Article Text

Abstract
Introduction Hepatitis C virus (HCV) infection is a silent epidemic that needs a comprehensive and contextualised approach to manage. Access to readily available, affordable and acceptable HCV point-of-care (POC) in vitro diagnostics (IVDs) is equally required to meet the global HCV goals. However, most guidelines for evaluating these IVDs such as the WHO prequalification process and country-specific standards disproportionately focus on diagnostic performance. The real-time connectivity, ease of specimen collection, affordability, sensitivity, specificity, user-friendliness, rapidity and robustness, equipment-free or simplicity and deliverability to end-users (REASSURED) criteria provide a holistic and user-oriented evaluation of the IVDs in the populations they are meant to be used. Therefore, as part of a multinational study in sub-Saharan Africa, we will conduct an evaluation of the Bioline HCV POC test for diagnosing HCV infection in primary healthcare settings of Ghana using the REASSURED criteria.
Methods and analysis This field evaluation will be conducted in three phases. The first phase will use a cross-sectional field evaluation study design to evaluate the diagnostic performance of the Bioline HCV POC test. The second phase will use mixed methods to ascertain operational characteristics and users’ perceptions. In the third phase, a cross-sectional survey will be used to estimate the costs of accessing HCV diagnostics services using three proposed HCV testing models to inform the affordability of the testing pathways and linkage to care in the primary healthcare clinics. This phase will run concurrently with the second phase of the study. Thematic content analysis and quantitative data analysis will be performed using ATLAS.ti V.23.0.6 and StataCorp LLC’s Stata statistical software V.16.0, respectively.
Ethics and dissemination The study protocol has been reviewed and fully approved by the Faculty of Health Sciences Research Ethics Committee, University of Pretoria (281/2023) and the Ghana Health Service Ethics Review Committee (GHS-ERC013/08/23). This diagnostic trial has also been registered in the Pan African Clinical Trial Registry (PACTR202410837698664). The findings of the study will be presented in relevant peer-reviewed journals, at local and international conferences, and to all stakeholders involved.
- PUBLIC HEALTH
- Hepatology
- INFECTIOUS DISEASES
- Epidemiology
- Diagnostic microbiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
A systematic and multiphase approach using both laboratory-led and user-oriented field evaluations will demonstrate holistic evaluation of the Bioline hepatitis C virus point-of-care (HCV POC) test.
The minimum required sample size will be used as demonstrated by respective sample size formulae.
The deployment of mixed methods in the second phase will ensure robust data collection to adequately ascertain operational characteristics and users’ perceptions of the Bioline HCV POC test.
As the study is designed purposely to evaluate the Bioline HCV POC test in sub-Saharan African population, the researchers do not intend to generalise the study outcomes. However, the study outcomes will be comparable to similar outputs in the subregion as part of a multicountry study.
Similarly, the researchers do not intend to generalise the HCV prevalence to be generated from the study as the target populations will be used for test evaluation purposes only.
Introduction
Hepatitis C virus (HCV) infection remains a public health menace and contributes significantly to the global burden of liver disease and complications including hepatocellular carcinomas.1–5 Known as a silent epidemic in most global settings, 50%–80% of people living with HCV infection are oblivious to their status.6 7 Annually, 1.5 million new cases are reported with more than 290 000 deaths.8 Of the 130–150 million cases of HCV recorded worldwide in 2017,9 10 over 58 million people progressed to chronic HCV and 13% treated as of 2019.8 11 Existing literature highlights specific vulnerable groups to HCV infection due to their circumstances of sharing spaces and potentially sharing sharp objects like razor blades and needles. These groups include incarcerated individuals, people who use or inject drugs, those who engage in unsafe tattoo practices, as well as men who have sex with men.12–14 HCV infection traverses most WHO member regions with 12 million recorded cases each in the Eastern Mediterranean and European regions, 10 million each in South-East Asia and the Western Pacific regions, and 5 million in the Americas as of 2021.8 However, sub-Saharan Africa (SSA) contributes 2%–5% of the global HCV burden with over 200 000 deaths annually.4 15 16 This is substantially associated with inadequate testing and linkage to care due to poor or no access to cheaper diagnostics particularly in hard-to-reach and resource-limited communities.17 18
The global narrative around medical diagnosis is progressively shifting towards rapid diagnostics testing at point-of-care (POC).19–24 This was heightened during the peak of COVID-19, which met high advocacies for the implementation of self-testing and near-bedside testing.25–30 Similarly, the WHO’s goal is to make HCV diagnosis closer and more accessible to hard-to-reach communities using POC diagnostic assays,11 thus linking most viral hepatitis cases to care to reduce viral hepatitis deaths by 65%, and new viral hepatitis infections by 90% by 2030.8
Ghana, like most SSA countries, battles with HCV infection with seroprevalence ranging between 1% and 3%.5 31 32 Arguably, this burden is expected to be disproportionately higher if expanded community-based HCV testing is implemented at POC. This will improve HCV awareness, and boost test uptake and coverage amidst the sizeable hard-to-reach communities that lack access to simple, robust, affordable and user-oriented HCV diagnostic services. Unlike HIV and hepatitis B, HCV diagnosis in Ghana is founded on the over-reliance on screening tests using rapid in vitro diagnostics (IVDs) with little or no attention paid to confirmatory testing.5 33 34 Moreover, these screening tests have been relegated to blood donors due to poor public awareness.35 Confirmatory testing may be outsourced to private-owned laboratories and research institutions since no public health facility in Ghana is equipped to reliably offer confirmatory testing for HCV.5 This development comes with huge cost implications that promote health inequalities among the poor and hard-to-reach communities who solely rely on primary healthcare (PHC) clinics.17 18 36 To meet the HCV POC diagnostic needs of Ghana’s Health system and to improve the HCV diagnosis in the country, there is the need for a reliable diagnostic that can serve its intended purposes.
Several HCV POC IVDs have received different regulatory approvals notably the WHO prequalification (PQ) process and others are ‘Conformité Européenne’ (CE) marked.34 However, the majority of these tests’ clinical trials did not include African populations, disproportionated in high-income settings and easy-to-reach communities and were largely evaluated on laboratory-based clinical performance.34 The Bioline HCV test, manufactured by Abbott Diagnostics, includes products (02FK10, 02FK16, 02FK17) that have met the WHO Prequalification process (PQDx 0257-012-00), are CE marked and are registered for use in Ghana by the Food and Drugs Authority (FDA) (FDA/D.21–11702).37 38 Using the Bioline HCV POC IVD as a case test, this study seeks to evaluate the test based on quality indicators within the Ghanaian health system, particularly in PHC clinics and among the Ghanaian population. The multiphased evaluation will be conducted using the real-time connectivity, ease of specimen collection, affordability, sensitivity, specificity, user-friendliness, rapidity and robustness, equipment-free or simplicity and deliverability to end-users (REASSURED) criteria. This criteria is a revised version of the affordable, sensitive, specific, user-friendly, rapid and robust, equipment-free or simple and deliverable to end-users (ASSURED) criteria adopted by the WHO/Tropical Diseases Research in 2006.39 40 The update was made to incorporate technological advancements in POC diagnostics after a decade of implementing the original ASSURED criteria.
Methods
Study design
This study will employ varying study designs to evaluate the Bioline HCV test based on specific components of the REASSURED criteria. In a three-phased approach, the study will be rolled out to address three specific study objectives with each phase addressing each objective. The first phase will use a cross-sectional field evaluation study design to evaluate the diagnostic performance of the Bioline HCV POC test. A mixed method study approach will be employed to ascertain users’ perceptions of the Bioline HCV POC test in terms of real-time connectivity, ease of specimen collection, equipment-free or simplicity and user-friendliness in the second phase of the study. To be run concurrently with phase 2, the final phase will use a cross-sectional survey to estimate the costs of accessing HCV diagnostics services using three proposed HCV testing models to inform the affordability of the testing pathways including Bioline HCV POC test and linkage to care in the PHC clinics. Laying foundation for this work, a comprehensive narrative review, was conducted and published elsewhere to shape the study objectives in this protocol.34 This review summarised the standard regulatory requirements and quality assurance for HCV POC testing in SSA including Ghana. Recommendations for future studies towards evaluating the accessibility, affordability and user-oriented application were made.
Study setting
The study will be conducted in Ghana. More specifically, the study will be conducted in the Central region, one of the 16 administrative regions of Ghana.41 The Central region is considered one of the smallest regions in Ghana with a land area of about 9826 square kilometres.42 Specifically, in phase 1 of the study, three HCV target populations will be recruited from two study settings, including the Ankarful prison, and the Cape Coast Teaching Hospital both in the Cape Coast Metropolis. During phases 2 and 3, data will be drawn from a total of 70 PHC clinics in three districts, thus Komenda-Edina-Eguafo-Abirem, Cape Coast, and Mfantseman out of the 414 PHC clinics in the Central region.43 44 The selection of the prison was informed by the existing literature that underscores the risk factors associated with confined environments and the sharing of sharp objects. This includes incarcerated individuals, people who use or inject drugs, and those involved in unsafe tattoo practices.12 45 46 The PHC clinics play a crucial role as the first point of contact for local communities, providing essential medical services such as preventive care, treatment for common illnesses, vaccinations, chronic disease management and health education. In contrast, the teaching hospital serves as a referral tertiary facility for smaller health facilities within and outside the Central region of Ghana, providing emergency services, special clinics, and blood banking facilities.
Conceptual framework
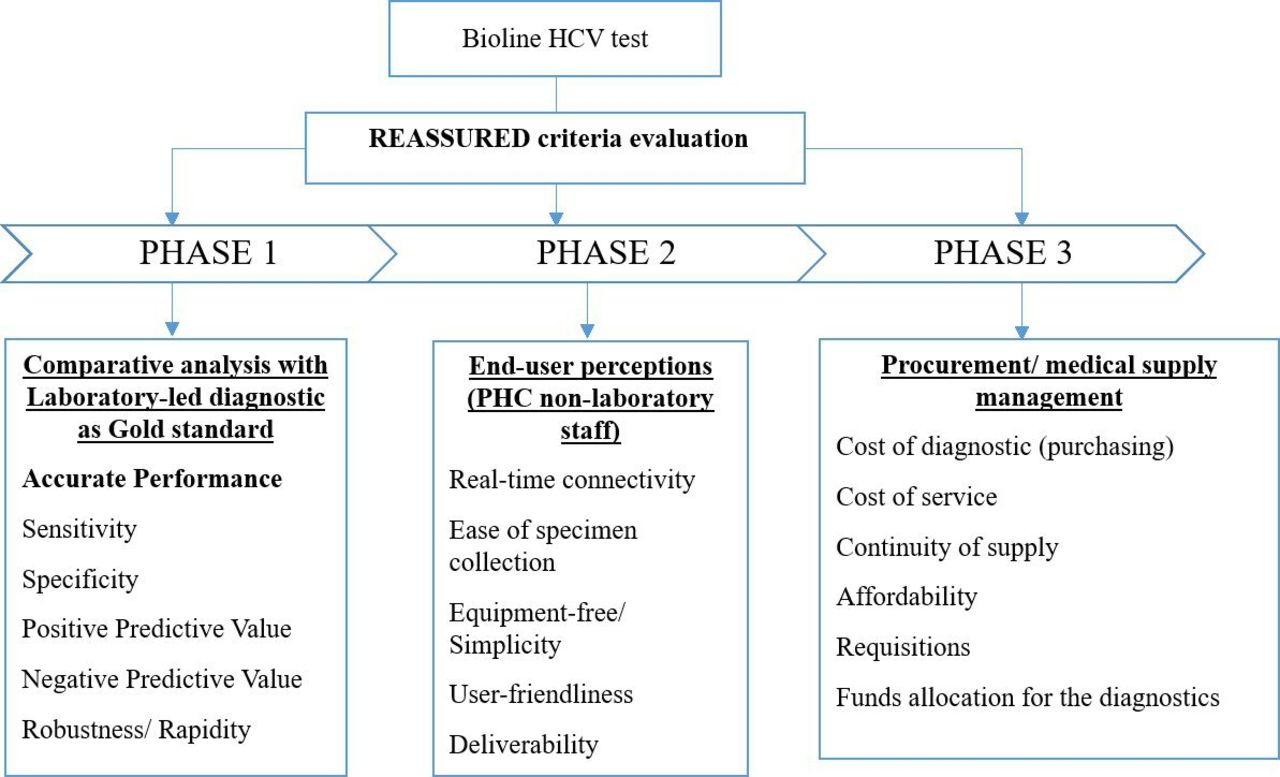
Figure 1 gives a framework that describes the relational connection between key concepts and variables towards evaluating the Bioline HCV test using the REASSURED criteria.39 This framework guides the three-phased evaluation study under the broader building blocks of performance evaluation, user perceptions and cost-effectiveness indicators in a unidirectional flow. The first phase of the study will address the first research objective, thus evaluating the diagnostic performance of the Bioline HCV test against a laboratory-led HCV reference test (the Fortress Diagnostics qualitative HCV kit, using the sandwich ELISA test principle and to be run on the ChemWell Fusion Automatic Immunoassay Analyzer). This objective will use standard statistical indicators for evaluating the accurate diagnostic performance of POC tests.47 This includes estimating the sensitivity, specificity, positive predictive value, negative predictive value and robustness or rapidity of the tests involved. The second phase seeks to assess the perceptions of the non-laboratory staff in the PHC clinics in using the Bioline HCV test. This objective will, through in-depth interviews, collect data on user perceptions concerning real-time connectivity, ease of specimen collection, equipment-free or simplicity, and user-friendliness. Finally, the third phase will follow the step-by-step guidelines for disease-specific costing, payments, affordability and linkage to care metrics in low and middle-income countries.48 49

Conceptual framework for evaluating the Bioline HCV point-of-care testing using the REASSURED criteria. HCV, hepatitis C virus; PHC, primary healthcare; REASSURED, real-time connectivity, ease of specimen collection, affordability, sensitivity, specificity, user-friendliness, rapidity and robustness, equipment-free or simplicity and deliverability to end-users.
Phase 1: comparative analysis
Objective 1: to evaluate the diagnostic performance of the Bioline HCV POC test
Design: Cross-sectional field evaluation study.
Study population: incarcerated individuals, patients with a Clinician’s request for HCV test and voluntary blood donors with a request for predonation screening.
Sampling: a sample of the study population calculated by Buderer’s formula for diagnostic studies will be obtained using the convenience sampling technique.50 A total required minimum sample size of 433 will be used for the study, thus 399 and 34 for sensitivity and specificity analysis, respectively assuming a 10% non-response rate.
Sensitivity

 =minimum sample size for estimating sensitivity,50
=minimum sample size for estimating sensitivity,50
Z = standard normal deviate for a given level of significance (α), here α=5%, Z=1.96,
 = predetermined sensitivity of Bioline HCV=99.3%,38
= predetermined sensitivity of Bioline HCV=99.3%,38
d=level of precision or marginal of error for the sensitivity=5%,
Prev=predetermined prevalence of HCV in Ghana=3%5


Assuming a 10% non-response rate


Specificity

 =minimum sample size for estimating specificity
=minimum sample size for estimating specificity
Z =standard normal deviate for a given level of significance (α), here α=5%, Z=1.96
 =predetermined specificity of Bioline HCV=98.1%38
=predetermined specificity of Bioline HCV=98.1%38
d=level of precision or marginal of error for the specificity=5%
Prev=predetermined prevalence of HCV in Ghana=3%5


At a 10% non-response rate


The convenience sampling technique will be used to obtain a sample of the study population. This non-probability sampling technique will permit all consenting participants to be included in the study.
Data collection and testing: at the Ankarful prison, a medical screening programme will be rolled out by the principal investigator (PI) and research assistants, including a team consisting of a medical doctor, two medical laboratory professionals, a disease control officer, and a nurse. This will also include pretest counselling, post-test counselling and linking all positive cases to care at the Cape Coast Teaching Hospital. A paper-based structured questionnaire will be administered by the PI and the research assistants to collect non-identifiable demographic information (online supplemental file S1). A study-specific venous blood sample will be collected in a 5 mL gel separator tube and a 4 mL EDTA tube by the medical laboratory professionals. The study-specific blood collection tubes will be processed according to the study work instructions and standard operating procedures at the Cape Coast Teaching Hospital Laboratory. The medical laboratory professionals will use the whole blood sample in the EDTA tube for the Bioline HCV POC testing, while the serum sample obtained by centrifuging the gel separator tube will be used for the reference testing. Additionally, at the Cape Coast Teaching Hospital Laboratory, freshly collected whole blood and serum samples from patients with a clinician’s request for HCV testing, as well as from voluntary blood donors requiring predonation screening, will be obtained by the medical laboratory professionals. These blood samples, along with non-identifiable demographic information of the patients and donors (online supplemental file S1), will be catalogued, provided informed consent (online supplemental file S2) is obtained. Whole blood samples will be tested using the Bioline HCV POC test. Reference testing will be performed using the Fortress Diagnostics qualitative HCV kit on the ChemWell Fusion Automatic Immunoassay Analyzer. This kit detects serum HCV antibodies (Anti-HCV) using a microplate qualitative chemiluminescence immunoassay based on the sandwich ELISA principle.
Supplemental material
Supplemental material
Inclusion criteria
At the Ankarful Prison, all incarcerated individuals who consent to be screened will be included in the study.
At the Cape Coast Teaching Hospital, all patients with a Clinician’s request for HCV test and voluntary blood donors with a request for predonation screening who give informed consent will be included in the study.
Exclusion criteria
At the Ankarful Prison, a participant will be considered ineligible for this study if:
Participant withdraws consent for study participation.
Inadequate venous whole blood samples are obtained.
Participants who are ineligible will be withdrawn from the study and may be replaced at the discretion of the sponsor and PI.
Data analysis: the paper-based data will be manually entered into an Excel spreadsheet, cleaned and imported into StataCorp LLC’s Stata statistical software V.16.051 for further statistical analysis. Descriptive statistics will be performed for the general distribution of data followed by performance analysis for diagnostic tests. This will estimate the sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, negative likelihood ratio, Youden index and test efficiency of the Bioline HCV POC test with corresponding 95% CI as defined in table 1. In addition, the Kappa coefficient of concordance between the Bioline HCV POC test and the ELISA test will be estimated.
A 2×2 contingency table for evaluating diagnostic performance








Outcome measures: diagnostic performance of the Bioline HCV POC test.
Phase 2: end-user perceptions
Objective 2: to ascertain users’ perceptions of the Bioline HCV POC test in terms of real-time connectivity, ease of specimen collection, equipment-free or simplicity and user-friendliness
Design: Mixed methods study
Study population: all non-laboratory clinical staff of PHC clinics in the Komenda-Edina-Eguafo-Abirem, Cape Coast, and Mfantseman districts.
Sampling: a representative sample of the study population will be obtained using simple random sampling technique guided by the Cochrane sample size formula.52 However, the PHC clinics will be selected conveniently until the minimum required sample size is obtained. A minimum required sample size of 428 will be used for the quantitative study assuming a 10% non-response rate.

n=minimum sample size52
Z=Standard normal deviate for a given level of significance (α), here α=5%, Z=1.96
P=Predetermined user perception. A 50% good perception of the usability and acceptability of the Bioline HCV test is assumed since there are no published data on this subject in Ghana.
d=level of precision or marginal of error for the specificity=5%


Assuming a 10% non-response rate


Also, the minimum required sample size for the qualitative component will be set at 20 in-depth interviews until data saturation is reached. These study participants will be selected purposively from the 428 non-laboratory clinical staff for the qualitative study.
Data collection: in the quantitative study, the PI and research assistants made up of two medical laboratory professionals will train the study participants on how to use the Bioline HCV POC test, guided by the manufacturer’s instruction for use. The PI and research assistants will demonstrate how the test is used while observing all required safety protocols including wearing of a pair of gloves. The study participants will be observed and evaluated by the PI and research assistants with a paper-based standardised checklist (online supplemental file S1) while performing the test on each other in pairs in private rooms and results documented. The checklist will document errors and difficulties faced by the study participants and also indicate where assistance will be requested while performing the test. This checklist will cover the pretesting (preanalytical) processes, analytical processes (performing the test) and postanalytical processes (reading, reporting interpreting results). These will include pretesting: (1) reading the test instruction on the information sheet or test leaflet, (2) removing the test device from the foil pouch, (3) placing the test material on a flat surface and opening all pouches and caps and (4) washing hands in warm water, drying and wearing gloves. Testing: (5) correctly choosing the ring or middle finger, (6) massaging and warming the finger, (7) cleaning the finger with an alcohol swab and letting it dry, (8) pressing down firmly to prick the skin, (9) safely discarding the lancet, (10) wiping away the first drop of blood with tissue and rubbing it to create a second large drop of blood, (11) collecting the drop of blood with the specimen dropper, (12) dispensing the whole blood into the round specimen well (marked S’), (13) applying plaster, (14) twisting and pulling the cap to open the assay diluent, (15) dispensing all the assay diluent tube into the square well of the device and (16) timekeeping for results. Post-testing: (17) reading and interpreting the results, (18) safely discarding the used test kit and (19) retesting/attempting to retest if invalid results are obtained. The tests will be repeated and equally documented by a research assistant to determine the interoperator and inter-reader concordance of the tests. Additionally, the participants will be randomly given one of two known standard samples labelled A or B, which will be blinded from the study participants, to perform the Bioline HCV test. Similarly, the results will be documented and compared with the standard results to assess the interoperator and inter-reader concordance of the tests.
Concurrently, the study will explore the users’ experiences and acceptability of the Bioline HCV test using qualitative methods. In-depth interviews will be conducted with 20 study participants purposively sampled, using a semistructured interview guide (online supplemental file S1). The interview guide consists of questions that seek to explore participants’ personal experiences and perceptions about the use of the test. These include questions about their overall hands-on experience, confidence, usability and reliability of the manufacturer’s test instructions; challenges, ease of sample collection, quality assurance, real-time connectivity, simplicity or equipment-free, deliverability, improvement areas and recommendations. The interviews will be conducted in English and are anticipated to last 45 min per participant. The interviews will be audio-recorded, and field notes will be taken to supplement the recorded interviews.
Inclusion criteria
Non-laboratory consenting personnel of the targeted PHC clinics will be allowed an opportunity to participate in the study.
Exclusion criteria
A participant who withdraws consent (online supplemental file S2) for study participation will be excluded from the study.
Laboratory personnel will be excluded from the study.
Data analysis: the audio-recorded files will be transcribed into Word documents, and thematic analysis will be performed on the qualitative data to identify relevant themes from the end-user perception evaluation. This analysis will be conducted by importing the Word documents into ATLAS.ti qualitative data analysis software, V.23.0.6.53 The paper-based quantitative data will be manually entered into an Excel spreadsheet, cleaned and imported into StataCorp LLC’s Stata statistical software V.16.051 for statistical analysis. The general distribution of the data will be established by descriptive measures. The usability or user-friendliness of the Bioline HCV POC test will be measured by the observed errors recorded and difficulties faced by the study participants when using the POC test as recorded on the study checklist. These will be computed and presented in absolute frequencies and percentages as proportion with 95% CI. Interoperator and inter-reader concordance of the test will be estimated as percentage agreement between the test results as reported and interpreted by the participants and the research assistants. Cohen’s kappa coefficient will be estimated. Statistical significance exists at p<0.05. Results will be presented in tables, graphs and quotes.
Outcome measures: usability or user-friendliness of the Bioline HCV POC test as well as interoperator and inter-reader agreement results of the test.
Phase 3: comparative cost evaluation
Objective 3: to estimate the costs of accessing HCV diagnostic services using proposed HCV testing models to inform the affordability of the testing pathways
Design: cross-sectional survey
Study population: financial units of the PHC clinics and referral laboratories in the Komenda-Edina-Eguafo-Abirem, Cape Coast and Mfantseman districts.
Sampling: using Yamane’s sample size formula, a minimum required number of 60 PHC clinics will be sampled simple randomly from the 70 profiled PHC clinics in the three districts.52

where:
N=the total number of PHC clinics in the districts under study is 70.52
e =margin of error=5% =0.05 at 95% CI.



Data collection: a decision tree approach will be used to test three HCV testing models in the selected districts (figure 2). The testing models are made up of phases that represent varying testing strategies and algorithms. The PI and trained research assistants will use a paper-based questionnaire to collect data on the cost composition of various phases of testing decisions in each testing model thus:
Using no HCV testing algorithm at the PHC clinic hence resorting to referrals.
Using PHC clinic’s (brand withheld) HCV POC test and referring for confirmatory testing.
Using the Bioline HCV POC test at the PHC clinic and referring for confirmatory testing.

{kind=link}
{kind=link}
HCV testing models (decision tree). HCV, hepatitis C virus; PHC, primary healthcare.
The cost of service chart at each PHC clinic and referral laboratory will be requested. The cost implications of the Bioline HCV POC test will be compared with that of the available testing algorithms in the testing models.
Model 1 will establish the cost of transport to the referral laboratory for the HCV test+the cost of anti-HCV testing at the referral laboratory+cost of transport back to the PHC clinic+cost of transport to the Central Laboratory for confirmatory test+type and cost of confirmatory test+cost of returning to the PHC clinic with confirmatory test results.
Model 2 will determine the cost of the anti-HCV test at the PHC clinic+the cost of transport to the Central Laboratory for confirmatory testing+the type and cost of the confirmatory test+the cost of returning the confirmatory test results to the PHC clinic.
Model 3 will inform the proposed cost of Bioline HCV POC test at the PHC clinic+type and cost of confirmatory test+cost of returning confirmatory test results to the PHC clinic. PHC clinics that have laboratories and laboratory staff will be excluded from the study.
In addition, the PI and research assistants will collect data on estimated distance to the referral and central laboratories; and payment methods will be accepted by the referral facilities (out-of-pocket or insured).
Inclusion criteria
The following will be included in the study:
PHC clinics within the three districts under study.
Referral laboratories provided by specific PHC clinics (if any).
Exclusion criteria
PHC clinics that have laboratories and all laboratory professionals will be excluded from the study.
Data analysis: the paper-based data will be manually entered into an Excel spreadsheet, cleaned and imported into StataCorp LLC’s Stata statistical software V.16.051 for statistical analysis. Descriptive analysis will be performed to demonstrate the general distribution of data such as the cost distribution among the testing algorithms and models under study. Mean and its associated standard deviation (SD) and median and its associated interquartile range (IQR), whichever appropriate will be used to summarise the data. The cost composition comparing the three testing models will be established by calculating the total cost for each model. All statistical results will be presented in tables and graphs.
Outcome measures: cost implications of the Bioline HCV POC test.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design of this study. However, study participants will be actively involved in the conduct of the study, reporting and dissemination of the study outcomes. Participants will be engaged in data collection processes, including using the Bioline HCV POC test and providing feedback on their experiences. Regular feedback sessions will be organised to discuss preliminary findings and gather input on data interpretation. Participants will have the opportunity to review study results during facility visits before finalisation and publication, ensuring their perspectives are considered. Workshops will be held for participants to share their experiences, and findings will be disseminated accordingly. Participants will be acknowledged in the acknowledgement section of all three publications for their contributions to the study.
Study timeline
Data collection is anticipated to be carried out between September 2024 and February 2025. The objective 1 is set to begin in September 2024 and the objectives 2 and 3 will run side-by-side starting in October 2024. The entire study is projected to be completed within 1 year.
Ethics approval
This diagnostics trial has been registered in the Pan African Clinical Trial Registry (PACTR202410837698664). The study has received full approval from the Faculty of Health Sciences Research Ethics Committee, University of Pretoria, South Africa (Reference number: 281/2023). Additional full approval has been given in Ghana by the Ghana Health Service Ethics Review Committee (Reference number: GHS-ERC013/08/23). Written permission has been obtained from the Ghana Prison Service’s Headquarters for data collection at the Ankarful Prison. Similarly, written permission has been obtained from the laboratory management of the Cape Coast Teaching Hospital for the performance evaluation phase.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualisation: ED, EMM, TPM-T. Methodology: ED, EMM, TPM-T. Project administration: ED. Supervision: RKDE, EMM, TPM-T. Validation: TPM-T. Writing—original draft: ED. Writing—review and editing: ED, RKDE, EMM, TPM-T. Guarantor: ED.
Funding This study has received product and financial support from Abbott Rapid Diagnostics as part of Abbott’s Investigator Sponsored Studies (ISS).
Competing interests EMM declares that he is employed by Abbott Rapid Diagnostics as a Scientific Affairs Manager for Africa and a co-supervisor to Evans Duah. He, therefore, acknowledges that he is aware of his responsibility to take the necessary steps to take reasonable steps to avoid any potential or perceived conflict of interest during his co-supervision duties in this study. Moreover, as a co-supervisor, his contribution and decisions will be reviewed and approved by TPM-T, the main supervisor of the study. All authors declare no other conflict of interest.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.