Article Text

Abstract
Introduction Amyotrophic lateral sclerosis (ALS) is a fatal neurogenerative disease with no effective treatment to date. Despite numerous clinical trials, the majority of studies have been futile in their effort to significantly alter the course of the disease. However, these studies may still provide valuable information for identifying patient subgroups and generating new hypotheses for future research. Additionally, synthesising evidence from these studies may help overcome the limitations of individual studies. Network meta-analysis may refine the assessment of efficacy in specific patient subgroups, evaluate intervention characteristics such as mode of administration or biological mechanisms of action, and rank order promising therapeutic areas of interest. Therefore, we aim to synthesise the available evidence from ALS clinical trials.
Methods and analysis We will conduct a systematic review to identify all clinical trials that assessed disease-modifying pharmaceutical therapies, cell therapies, or supplements in patients with ALS. Outcomes of interest are clinical disease progression outcomes and survival. We will conduct this search in the period Q4 2024 in three databases: PubMed, Embase and ClinicalTrials.gov for studies from 1999 to 2023. Individual patient data and aggregate data will be collected and subsequentially synthesised in meta-analytical models. The final model will be presented as an open-source web application with biannual updates of the underlying data, thereby providing a ‘living’ overview of the ALS clinical trial landscape.
Ethics and dissemination No ethics approvals are required. Findings will be presented at relevant conferences and submitted to peer-reviewed journals. Data will be stored anonymously in secure repositories.
- systematic review
- network meta-analysis
- neuromuscular disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This network meta-analysis and living review will centrally synthesise all randomised clinical trials in amyotrophic lateral sclerosis investigating disease-modifying therapies.
Retrieved studies will be screened with a validated machine-learning tool (ASReview) and through predefined eligibility criteria.
Specific efforts will be made to disentangle the effects of study-level characteristics including mode of administration and mechanism of action, and quantify heterogeneity in treatment responses.
The main challenges for this study will be the potential unavailability of individual patient data and large between-study differences in trial design, which will be partially addressed through the hybrid use of patient-level and aggregate data.
Introduction
Amyotrophic lateral sclerosis (ALS) is a rare and fatal neurogenerative disease which is characterised by the loss of motor neurons and progressive muscle weakness followed by death within, on average, 3–5 years after symptom onset.1–3 Although over 100 clinical trials have been conducted in the last 25 years,4 treatment options remain limited with no substantial improvement in the patient’s life expectancy.5 The futile clinical trial landscape is the result of an interplay of various elements including, but not limited to, a weak a priori study rationale; underestimation of the pathophysiological and clinical heterogeneity; and a suboptimal or flawed study design.4
By combining the results and outcomes of previous clinical trials, it may be possible to improve the design and conduct of future studies.6 This has been demonstrated by initiatives such as the Pooled Resource Open-Access ALS Clinical Trials or the Answer ALS database,7 8 which have been of significant value for characterising the natural history of ALS. These data sets provide key input for sample size calculations, eligibility criteria, and overall trial design considerations.9 Current initiatives are, however, lacking data on the received experimental treatment and individual studies are not identifiable. This limits the value of the data as key therapeutic questions such as subgroup efficacy10 or the impact of intervention characteristics, such as mode of administration and patient burden,11 cannot be addressed.
Hence, study-level evidence synthesis may improve the use of the available data. Moreover, it provides an opportunity to study between-trial variability12 and overcome limitations of individual clinical trials. By combining all clinical trials into a network, that is, network meta-analysis (NMA), information can be jointly harvested across studies through direct and indirect study comparisons.13 This approach yields increased statistical power to detect trends that may not be observed in single studies.14
From the network, head-to-head intervention comparisons can be made to rank order interventions based on their treatment effects and to identify areas of therapeutic interest where more research is needed. This would be of particular value for large drug screening platforms such as HEALEY,15 Motor Neuron Disease-Systematic Multi-Arm Adaptive Randomised Trial,16 and the EXPErimental medicine Route To Success in ALS as it may provide insight for investigating new therapeutic leads.17
The increased precision may be of particular interest to potentially identify subgroups of responding patients in otherwise futile clinical trials. Especially in smaller studies, efficacy signals in a small subset of patients may be lost when there is a large group of non-responders.10 The value of such a meta-analytical approach has been shown previously for lithium carbonate.18 A potentially responding subgroup was identified for patients homozygous for the c-allele of the UNC13A gene which is under investigation in a confirmatory study.19
Another area of interest is trial-related factors, such as mode of administration or mechanism of action. The significance of the former was recently highlighted for intravenous therapies where a potential procedural risk of prolonged intravenous administration may have had a negative impact on the patient’s prognosis, potentially jeopardising patient safety and confounding study results.20–22 A meta-analytical approach to the latter may reveal that groups of treatments sharing a common biological mechanism are more efficacious on certain outcomes or for specific subgroups. As these trial-related factors are applicable to all patients within a single study regardless of randomised treatment allocation, they cannot be assessed within a single study; meta-analytical models are needed to investigate their impact.
In this study, therefore, we aim to systematically identify all completed randomised clinical trials (RCTs) in ALS and synthesise their evidence through a comprehensive NMA, thereby improving the utilisation of existing clinical trial information and augmenting current large data initiatives. The final NMA model will be presented as an open-source web application with biannual updates of the underlying data to provide a ‘living’ overview of the ALS clinical trial landscape and serve as a tool for trial design, information dissemination and generating new hypotheses.23
Objectives
The primary objective of this study is to perform an NMA and synthesise the available data from RCTs, to enable the creation of efficacy rankings to identify potentially responding subgroups, and to generate new hypotheses for future research.
Subobjectives include: (1) conducting a systematic review of RCTs in ALS that evaluate disease-modifying drugs, cell therapies, or supplements; (2) obtaining and combining aggregate and individual patient data (IPD) from each study; (3) developing a network meta-analytical model; and (4) disseminating the findings through an open-source web application with biannual updates of the underlying data.
Methods and analysis
The protocol was designed based on principles outlined in The Cochrane Handbook for Systematic Reviews of Interventions and the Centre for Reviews and Dissemination’s Guidance for Undertaking Reviews in Healthcare.24 25 Due to the nature of this study, patients or the public were not involved in its planning.
Search strategy
The aim of the search is to identify phase II and III RCTs for ALS that assess the efficacy of disease-modifying therapies. In brief, we will search PubMed, Embase and trial registries (ClinicalTrials.gov, European Union Clinical Trials Register and ANZCTR), employing a prespecified search string developed in conjunction with information experts from the University Medical Center Utrecht (UMCU). The search string for PubMed and Embase includes terms for ‘ALS’ and ‘trial’ and sets a publication date filter from 1999 to the present. In ClinicalTrials.gov we will search for ALS trials conducted within the same time frame. The databases will be searched in the period Q4 2024. The full search term is included in online supplemental table I. Two reviewers will deduplicate and independently cross-reference the search output. As a last step, the references of included studies and any systematic reviews found in the search will be screened for additional eligible studies not found in the database search (snowballing).
Supplemental material
Screening process
The eligibility of each study will be determined by applying the inclusion and exclusion criteria for the title/abstract with ASReview (section 2.3).26 Subsequently, the remaining studies will undergo a second screening process by applying the inclusion and exclusion criteria for full-texts (section 2.4). All studies will be screened by two reviewers, after which the results will be compared and discussed until consensus is reached. If no consensus is reached, a third reviewer will be consulted. The number of excluded studies and the reasons for exclusion will be recorded in figure 1.

Flow diagram of study selection. After study completion, the number (n) of studies selected at each step will be indicated in each box. The dotted line represents the reference screening in the included studies for those studies not found in the database search. ALSFRS-R, the revised Amyotrophic Lateral Sclerosis Functional Rating Scale; VC, slow or forced vital capacity.
Types of studies
RCTs consisting of two or more comparative arms are eligible. The control group may be treated with a placebo, sham, another therapeutic intervention, or usual care. To ensure the inclusion of phase II and III RCTs, the total randomised sample size must contain at least 20 patients with ALS and the randomised treatment period must not be shorter than 12 weeks. The treatment period is defined as the time from blinded treatment initiation until the last follow-up or the commencement of an open-label extension period. We chose to exclude phase I studies as the sample sizes are too small and the follow-up duration is too short to allow investigation of efficacy. Larger phase Ib/IIa may be eligible if they fulfil the inclusion criteria. Moreover, phase IV trials are excluded as new drugs are added on to standard of care rending it not feasible to randomise a comparative trial of the standard of care versus a new drug. Clinical trials with deviating designs such as a single-arm, crossover, or externally controlled design are excluded alongside studies with an open-label extension unless they are preceded by a randomised treatment period of at least 12 weeks. Multistage trials are eligible if at least one stage fulfils the inclusion criteria.
Types of interventions
Interventions can be classified as either disease-modifying (eg, slowing of clinical progression rate) or symptomatic (eg, drug therapy for sialorrhoea, depression or pain).27 The primary interest of this review is disease-modifying interventions and the following types of interventions will be considered: (1) pharmaceutical interventions, (2) cell therapies, and (3) supplements (if intended to be disease-modifying). Studies that evaluate symptomatic treatments will be excluded. Studies investigating devices, dietary interventions other than supplements (eg, high-caloric intake), or physical activity programmes will also be excluded.
Types of outcomes
The outcomes of interest are measures of clinical disease progression and overall survival. Eligible outcomes include functional rating scales (eg, the revised ALS Functional Rating Scale (ALSFRS-R)), lung function (eg, slow or forced vital capacity (VC)) and survival (either defined as death alone or as a composite, for example, with respiratory insufficiency (non-invasive ventilation ≥16 hours/day) and/or tracheostomy).
Study population
Eligible patient populations are patients diagnosed with ALS according to the (revised) El Escorial, Awaji, or Gold Coast criteria.28 Studies enrolling patients before 1999 will be excluded as thereafter riluzole was introduced as a new standard of care and the revised version of the ALSFRS which more adequately measures respiratory involvement was adopted.29 30
ASReview for study selection based on title/abstract
ASReview is a machine-learning tool that increases screening efficiency by presenting the title and abstract of studies most similar to eligible ones.26 The ASReview process starts with a manual preselection of eligible and ineligible studies. To achieve an informative preselection set, these studies are heterogeneous in terms of intervention and publication date. The preselected studies can be found in online supplemental table II. Eligibility for the title/abstract screening and (systematic) review screening will be based on the selection criteria listed in table 1. The selection process continues until a stopping criterion has been reached, which will be defined as 100 consecutive ineligible studies.26 Five per cent of the unseen studies will be randomly sampled to examine whether any eligible studies have been missed. If so, the screening process will recommence until the stopping criterion has been reached.
Selection criteria for title/abstract screening
Full-text criteria
The studies found to be eligible in ASReview will undergo a full-text screening. The final set of selection criteria based on the eligibility described in sections 2.2.2–2.2.5 is listed in table 2. These criteria are slightly stricter than the title/abstract criteria as they finalise the set of included studies.
Full-text screening inclusion and exclusion criteria
Data extraction
Aggregated data (AD) of key study characteristics and outcomes will be extracted from all included studies while corresponding authors will be approached for IPD via e-mail. For the studies where IPD collection is not feasible, the analysis will proceed using only the available AD from the respective study. We strive to send out data request in autumn 2024. We will assume the author is uninterested if no reply has been received after 90 days unless other reasons for inaccessibility arise. We will extract AD in Q4 2024 after the database search and study inclusion has been completed.
AD of interest includes general study information, baseline data (eg, age, treatment group size, ALSFSR-R at baseline), intervention data (eg, name, mode of administration, treatment duration), and outcome data (eg, hazard ratios, ALSFRS-R change from baseline, p values). Online supplemental tables III and IV contain the complete list of essential IPD and AD variables that will be extracted from the studies. Online supplemental table V contains the code list for the AD variable extraction.
Data management
IPD will be collected in compliance with local regulations and under the supervision of a database manager appointed at the UMCU. All aggregate and patient-level data will be stored securely at the servers of the UMCU. Access to patient-level data will be restricted to authorised staff; costs of the data storage will be covered by the UMCU.
Statistical analysis
The primary aim of the analysis is to synthesise the available individual patient and aggregate data from all included RCTs and evaluate the efficacy of each intervention. As IPD will likely not be available for every study, we will employ network meta-analytical techniques for synthesising IPD and AD.
In brief, efficacy of the interventions will be evaluated as follows. First, we will estimate the overall efficacy of ALS treatments by conducting a random-effects pairwise meta-analysis for the ALSFRS-R, VC and survival outcome data to determine whether any treatment provides benefits compared with placebo.31 We will pool the AD from the different active treatment arms into one group and compare the pooled group to all pooled patients who received placebo.32
Second, we will employ a random-effects NMA model. The utilisation of NMA offers several advantages including the ability to (1) compare interventions that have not been performed in previous studies;33 (2) obtain more precise estimates compared with pairwise meta-analysis through direct and indirect comparisons;34 and (3) establish a ranked order or hierarchy for each investigational intervention based on their efficacy.35 The statistical model consists of a two-stage approach to combine the AD and IPD.36 37 As our objective is exploratory and hypothesis-generating, a standard 95% CI will be employed to display treatment effect estimates. Missing data in any of the covariates will be addressed by multiple imputation.38
We will conduct sensitivity analyses by restricting the model to include only studies where IPD are available, studies within the same class of mechanism of action (with classes delineated by Mead et al),39 studies that are at low risk of bias, or have total sample sizes ≥50 patients. To further investigate the impact of different classes of mechanisms of action, we will perform IPD network meta-regression. This will allow us to assess the differential effects associated with each class category and enable us to simultaneously account for and analyse the variability across different classifications providing a comprehensive understanding of the effects of the class of mechanism of action on the outcomes of interest.40
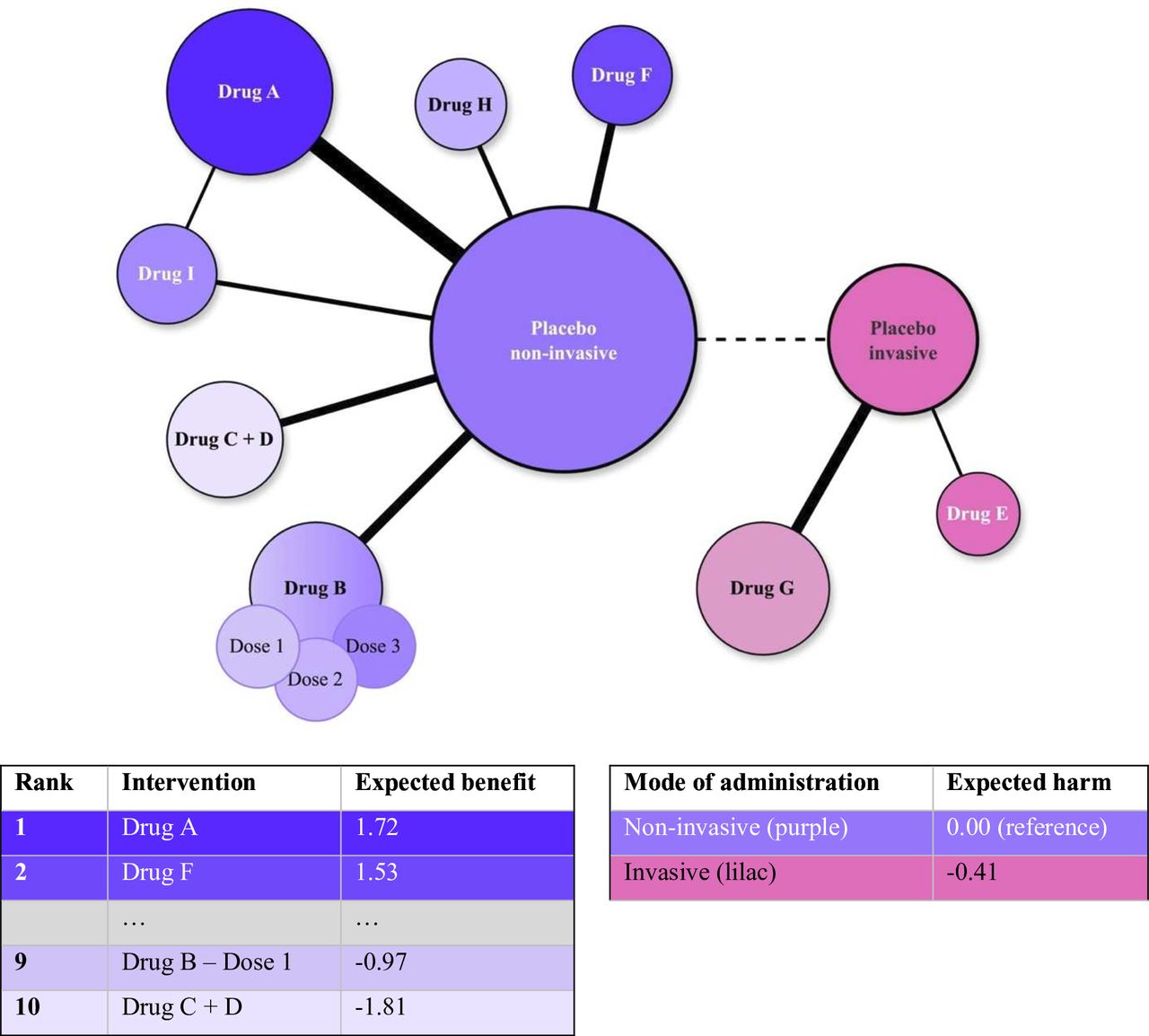
Finally, the network structure will be visually presented through a network plot while the output of the NMA model will be presented through forest plots, league tables, and tables displaying ranking metrics such as P-scores.41 A demonstrative network plot and table with ranking metrics is provided in figure 2.

{kind=link}
{kind=link}
Hypothetical network diagram and harm/benefits table. The figure above represents a hypothetical network. The network consists of intervention and placebo nodes (grouped per administration mode) while the solid lines connecting them indicate direct comparisons. Non-invasive nodes consist of oral and transdermal, while invasive nodes consist of intravenous, intrathecal, intramuscular, and subcutaneous modes of administration. The dashed lines reflect ‘disconnected’ networks that are reconnected through matching and propensity score methods. The table ranks the interventions based on their expected benefit compared with placebo as well as the expected harm of administration modes estimated through matching.
Addressing heterogeneity
Heterogeneity in an essential principle when synthesising data from different sources as it may bias results when improperly accounted for. The random-effects NMA model was chosen to address between-trial variability and heterogeneity in study populations, outcomes, and results. We will employ covariate adjustment and matching through propensity scores based on key prognostic characteristics (as defined by Westeneng et al)42 to address differences in patient characteristics. Additionally, we will conduct subgroup analyses (among for example, bulbar patients or fast-progressors) to determine which factors might modify the treatment effect, identify sources of outcome variability, or whether outcome variation may be caused by potentially random confounding factors.
Moreover, matching also allows us to ‘reconnect’ networks. Networks may be ‘disconnected’ as a result of differences in a study-level variable such as mode of administration.43 This connection allows us to explore the effect of mode of administration by comparing the pooled placebo groups of, for example, invasive versus non-invasive modes. Furthermore, outcomes may be measured differently (eg, change from baseline, mean difference, % reduction). To ensure comparability, the ALSFRS-R and VC will be recalculated as monthly decline during the randomised period. A monthly rate of decline is chosen as it is time independent and allows the pooling of results from studies with varying lengths of follow-up. Survival will be amalgamated among studies that share the same event definition and are expressed as a hazard ratio.
Heterogeneity in the model will be explored by visually inspecting forest plots and through the global assessment of the Q-statistic. Moreover, it will be quantified with the metrics τ2 and I2 estimated with the restricted maximum likelihood method. I2 denotes the percentage of variability due to heterogeneity rather than chance while a large value of I2 coupled with a relatively large estimate of τ2 signifies the presence of heterogeneity. If substantial heterogeneity is detected, it will be further explored through network meta-regression and subgroup analyses. These methods help identify potential sources of heterogeneity by examining the influence of study-level and patient-level characteristics.
A key assumption of NMA is that of transitivity which refers to the ability to infer through indirect evidence. A violation of transitivity threatens the validity of the NMA findings. To statistically evaluate transitivity, consistency will be used as a proxy. The presence of a notable difference between direct and indirect evidence signifies the presence of inconsistency which may mask the presence of heterogeneity. Network consistency will be tested both globally and locally. Global methods test whether the network is inconsistent as a whole while local methods identify inconsistent network comparisons. Global assessment of inconsistency includes the integration of inconsistency factors in the inconsistency detection process and the use of between-designs Q-statistic under the full design-by-treatment interaction random-effects model while local assessment involves the use of node-split methods.44–46
Quality assessment
We will assess the quality of the included studies in two ways. Initially, the short version of the revised Cochrane risk-of-bias tool for randomised trials will serve as a framework for summarising the risk of bias in five domains, namely: randomisation process; deviations from intended interventions; missing outcome data; outcome assessment; and selective reporting. Each domain will be rated as ‘low risk’, ‘some concerns’, or ‘high risk’, and an overall score will be determined. Second, the quality of the evidence in the individual studies will be assessed with the Grading of Recommendations Assessment, Development, and Evaluation approach. This method evaluates the outcomes of each study and determines how closely the estimated effect approximates the true effect and is rated on a 4-level scale from ‘very low’ to ‘high’. The outcomes of both assessments will be summarised and presented in a figure. Lastly, the Confidence in Network Meta-Analysis framework will be used to display bias, coherence, and heterogeneity in the evidence found and aid in the transparent reporting of the NMA.47
Living NMA model framework
Ultimately, the output of the NMA model will be presented as an interactive, open-source web application using the R package Shiny.48 A standardised operating procedure will be developed for routinely updating the NMA model including biannual reviews of the literature to identify new studies and a pipeline for IPD data requests, and to update the data analysis models accordingly. This will create a ‘living NMA model’ that could potentially serve as a perpetual overview of the clinical trial landscape of ALS and an interactive environment to support trial design.
Expected challenges and considerations
One of the potential challenges of this study is the acquisition of IPD, especially from industry-sponsored studies due to intellectual property restrictions. This was the main reason for the proposed statistical framework as it is flexible and could use both IPD as well as AD from the published literature. Hence, the missing IPD can be supplemented with AD, which may limit the impact on the main study objectives. Naturally, IPD will be required for subgroup analysis—especially for those subgroups that are not commonly reported—and to overcome ‘disconnected’ networks as a result of, for example, differential modes of administration.
Other limitations of the network will be primarily driven by the limitations of the underlying study quality and available data. These will be evaluated with the tools outlined in the Quality assessment (section 2.8).
Patient and public involvement
This study protocol has been initiated without prior patient involvement. However, the rationale for undertaking it is deeply rooted in patients’ urgent need for better disease-modifying treatment for this relentless and rapidly progressing disease. The topline results of this study will be disseminated to patients via communications from the Dutch ALS Foundation.
Ethics and dissemination
This study will meta-analyse previously collected anonymised data sets. No ethics approvals are necessary for the initiation of this project. An overview of all included studies will be provided as well as an overview of the search procedure. The AD data set will be made available on reasonable request to the corresponding author. The IPD data sets will not be made publicly available due to personal data protection considerations.
The findings obtained in this project will be presented at relevant ALS conferences (eg, The European Network for the Cure of ALS and Motor Neurone Disease Association conferences) and submitted to peer-reviewed scientific journals. In addition, as previously stated, the NMA model will be presented as an open-access web application to aid in dissemination.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @rpavaneijk
Contributors FTvL, GS, SN and RvE drafted the protocol. FTvL and RvE developed the search string and criteria. FTvL and IB will be involved in screening and data collection. FTvL, GS, DM, DW, JvU, LHvdB, SN and RvE are involved with revisions. FTvL, GS, DM, SN and RvE will be involved in developing the statistical framework. FTvL, GS, SN and RvE will be involved in data analysis and manuscript writing. RvE is the guarantor. All authors have read and approved the final protocol. ChatGPT has been used in the following ways: To find synonyms (‘academic synonyms for: …’)—To diversify word use (‘list me 10 alternatives for: furthermore’). SN and RvE are joint last authors.
Funding Stichting ALS Nederland (Project EVIDENCE).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.