consistent condom use, condom use self-efficacy, sexual risk) with urban refugee youth in Kampala, Uganda. A three-arm randomised controlled trial will be implemented from 8 April 2024 to 31 October 2024 with youth across five informal settlements in Kampala, grouped into three sites based on proximity, and randomised in a 1:1:1 design. Approximately 330 participants (110 per arm) are enrolled and data collection will occur at three time points (baseline enrolment, 3-month follow-up and 6-month follow-up).
Ethics and dissemination The study received ethical approval from the University of Toronto (#37496), Mildmay Uganda Research Ethics Committee (#MUREC-2021-41) and Uganda National Council for Science & Technology (#SS1021ES). The trial is registered at ClinicalTrials.gov (NCT06270160). Study findings will produce new knowledge of the impacts of a mental health programme, and a combined mental health and livelihoods programme, on improving HIV prevention outcomes among urban refugee youth in Kampala. Findings will be shared in peer-reviewed publications, conference presentations and in community dissemination.
Trial registration number NCT06270160 (date of registration: 13 February 2024).
Trial sponsor Dr. Carmen Logie, carmen.logie@utoronto.ca.
- MENTAL HEALTH
- HIV & AIDS
- Stress, Psychological
- Adolescents
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This trial will compare offering a mHealth-delivered mental health programme on its own versus combined with a livelihoods programme on HIV testing outcomes among urban refugee youth in Kampala.
Addressing poverty and mental health challenges alongside HIV self-testing with urban refugee youth is innovative and can advance syndemics-informed programming.
Conducting gender-stratified and age-stratified analyses will provide insight into gender and/or age differences in intervention effectiveness.
Study limitations may include attrition and potential loss to follow-up.
Introduction
By mid 2023, there were 110 million persons forcibly displaced globally, three-quarters hosted in low and middle-income countries (LMIC).1 Displaced persons experience HIV vulnerabilities that span social–ecological levels. For instance, structural-level factors include underfunded health systems in humanitarian settings and poverty-related barriers to accessing healthcare; community-level factors include intersecting stigma (e.g, refugee stigma, HIV stigma), sexual violence and inequitable gender norms; and individual-level factors include disruption of family structures, mental health challenges and transactional sex for survival needs.2–8 Knowledge gaps persist regarding efficacious approaches to increase HIV prevention and care cascades with forcibly displaced persons in LMIC, reflecting that ‘displaced populations are being neglected in efforts to end the AIDS epidemic’ (p5).8
Uganda is relevant context to address these knowledge gaps and identify targeted needs for HIV prevention, testing and care. Uganda hosts over 1.5 million refugees, over 100 000 of whom live in the urban centre of Kampala,9 often in slums or informal settlements.9–13 While HIV prevalence and testing engagement among Uganda’s refugees is uncertain due to the lack of standardised surveillance of refugees,14 a 2017 study15 in Nakivale refugee settlement in western Uganda reported an HIV prevalence of 4% among refugee adults, of whom only 54% were linked to HIV care and 6% initiated antiretroviral treatment (ART). These rates fall far below the UNAIDS goals of 95% of PLHIV receiving ART by 2030, respectively,16 signalling the need for further attention to HIV care engagement among refugees.
HIV self-testing is a promising youth-friendly strategy for increasing HIV testing uptake with youth in diverse African countries, including Zimbabwe,17 South Africa18 and Uganda.19 Innovative HIV self-testing (HIVST) delivery strategies offer promise in linking persons with positive HIVST results to confirmatory testing and HIV care.20 As such, identifying strategies to promote linkage to HIV care is essential to realise the public health impact of HIVST.21 An HIVST study in 14 communities (n=14 004) in Malawi reported that HIVST uptake among adolescent girls aged 16–19 was 100%, yet only 56% of people testing positive were linked to HIV care,22 which is far below the UNAIDS goal of 90% and 95% of PLHIV receiving ART.16 22 23 A 2014 systematic review reported a dearth of evidence-based strategies for linkage to HIV care with adolescents, highlighting the need for research focused in this age group.24 An HIVST trial with refugee youth in Kampala found increased uptake of HIV-testing and HIV status knowledge among participants in the HIVST arm (vs standard of care), and in the study arm where HIVST was combined with mHealth support, there were further benefits in reduced adolescent sexual and reproductive health stigma.25
Refugee youth in Kampala’s urban informal settlements are at the nexus of health and social vulnerabilities experienced by youth in Uganda and youth living in Kampala’s informal settlements. For instance, as of March 2021, the HIV prevalence among Ugandan youth aged 15–24 years was estimated at ~2%.26 The HIV prevalence among youth living in Kampala’s slums and informal settlements may be higher than the national prevalence, with estimates of 13.9%–37.2%.27–29 This high prevalence may be driven by food insecurity, poverty, stigma, and inequitable gender norms, which may affect many residents in slum settings.30 31 These interlinked factors can increase HIV vulnerabilities through complex pathways, including limiting safer sex negotiation, increasing transactional sex, and constraining youth engagement with HIV prevention services.27 32 For instance, research with urban refugee youth in Kampala identified associations between mental health challenges (frequent alcohol use, depression), violence (intimate partner violence, violence in young adulthood) and HIV vulnerabilities (multiple sex partners, transactional sex) that reflect a syndemic.33 Syndemics refer to interactions between social inequities (eg, poverty, violence) and health inequities.34 35 The poverty rate among refugees in Uganda worsened during COVID-19 from 44% to 50%, and employment dropped from 43% to 32%, and it is projected that recovery from the economic impacts of COVID-19 may be slower for refugees compared with Ugandan nationals.36 Other studies among urban refugee youth in Kampala have noted associations between poverty indicators and poorer health outcomes, including: food insecurity and poorer mental health37; unemployment and reduced HIV testing uptake38; and resource insecurity (food/water insecurity) and reduced sexual and reproductive health access (including HIV and STI testing)39 and transactional sex.39 40 Multilevel approaches that jointly address this convergence of poverty, mental health and HIV vulnerabilities thus offer promise to address co-occurring social and health challenges yet are understudied with urban refugee youth in low-income and middle-income settings such as Uganda.
There are persistent knowledge gaps regarding integrating mental health and poverty reduction in HIV testing and prevention with urban refugee youth in LMIC such as Uganda. The study aim is to evaluate the effectiveness of (1) HIVST alone (standard of care); (2) an evidence-based mental health programme delivered using mobile health (mHealth) and graphic medicine (comic) alongside HIVST; and (3) the combination of HIVST, a livelihoods programme and mental health programme, in advancing HIV prevention outcomes, including increasing routine HIV testing, HIV status knowledge and linkage to confirmatory testing and HIV care.
Methods and analysis
Study design
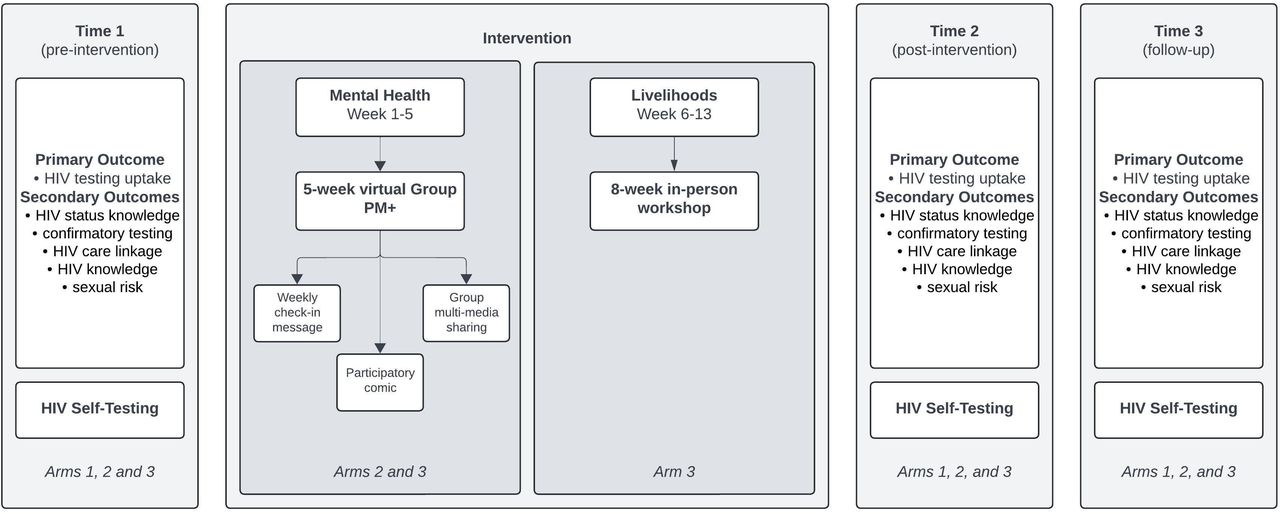
We will conduct a three-arm randomised controlled trial (RCT) to evaluate the effectiveness of HIVST delivery methods alone and combined with a mental health programme, and mental health and livelihoods programmes, among refugee youth living in Kampala41 (figure 1). Five informal settlements in Kampala where most urban refugees reside will be randomised in a 1:1:1 approach to one of the three study arms: (1) HIV self-testing; (2) HIV self-testing alongside a mental health programme; and (3) HIV self-testing, a mental health programme, and a livelihoods programme (interventions described in-depth below). Refugee youth (aged 18–24 years) living in the same informal settlements who are trained in research methods and ethics will act as peer navigators and enrol other youth in the study after obtaining written informed consent. Participants will be randomly allocated to a study arm based on their informal settlement of residence. Youth living in slums and informal settlements have shared sociophysical environments.41 As such, except for individual-level outcome data, we will use a cluster approach to analyses and programme delivery to limit challenges posed by experimental contamination and threats to internal validity. Data collection will be performed at baseline, and 3 and 6 months post-intervention implementation. The clusters will be numbered 1, 2 and 3. We will use a computer-generated randomisation list created by a trained research assistant to allocate the cluster to intervention. The number of the clusters and the randomisation list will be kept separate until it is time to implement the interventions. The trained study coordinators (FA and BK) will generate the allocation sequence, enrol participants and assign participants to interventions.

Study design for Tushirikiane-4-Uthabiti, a three-arm randomised controlled trial to evaluate the effectiveness of HIV self-testing (HIVST) delivery methods alone and combined with a mental health programme, and mental health and livelihoods programmes, among urban refugee youth living in Kampala, Uganda.
Study setting
We are conducting this RCT in five informal settlements in Kampala, Uganda. Settlements will be grouped into three arms based on close geographical proximity (1: Kabalagala and Kansanga, 2: Katwe and Nsambya and 3: Rubaga), a strategy successfully used in prior interventions with this study population.25 We used the following criteria to select informal settlements: (1) settlements that host a large number of refugees or displaced persons,11–13 42 (2) communities with similar measures of socioeconomic status, healthcare access, languages and living conditions; and (3) evidence of a high prevalence of depressive symptoms among urban refugee youth.37 43 We have previously published details on trial site location, population and geography.44
Study population and eligibility criteria
We will use an existing cohort of approximately 330 (110 participants/cluster) youth aged 16–25. Cohort eligibility includes those (1) currently living in one of the five selected Kampala informal settlements (Kabalagala, Kansanga, Katwe, Nsambya, or Rubaga); (2) who identify as a displaced person, refugee, or as having a refugee or displaced parent(s); (3) aged 16–25 years; (4) who own or have daily access to a mobile phone; (5) who speak French, English, Kirundi, Kinyarwanda, or Swahili. Participants were screened for eligibility (via phone, in person, or WhatsApp) by trained peer navigators. Self-reported HIV serostatus is not an inclusion criterion for participation; we anticipate based on our prior work with this cohort and population25 that most participants will be HIV negative, and we will collect self-reported HIV serostatus at each data collection timepoint (see the Outcome section for more detail). Youth living with HIV will not be excluded from this study.
Participant recruitment and retention
The project team includes academics, practitioners, Ugandan Ministry of Health stakeholders and a non-governmental organisation with expertise in refugee youth community engagement. Participant recruitment, study design and pilot testing will be facilitated by peer navigators, study coordinators and implementing partners. Peer navigators (12: 6 young women, 6 young men) are all experienced health/peer educators within study communities and were identified and recruited by community-based collaborators for being respected and involved within their communities.
We employed purposive methods to recruit participants, such as word-of-mouth and venue-based sampling at community events and refugee agencies, beginning with participants who belonged to the Tushirkiane cohort and participated in previous trials on HIVST,44 COVID-19 prevention45 and mental health interventions.41 We will refresh the cohort with additional purposive recruitment of 16-year-old and 17-year-old participants.
Patient and public involvement in research
This community-based study is a collaboration with Young African Refugees for Integral Development (YARID), a non-governmental youth refugee organisation in Kampala, who have been involved since the initial research question and focus development stage. We developed the study protocol after a formative qualitative research phase (phase 1), which included semistructured interviews with peer navigators and other key informants (eg, refugee health professionals, migrant workers and teen mothers). We completed four focus group discussions stratified by age and gender to explore refugee youth perspectives on livelihoods and mental health to identify key themes and prioritise the health needs of urban refugee youth.
Intervention description
We designed an RCT consisting of three arms: (1) HIVST, (2) HIVST+ mental health mobile health (mHealth) (bidirectional SMS and WhatsApp discussions) program and (3) HIVST+ mental health mHealth program + Creating Futures (standardized livelihoods training program). Data will be collected at baseline, and 3 and 6 months post-intervention implementation. All study arms will receive HIVST kits at each data collection timepoint. All participants will meet with trained research assistants at the three time points. Unique study identification (ID) numbers on coupons will be used to track HIV testing access and linkage to HIV and sexual and reproductive health services care. If a participant requests, they can discontinue the allocated intervention.
Arm 1: HIVST
Participants will be provided with HIVST instructions and education from peer navigators, who will also emphasise the importance of receiving a confirmatory test irrespective of HIV positive result. At each timepoint, participants will receive an HIVST package (OraQuick Rapid HIV‐1/2 Antibody Test, OraSure Technologies) with written and pictorial instructions and a referral sheet for confirmatory testing. Peer navigators will demonstrate how to use the HIVST kit, including how to (1) open the kit, (2) collect the oral fluid samples, and (3) read the results. In addition to HIVST education, participants will be offered optional pretest counselling and SMS contact information to connect with their peer navigator. If participants do not want post-test counselling, the PN will follow up within 2 weeks. If the participants report testing HIV positive, then they will be immediately scheduled for confirmatory testing and enrolled in the support programmes at the Uganda Ministry of Health Most at Risk Population Initiative (MARPI) Clinic for young people living with HIV led by study coapplicant and coauthor (PK). If participants report being HIV positive after enrolment (prior to the intervention), we will similarly refer them to the MARPI clinic resources.
Arm 2: HIVST and mental health mobile health (mHealth) program
Participants in this arm will be enrolled into the HIVST intervention (as described above in arm 1) as well as a mental health programme delivered using mobile health (mHealth) and participatory comics. We will adapt and implement, using mHealth and participatory comic approaches detailed below, the WHO Program Management Plus (PM+) scalable, low-intensity brief psychological intervention that is transdiagnostic and developed for delivery by lay persons to address a range of common mental health challenges and adversities.46–49 PM+ has been adapted for delivery across settings,50 and during formative work for this specific intervention the study team adapted PM+ materials into all languages for delivery, and worked with the Peer Navigators to produce key messages from PM+ for delivery by mHealth and participatory comics (below). The four key strategies shared during PM+ are stress management, problem-solving, behavioural activation and strengthening social support, and an additional relapse prevention (staying well)48 (figure 2). PM+ has also been adapted for group delivery (Group PM+) and digital delivery (step-by-step (SbS)), to increase access and help with cost saving.48 PM+, including Group PM+, participation was associated with reduced psychological distress, anxiety, depression, problems and post-traumatic stress with adults in Kenya46 and Nepal51 and Syrian refugees in the Netherlands.52 A systematic review and meta-analyses of 23 studies implementing PM+ and SbS reported effects on reducing distress and promoting positive mental health and called for additional evidence.53

Overview of the 4-key strategies in the adapted Problem Management Plus mental health programme and the themes delivered using mobile health (mHealth), including WhatsApp group discussion, bidirectional SMS, and participatory comics.
In Uganda, over 13 million persons have access to mobile phones, and data suggest that HIV prevention messages through mobile phones are beneficial to supplement traditional modalities such as schools for adolescents.54 55 This reflects calls to integrate technology into health interventions with refugees/displaced persons.3 56 SbS was an online self-help intervention with minimal guidance that aimed to adapt PM+ for digital delivery, yet focused on the behavioural activation strategy as the problem management strategy required more facilitator support.57 To overcome this challenge and address all PM+ strategies, we are using (in addition to the participatory comics described below) a multistep mHealth delivery strategy that includes (1) weekly SMS check-ins moderated by the peer navigator; (2) weekly themed informational SMS to share PMP messages for each weekly strategy, and accompanying questions to enhance engagement; and (3) WhatsApp group multimedia sharing and discussions of participatory comic responses with peer navigators. The peer navigator and coordinator will review group discussions weekly to incentivise engagement; (4) participatory comic books: an adapted PM+ comic book, outlining problem management strategies and solutions across each of the four strategies and the relapse prevention strategy. We are collaborating with the WelTel non-profit agency for the implementation of the supportive SMS intervention.58–61 The WelTel system will manage the SMS intervention on their structured mobile phone platform (all SMS interactions are logged). Weekly two-way supportive messages will automatically be sent on the same weekday with WelTel software to mental health programme participants (arms 2 and 3). The peer navigator will ask mental health programme participants to respond to the SMS within 48 hours to confirm their well-being and will follow up with non-responders. The peer navigators and Research Coordinator will access the server every 24–48 hours to triage and respond to participants who express a problem or need, including referral to the project social worker based at the collaborating agency.
The participatory comic delivery includes providing a combination of PMP written and pictorial content and including one page of educational information and the second page with blank spaces for participants to write their answers in, as our team has done in prior research.62–65 Educational comics offer a youth-friendly, low-cost, scalable approach for providing education and health promotion on health topics such as HIV, sexually transmitted infections, vaccines and dementia.66–68 Comics have been used to educate both the general population and healthcare providers to improve care and patient experiences, as they are accessible, do not require high levels of literacy and can encourage participants to envision and share solutions through facilitating dialogue around emotionally difficult and often stigmatised issues.69–74
Arm 3: HIVST and mental health mHealth and livelihoods programme
In addition to HIVST and the mental health mHealth programme, participants in arm 3 will also be in enrolled in an 8-week Creating Futures programme. Creating Futures is a group intervention that aims to help young people build their livelihoods and was designed for use with youth (18–24) in urban informal settlements in South Africa.75 A key intervention aim is to address livelihood insecurity and gender inequality with the end goal of reducing HIV-related risks. Previous researchers have implemented the Creating Futures intervention in South Africa and found that after the intervention, men’s earnings increased, women’s experiences of intimate partner violence decreased, men and women scored better on gender attitudes, and depression and suicidal thoughts decreased among men.76 This manualised programme was developed with youth in South Africa and adapted for the Kenyan context.77 78 Topics within the Creating Futures programme include: (1) introduction and situating self; (2) sustainable and social resources; (3) peer group meeting; (4) education and learning; (5) getting and keeping jobs; (6) income generating activities; (7) saving and coping with shocks; (8) reflection and looking ahead (figure 3). This intervention aims to help participants think about, and plan for, their futures to assist them in making a living in the long term. Each workshop will be conducted in-person, for approximately 3 hours and will be facilitated by pairs of peer navigators. Our team met with the peer navigators on this planned study to adapt some aspects to fit the Kampala context, and found that the structure, and most materials, were relevant for participants in this study.

{kind=link}
{kind=link}
{kind=link}
Overview and key themes of the 8 week adapted creating futures livelihoods programme, that aims to help young people build their livelihoods. NA, not applicable.
Outcomes
Primary outcome
The primary outcome measured in this trial is routine (every 3 months) HIV testing uptake as a measure of HIV prevention. Participants will be asked to self-report when their last HIV test occurred and where it was received (i.e., HIVST, clinic and point of care).
Secondary outcomes
The secondary outcomes of this trial include (1) HIV status knowledge, (2) confirmatory testing, (3) HIV care linkage, (4) HIV knowledge and (5) sexual risk. We will document antiretroviral therapy (ART) adherence for those who seroconvert during the study using a three-item self-report scale.79
Knowledge of HIV status
Since HIV status is self-reported, we will use multiple steps to overcome challenges of social desirability bias. First, interviewers will ask participants to report their current HIV status at 3 and 6 months follow-up surveys. Second, the trained interviewer will offer participants a voluntary rapid HIV test at the final survey (6-month follow-up). Knowledge of HIV status will be assessed as correct for participants who agree to take the rapid test and correctly report their HIV status. We will also record if participants were willing to take the interviewer-administered rapid test. Linkage to confirmatory HIV testing: participants will be asked if they used their HIVST kit at 3 and 6 months follow-up surveys. For those who affirm use of HIVST kits with a positive test result, we will ask if and where they received a confirmatory test. Participants can receive confirmatory testing without reporting to the interviewer and can submit coupons at MARPI or to local clinics. Linkage to HIV care: we will ask participants who seroconvert during the study to report the frequency of HIV care services. In addition, participants can present coupons when accessing MARPI or local clinic services. HIV knowledge: we will use an 18-item Brief HIV Knowledge Questionnaire to assess HIV knowledge.80 Sexual practices that elevate HIV exposure: we will assess sexual risk through self-reported measures of consistent condom use (anal, vaginal sex) with regular, causal and paid sex partners in the past month, as well as the number of sex partners in the past month, condom use self-efficacy81 and selling sex in the past 3 months.
Sample size and power analysis
A parallel, three-group cluster-randomised design will be used to test the difference among the three proportions that is defined by the contrast coefficients −2, 1, 1. The comparison will be made using a generalised estimating equation (GEE) logistic model Z-test with a type I error rate (α) of 0.05. The autocorrelation matrix of the responses within a cluster is assumed to be compound symmetric with an intraclass correlation coefficient of 0.013. Missing values are assumed to occur completely at random (MCAR), and the anticipated proportion missing is 0.05. To detect the group proportions 0.5, 0.75, 0.75, with contrast coefficients −2, 1, 1, with a total of three clusters (allocated to the three groups as 1, 1, 1), with an average cluster size of 110 subjects per cluster (for a total sample size of 330 subjects), the power is 0.80. The power was computed using PASS 2024, V.24.0.2.
Data collection and management
Data collection will be conducted by research assistants trained by the Ministry of Health in pretest and post-test counselling. We will collect data using a structured survey accessed via mobile phones or tablets in all study languages via the SurveyCTO app (Dobility). This app houses a secure platform and automatically encrypts data, which are then uploaded with a Secure Sockets Layer certificate to a password-protected server. The use of SurveyCTO allows for multilingual and offline data collection with branching logic and consistency checks. All participants are assigned a unique ID number without any personal identifying information to enhance confidentiality. All datasets will be saved on a password-protected server that can only be accessed by study staff on a need-to-know basis for data management and outcome reporting.
Data analysis plan
The analysis and reporting of this study will be conducted following the Consolidated Standards of Reporting Trials (CONSORT) guidelines.82 The study analyst will be blinded to group allocation. Participant flow (screening, randomisation, allocation and follow-up) will be illustrated using a CONSORT flow diagram. We will report baseline data for all groups summarised using mean (SD) or median (first and third quartiles) for continuous variables and counts and frequencies (per cent) for categorical variables. For this study, we will use an intention-to-treat approach with a complete data set whereby participants will be analysed according to their initial group allocation irrespective of whether they received said intervention.
We will conduct a between-group comparison using GEE models, treating the intervention group as a fixed effect. To specify a GEE model for our binary categorical outcomes, we will employ a binomial distribution with a logit link function and select an appropriate working correlation structure (exchangeable) to address the within-cluster correlation of observations.83
Model fit will be evaluated using the quasi-likelihood under the independence model criterion (QIC). This approach enables us to analyse the relationship between the predictors and the binary outcome while providing robust estimates that account for clustering in our data.84 The significance level will be set at alpha=0.05 for the primary outcome to ensure sufficient power for our analysis and to test a prespecified hypothesis. For the secondary outcomes and subgroup analyses (by gender), we will employ a Bonferroni adjustment to mitigate the increased risk of type I error associated with multiple comparisons.85 86
Results will be presented as ORs or mean differences as appropriate, with corresponding 95% CIs and p values. For the primary outcome (HIV testing), we will conduct an adjusted analysis using GEE to investigate the influence of covariates on the relative effect. We will then perform an economic evaluation using the intention-to-treat approach to assess how much the average costs and primary outcome differ between each intervention group and the control group through estimation of the incremental cost-effectiveness ratio (ICER) given as [(Cost of intervention)−(Cost of control)]/[(Success of intervention)−(Success of control)].
We will perform an economic evaluation using the intention-to-treat approach to assess the differences in average costs and primary outcomes between each intervention groups. This will involve estimating the ICER, calculated as [(Cost of intervention) − (Cost of control)]/[(Effectiveness of intervention) − (Effectiveness of control)]. The economic analyses, conducted from the health system perspective, will include outcomes and costs in the trial’s time horizon. We will use a graphical plane to present the cost-effectiveness ratio for each outcome, and bootstrapping techniques will be used to estimate cost-effectiveness ratio CIs.
Ethics and dissemination
Ethical considerations
The Tushirikiane Phase 2: HIV self-testing study protocol has been approved by the Research Ethics Boards University of Toronto (July 22, 2022, #37496), Mildmay Uganda Research Ethics Committee (13 March 2023; #MUREC-2021-41) and Uganda National Council for Science & Technology (29 February 2024; # SS1021ES). The trial is registered at ClinicalTrials.gov (NCT06270160), which we will inform should there be modifications from the protocol. We will audit trial by conducting data queries at 1 month post intervention starting, 3 months and 6 months; the process will be conducted by a trained data analysis and independent from investigators and the sponsor.
We developed the protocol for the study under the Standard Protocol Items: Recommendations for Interventional Trials Statement.87 Our study population consists of young adults aged 16 years and older who can provide informed consent for HIV testing in Uganda without parental involvement (at the age of 12 and above), and we received research ethics approval to allow youth aged 16–17 to participate in the trial without parental consent to reduce barriers to participation in sexual health research.88 89
All participants will receive information about the study prior to enrolment and will be informed of their rights to refuse or withdraw from the study, as well as understand study processes and expectations. Participants will be given sufficient time to provide their voluntary written consent and all informed written consent processes will occur in a private room at a location provided by YARID. Participants or peer navigators will read consent forms (online supplemental file 1) themselves in a language comfortable to them (French, English, Luganda, Kirundi, Kinyarwanda or Swahili). Consent forms (signed via signature or thumbprint) will not be connected to data collection and will be destroyed 5 years after study completion. Participants can withdraw from the study at any time during study data collection before interview completion and will be informed that there are no adverse consequences to their care or health service delivery if they choose to withdraw. Data will be stored on password-protected and secure servers and all participants will be given a unique ID to maintain confidentiality. Only study investigators will have access to the final trial dataset per research ethics board approval for working with vulnerable populations (refugees).
Supplemental material
Peer navigators and counsellors trained in psychological first aid90 will be on-site throughout the intervention and participants will be provided with a list of community resources, although interventions are not expected to cause psychological distress. Peer navigators will report any adverse events to research assistants, who will then fill out an Adverse Event Reporting Form and Adverse Event Narrative Form if appropriate; participants can leave the study at any time, including if having experienced adverse events. Participants can also directly report adverse events to YARID or the study team. All adverse events require a narrative form to be sent to the principal investigators within 24 hours. There will be no Data Safety and Monitoring Board (DSMB) as this is a low-risk intervention largely involving methods the team has already implemented with this population (HIV self-testing, group problem management plus), and YARID (RH and BK) has a long history of livelihoods interventions with this population; thus, there is no need for a DSMB or interim analysis.
Data sharing and dissemination
The final data set will be shared between the Uganda-based and Toronto-based research teams using a secured, encrypted and password-protected system. Users entered under a data-sharing agreement and secure research ethics approval via a research ethics board amendment with the University of Toronto will be able to access the final deidentified data set. Findings will be shared in peer-reviewed publications, conference presentations and with community dissemination.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge all of the peer navigators and participants, as well as collaborating agencies: Young African Refugees for Integral Development (YARID), Ugandan Ministry of Health, Office of the Prime Minister, Most At Risk Populations Initiative (MARPI), and International Research Consortium (Kampala).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @carmenlogie
Contributors CHL is the guarantor. Study design: CHL, MO, RH and LM. Data management: LT, FM, ZA, RH, DKM, BK and AN. Manuscript writing: CHL, LT, FM and LM. Manuscript editing: MO, ZA, RH, DKM, BK, AN and PK.
Funding The study was funded by the Canadian Institutes of Health Research (CIHR: WI3- 179958). Logie was also supported by the Canada Research Chairs Program. Funders played no role in study design, collection, management, analysis and interpretation of data; writing of the report; or the decision to submit the report for publication; they will not have ultimate authority over any of these activities.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.