Article Text

Abstract
Objectives To assess the feasibility and acceptability of delivering Healthy Eating and Active Lifestyles for Diabetes (HEAL-D) Online.
Intervention HEAL-D Online—a 7-week culturally tailored type 2 diabetes educational programme delivered using online platform.
Setting Programme delivered by a London NHS trust, with patients referred from primary care healthcare professionals via a central booking system.
Participants 53 HEAL-D service users completed a postcourse questionnaire, and 14 service users and 7 service delivery staff participated in interviews.
Design Mixed methods service evaluation.
Primary and secondary outcomes Service user engagement, acceptability and perceived patient benefit assessed using service activity data. Feasibility and acceptability of HEAL-D Online, using semi-structured interviews to explore the views and experiences of service users and service delivery staff.
Results Service activity data showed that initial uptake of HEAL-D Online was good (62% attendance) with a high adherence to the programme (77% completion). A high fidelity (94%) was observed, and qualitative findings showed that staff and service users were satisfied with all aspects of course delivery. Both service activity and qualitative data indicated that attendees felt more confident in controlling their diet and managing their diabetes post-HEAL-D Online.
Conclusion This evaluation demonstrates the feasibility of delivering HEAL-D using an online platform, with its ability to achieve similar goals compared with its face-to-face counterpart. Challenges were identified around the identification, recruitment and referral of eligible patients into the programme, which need to be addressed for successful implementation on a wider scale.
- implementation science
- general diabetes
- feasibility studies
- primary prevention
- qualitative research
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The mixed methods, pragmatic design enabled the rapid gathering of insights and identification of practical barriers and enablers to implementation, while delivering maximum benefit to service users.
A key strength was the co-design and delivery of the study, which brought together a collaboration between researchers, professionals working in the National Health Service and people from African and Caribbean communities with a lived experience of diabetes.
A limitation is the absence of a control group and the use of routinely collected data, which means the evaluation is unable to determine causation or effectiveness.
Introduction
Type 2 diabetes (T2D) is a major health concern for the UK Caribbean and African population with prevalence estimated to be three times higher,1 onset 10 years earlier2 and poorer health outcomes compared with white Europeans.3–5 Compared with other population cohorts, uptake of self-management programmes, which are recommended as a core component of management, is low in African and Caribbean communities.6 To address these ethnic inequalities in diabetes healthcare access and outcomes for UK African and Caribbean communities, a culturally tailored 7-week T2D educational programme, Healthy Eating and Active Lifestyles for Diabetes (HEAL-D) (heal-d.org), was co-designed.7 HEAL-D was originally designed for face-to-face delivery, and feasibility studies have shown that it is highly acceptable to participants.8
The COVID-19 pandemic disproportionately affected minoritised groups,9 making it essential to maintain services that address health inequalities within these groups. The associated lockdown restrictions required service providers to reconfigure how health programmes were delivered, leading to the development of online delivery for services that were previously conducted face-to-face. HEAL-D Online is one such service, using the same approach and content as the original face-to face programme but delivered through an online platform. HEAL-D Online consists of seven 2-hour sessions of group-based, culturally tailored education, behaviour change support and participatory physical activity. The sessions are delivered by a lay educator of black British ethnicity and a diabetes specialist registered dietitian (who does not have a specific ethnicity). Additionally, physical activity classes, delivered by exercise instructors trained in rehabilitation exercise, are included in five of the sessions.
This paper presents an evaluation of the feasibility and acceptability of delivering the HEAL-D Online service using an online platform delivered by the National Health Service (NHS) in South London. The evaluation aimed to examine the following factors: (i) acceptability to service users; (ii) feasibility to staff delivering the online programme; (iii) feasibility of digital participation for service users; (iv) potential benefits to service users following participation; (v) potential future improvements to HEAL-D Online.
Methods
Setting
The evaluation focused on the delivery of HEAL-D Online, a programme managed and delivered by an NHS trust in London, UK. Patients could be referred by healthcare professionals in primary care via a central booking system.
Procedure
A detailed description of the procedures is provided in the published protocol.10 This was a prospective, pragmatic, mixed methods service evaluation, using service activity records, service user questionnaires, observational data and interviews. Service activity records and responses from a postcourse telephone questionnaire were used to assess service user acceptability of HEAL-D Online, along with the feasibility of using digital technology and potential patient benefits. Qualitative descriptive methods were used to explore the perspectives of service users and service delivery staff regarding HEAL-D Online. Service user interviews were used to explore reasons for acceptability, thoughts on using digital technology, perceived benefits of HEAL-D Online and suggestions for future improvements. Additionally, both service delivery staff interviews and observational data were used to assess the feasibility of delivering HEAL-D Online.
Quantitative methods
Data on service engagement—that is, attendance rates, did not attend (DNA) rates and completion rates—were collected by the service provider for anyone attending the HEAL-D Online programme between January and December 2022.
In addition, a postcourse questionnaire was administered by the service provider over the phone as part of routine care (online supplemental appendix i). The questionnaire collected data on the following outcomes:
Supplemental material
Patient benefit assessed via perceived weight loss and diabetes-related psychological distress. This was measured pre-attendance and post-attendance using the validated Problem Areas In Diabetes (PAID-5) questionnaire,11 where score of ≥8 indicates distress.
Acceptability of HEAL-D Online for service users (expectations met, satisfaction with delivery, accessibility issues, recommendation to others). This used questions co-developed by the service provider and the study team with input from service users, and was non-standardised.
Service users’ expectations of HEAL-D Online. Following a recommendation by the reference group, a question was added once the evaluation had started, asking participants whether HEAL-D Online met their expectations. As 21 service users had already completed the postcourse questionnaire, only 32 participants were able to answer this question.
Qualitative methods
Interviews
Of the 53 who completed the postcourse telephone questionnaires, 15 service users provided consent to be approached for interview. To ensure ethical procedures were followed in recruiting participants for the qualitative interviews, these service users were first contacted via an introductory email by the evaluation team (JTSL, SL, LB, ZZ—all with postgraduate qualification and at least 5 years mixed methods experience in health services research/evaluation, including qualitative data collection methods). The email had an information sheet explaining the purpose of the evaluation, reason for being invited to interview and how their personal data would be used and stored. All participants were given at least 72 hours before being contacted by telephone. The evaluation team checked whether people understood the contents of the information sheet and were given opportunities to ask questions. They were informed that they could withdraw from the evaluation at any time without any impact on them. Fourteen of the 15 service users agreed to participate and provided verbally recorded informed consent. Service user interviews were conducted by JTSL, SL, LB and ZZ (all had no prior relationship with participants) and were 20–59 min in duration.
The service lead identified 12 staff members who were actively involved in the ongoing delivery of HEAL-D Online. All staff were invited to an interview by SL or JTSL and seven agreed to participate. Service delivery staff were consented using the same process as service users. All service delivery staff interviews were conducted by either SL or JTSL (who had no prior relationship with the participants) and were 15–90 min in duration.
All interviews with service users were conducted between 1 and 3 months after they had completed the HEAL-D Online course. All interviews with service delivery staff were conducted while they were still delivering the HEAL-D Online course.
A topic guide was used to explore experience of participating in HEAL-D Online to understand the feasibility and acceptability of the programme as part of a semi-structured interview technique (online supplemental appendix ii—service user interviews; online supplemental appendix iii—service delivery staff). Interviews were conducted by the evaluation team using Microsoft Teams, with all interviews recorded and transcribed through the platform. On completion of each interview, the interviewer relistened to the recording alongside the Teams transcript to ensure the accuracy of the content. To ensure accurate transcription, JTSL and SL checked two of each other’s interviews for accuracy. Additionally, JTSL checked the accuracy of two interviews conducted by LB.
Observations
As per usual practice in fidelity assessment, a customised observation checklist was developed based on the core components and principles underlying HEAL-D Online.12 This checklist included key items linked to delivery structure, cultural sensitivity and competence and underlying theory used to evaluate service delivery fidelity (online supplemental appendix iv). It consisted of 13 items, except for session 1 (11 items) and session 3 (12 items), which had components that were not relevant or unique.
Seven sessions were observed, selected from the seven HEAL-D cohorts, with the evaluation team (SL) identifying those with different delivery staff and on different days/times to gain an overview of the different delivery styles. All sessions were observed by SL, while three sessions (3, 5 and 7) were observed by both SL and JTSL independently, and their scores were compared to assess interobserver reliability. Service users were informed about the purpose of the observation, and permission was obtained from them before SL and JTSL were allowed to observe their sessions.
Data analysis
Quantitative
Frequencies and percentages were used to describe the level of service users’ engagement, their satisfaction with the delivery of HEAL-D Online, their expectations and any self-reported health benefits gained from participating in the programme. To assess the level of diabetes-related emotional distress at pre-attendance and post-attendance, total PAID-5 scores were calculated, and descriptive statistics were used to describe the level of distress at both timepoints. The percentage of distressed participants (PAID-5 score ≥8) was also calculated at both timepoints. Data were summarised to understand potential patient benefits and the feasibility of delivering HEAL-D Online.
Qualitative
Interview transcripts were first read in their entirety by the interviewer. The Framework Method was used for analysis, using a matrix developed from the topic guide.13 Relevant excerpts from each transcript were transferred to the framework and thematically analysed to summarise key concepts. Excel was used to organise data for analysis. A between-participant analysis was conducted to explore similarities and differences in perceptions of HEAL-D Online. Data were analysed with a focus on understanding the acceptability and feasibility of virtual delivery. Using a triangulation process, qualitative data were also used to understand and explain patterns in the quantitative data. To check on the accuracy of the analysis, JTSL and SL both independently coded two of their respective interviews.
To explore the feasibility of delivering HEAL-D Online, the fidelity of the different sessions was calculated using the mean rating score from the observations on the fidelity checklist. Inter-rater reliability was calculated by comparing the checklist items where both observers rated similarly against those they rated differently (see online supplemental appendix iv).
Patient and public involvement
Co-design has been integral throughout the development of HEAL-D, and this ethos continued in this evaluation with the recruitment of a group of people of African and Caribbean heritage who had been involved either in the original HEAL-D co-design research or had completed the online course to form a reference group.7 14 The reference group met regularly, approximately bi-monthly, from initial review of the evaluation design, through to co-design of service user interview materials (including the consent form, information sheet and topic guide), review of the postcourse questionnaire and discussions regarding analysis and reporting. Results were shared with the reference group, and members engaged with dissemination activities related to the programme, including a podcast and conference presentations.
Results
Participants
Service users
Qualitative
Demographic and clinical characteristics for service user interviewees are presented in table 1. Of the 14 participants, the majority were female (n=8, 57%), had an African heritage (n=8, 57%) and an average age of 51 years. The median time since diagnosis was 2 years (IQR 1–4; range 0.3–20). Most had been provided with some information about diet and the need to exercise (n=9, 64%) and only two (14%) had been on a DESMOND diabetes programme (www.desmond.nhs.uk) or a similar self-management course before attending HEAL-D Online.
Demographic and clinical characteristics of service user participants in qualitative arm of the evaluation
Quantitative
No demographic data were collected for the quantitative sample other than the fact that all participants were of African or Caribbean heritage, due to privacy statements from the participating NHS trust regarding the sharing of personal data.
Service delivery staff
The characteristics of the seven service delivery staff interviewees are presented in table 2. The sample consisted entirely of female participants, mainly from black cultural heritages, with a median of 2 years (range <1 year to 9 years) of experience working on HEAL-D Online. Data on culture heritage are provided for completeness, as the literature suggests that there may be potential benefits for service users when delivery staff share the same cultural heritage.15 All service delivery roles were represented, including service management; physiotherapy, dietitian, lay educator and cooking workshop facilitator.
Demographic and clinical characteristics for service delivery staff—qualitative arm of the evaluation
Results
Acceptance of HEAL-D Online for service users
Service users’ engagement with HEAL-D
Eighteen courses ran between January and December 2022, offering 197 places for potential participants to attend. 135 places were booked, with 84 patients attending the first session and 51 marked as ‘DNA’, resulting in a 62% attendance rate. An analysis of programme attendance revealed that 65 individuals completed the course (attending at least 4 out of 7 sessions), leading to a completion rate of 77% for the 84 participants who attended the first session and 48% for the 135 people who were initially booked.
Interview data suggest that this high level of engagement among participants who attended the first session may be linked to the course’s relevance to their lives and the new knowledge they gained from it.
“When I stumbled onto the programme, it just got my interest. You know the way the programme was being introduced. The topics, I was like, wow. I didn’t want to finish because every day you go in, you learn a new thing.” (Service user 1013)
Service users’ perceptions of service provision
Figure 1 outlines participant satisfaction with the delivery of the seven key HEAL-D Online elements explored in the postcourse questionnaire (n=53). Nearly all participants expressed satisfaction with the delivery of all seven key elements of HEAL-D Online. All 53 participants reported that the facilitator delivery was either excellent or good. At least 48 (91%) participants gave a similarly positive rating for other aspects of HEAL-D Online, including the initial contact with the HEAL-D team, interaction with the facilitator, the HEAL-D participant pack, cooking and exercise sessions and interaction with other service users. All participants reported they would recommend HEAL-D Online to family and friends. Qualitative data suggest that peer support and the achievement of their learning goals were key reasons behind for this willingness to recommend the programme.
“The reason why I will refer other people to it [HEAL-D] is because I learned a lot about my diet, exercises, drinking, and hearing from other people, reassuring me that don’t worry. It’s gonna be OK. You’re not on your own.” (Service user 1005)

Satisfaction with the seven elements of delivery in Healthy Eating and Active Lifestyles for Diabetes (HEAL-D) Online (n=53).
Thirty-two service users were asked whether the HEAL-D Online programme met their expectations. All agreed that it had either met or exceeded their expectations. The fact that HEAL-D Online is attended only by people of African and Caribbean heritage made the experiences of living with diabetes more relevant to those in the group and made HEAL-D Online more acceptable than other diabetes educational courses people had attended previously.
“So that’s what brought me back and also other people’s experiences of black people’s experiences of how diabetes affect them. (Service user 1007)”
The impact of a digital mode of delivery on service user participation
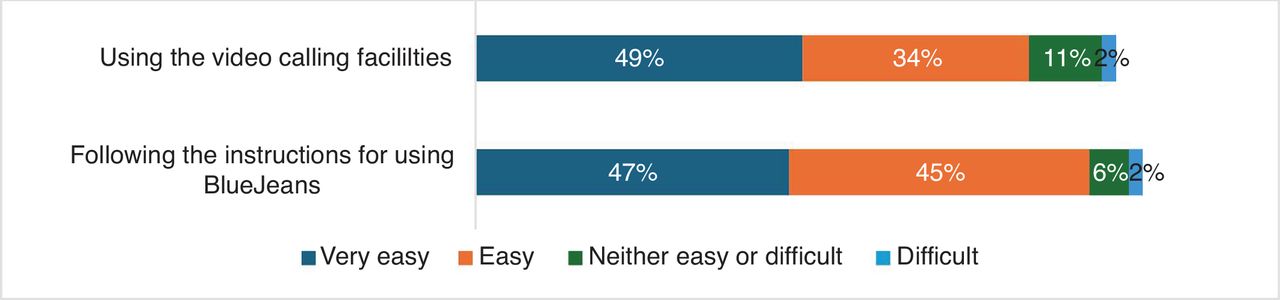
Service delivery data from the 53 participants showed that most (83%, n=44) found the BlueJeans video calling facilities—the online delivery platform used to deliver HEAL-D Online—easy to use. Additionally, 92% (n=49) reported that the instructions for use were easy to follow (figure 2), indicating that service users had little difficulty in using the technology. These findings are supported by interview data, which indicated that nearly all participants faced no major challenges using the technology to access HEAL-D Online. However, a few reported issues with downloading or accessing BlueJeans. Some participants commented that they were generally comfortable using digital technology, while one service user mentioned receiving technical support by her granddaughter to access HEAL-D Online. Some participants stated that with the onset of the COVID-19 pandemic, people had generally become more accustomed to programmes being delivered online.

Ease of using the video calling facilities for Healthy Eating and Active Lifestyles for Diabetes Online (n=53).
“I suppose because we’ve come out of lockdown, I’ve been used to doing lots of things virtually anyway, because even a support group that I mean, that’s been virtual, so that was OK.” (Service user 1010)
This was reiterated by service delivery staff, who felt that service users had become more accustomed to online delivery of services due to the COVID-19 pandemic.
“I joined at a time where people have become used to virtual, if this was before COVID I think it would be a lot more challenging. It’s almost like people are used to it and are more open to the idea now of doing things virtually.” (Service delivery staff 2002)
Qualitative data highlighted convenience and flexibility as two key advantages of virtual course delivery. It was easier for service users to attend the sessions, and they could attend if they were away from home, and thereby not miss a session.
“I actually joined it while I was on holiday with the time difference and all that stuff, and there was another lady that I know that she was in [west African country] and she joined it as well. I really wanted to do it, so I took my computer with me and everything.” (Service user 1011)
Delivery staff recognised the benefits of flexibility and convenience that virtual delivery offers, noting its potential to allow more service users to access the HEAL-D programme.
“I think it’s great because people, after work, can’t always be somewhere face to face and you know having that option of just logging in whenever. We had people log in on their lunch break, we had people log in on their way to work and participate. So it opens up a door to people who don’t want to do face to face sessions.” (Service delivery staff 2003)
The feasibility for service delivery staff to deliver HEAL-D Online
The observational data showed that service delivery staff were successful in delivering the components of HEAL-D using a digital platform, confirming that HEAL-D Online was being delivered as intended. This is indicated by a mean fidelity score of 94% (online supplemental appendix v) showing that 118/126 items on the fidelity checklist were observed by two independent raters during the delivery sessions. Inter-rater reliability between the two independent observers showed 100% agreement on the three joint observations. The observation data showed that service delivery staff achieved 100% fidelity in four of the seven sessions, with fidelity rates falling below 90% in only one session.
Although the observational data indicated the feasibility of delivering HEAL-D Online, qualitative data identified challenges faced by service delivery staff in conducting these sessions. Those who had previously been involved in face-to-face delivery noted how online delivery requires different skills to effectively engage service users.
“When you’re online I feel that you have to work extra hard to keep people engaged and one of the ways to do this is by being ‘more animated’.” (Service delivery staff 2007)
These issues may stem from the need to balance respect for the older age group in African and Caribbean cultures with their potential lack of knowledge in using the new technologies. For service delivery staff, it was important to recognise and address the challenges individuals faced when using the technology.
“Respect and regard for this kind of age group is quite important in the black African and Caribbean culture, and to help them to not feel silly or to carry them along very respectfully, but in a way that they don’t feel that they are technologically behind. I think it takes a different kind of skill because they’re also dealing with a chronic illness, which they’re probably really worried about. So, it’s kind of trying to lighten that and make it not such a big deal [if they struggle with the technology].” (Service delivery staff 2007)
Another key challenge with online delivery was encouraging interaction and engagement among service users, particularly at the start of the sessions. The option to turn off cameras added an additional layer of complexity when trying to assess service user participation and engagement.
“There’s an option to turn your camera off. So those people who are just signing in because they feel they need to show that they are attending but will turn the camera off and not engage in any conversation, that can be quite challenging. Whereas if they physically were there, they can’t turn the screen off.” (Service delivery staff 2002)
This difficulty in assessing engagement resulted in safety concerns during the delivery of the exercise component, making it more challenging for the physiotherapy team to determine the right level of exercise for the group.
“If someone’s cameras are off, it can be quite difficult to gauge how they’re finding it, so thinking of a safety element as well, it can be difficult to know. And you know, am I offering the right options? Is it too easy or hard? Even when the cameras are on, it’s quite difficult. You can’t hear someone breathing heavily or not. And sometimes you can’t see their whole body.” (Service delivery staff 2006)
Delivering the cooking session effectively online posed challenges, as sensory aspects—such as smells and the physical experience of seeing and touching the ingredients—are difficult to recreate in a virtual environment.
“It’s quite different to being in the kitchen where people are quite engaged if there’s a lot of sensory aspects to being in the kitchen, the smells, the auditory, the touch. When you’re online, you have to work extra hard to keep people engaged, even though our videos are fantastic.” (Service delivery staff 2007)
An additional challenge in the online delivery was the use of a digital platform that service delivery staff were unfamiliar with. It was not possible to use the digital platforms that delivery staff were used to, such as Zoom or Microsoft Teams, as they were not considered secure enough to deliver patient care. Instead, the health providers used a digital platform called BlueJeans, which works in a similar way to Zoom or Microsoft Teams, but has high levels of data security. Unfortunately, many service delivery staff had issues using BlueJeans in delivering the online course, such as sharing session videos or understanding how to operate the platform, even for staff who consider themselves ‘tech savvy’.
“Some of the feedback we get is a difficulty with BlueJeans, like some of the dietitians find that quite difficult to navigate. I guess we use MS Teams most of the time, so it’s kind of like using a different system.” (Service delivery staff 2001)
It was acknowledged that over time, the online platform became easier to use as staff became more familiar with it.
“We now know exactly what settings are [needed] and are better at troubleshooting. Now if something were to happen just through that experience, some of it happening before. So yes, I definitely feel like it’s much smoother.” (Service delivery staff 2006)
Potential benefits to service users from participating in HEAL-D Online
Service users reported a range of benefits from participating in HEAL-D Online (figure 3). All agreed that it was helpful to meet other people with diabetes and that it provided them with support to live with diabetes. Most felt they learnt practical skills and that it helped their confidence in managing their diabetes. The qualitative data further illustrated that service users felt that they were more knowledgeable on diabetes management and recognised the importance of managing their diet, understanding their food intake, doing more exercise and regularly monitoring their weight and blood sugar levels.

{kind=link}
{kind=link}
{kind=link}
Learning outcomes following Healthy Eating and Active Lifestyles for Diabetes (HEAL-D) Online (n=53).
“How to manage my diabetes in regard to the kind of food I eat. These are routines that I never used to do. Now I’m very careful what I eat. I watch the portion sizes. I do the exercises and then I'll make sure that the way the food is prepared, because the way most of our foods are prepared, that’s where we get it wrong.” (Service user 1013)
Of the 32 service users asked, 78% (25/32) self-reported weight loss following the HEAL-D programme, and 72% (23/32) noticed a reduction in waist measurement. Service users showed improvement in diabetes-related emotional distress after completing HEAL-D Online, with a reduction in total median PAID-5 scores from 7 at precourse to 4 at postcourse. This improvement was further illustrated by a decrease in the proportion of participants showing diabetes-related emotional distress (ie, PAID-5 score ≥8) from 49% precourse to 23% at postcourse. The qualitative data further support this quantitative evidence of potential benefits, with service users reporting that they had changed their dietary and exercise behaviour and had become more conscious of monitoring their weight and blood sugar levels. Service users felt more confident in managing their diabetes. For some service users, this also improved their level of happiness.
“It makes me feel happier with myself as a person and makes me feel better knowing that I’m trying all I can to manage my diabetes.” (Service user 1013).
Qualitative data suggested that HEAL-D Online acts to build both the confidence and the social support network of service users, which facilitated their ability to use the skills taught during the programme to manage their diabetes. Most acknowledged the role of the educators’ ability in engaging service users, and creating a safe and non-judgmental space to discuss sensitive topics.
“They (the facilitators) were lovely in how they presented the course, the way they were engaging and how they’re having the discussions. They were supportive and encouraging. They make you feel involved and welcome. So you can literally be yourself and then, it allows you to be more open, to be able to discuss things that you normally don't talk about.” (Service user 1011)
Even using a digital platform, the educators were able to create a safe space for service users that encouraged them to develop a forum for peer support, create group cohesion and provide the conditions for service users to share stories and experiences. By sharing learning among themselves, service users could find relevant solutions in living with diabetes and reassurances that their situation was not unique and that other people from similar cultural backgrounds had experienced similar situations.
“The thing is that we’re talking, no one was looked down upon. Everybody was listening to you. It was just like a little family gathering, whereby we could talk to each other and tell people what is wrong with us and find solutions.” (Service user 1013)
Improvements to HEAL-D Online
Qualitative data indicated that service users were generally overwhelmingly positive about the programme. From the interviews, two service users felt that no further improvement was necessary, with the remaining 12 identifying specific issues in two key areas: ‘postcourse follow-up support’ and ‘increasing engagement for those with impairments’.
Postcourse follow-up support
Many service users had a sense of loss when the HEAL-D Online programme ended. Most would have liked follow-up from the HEAL-D team. One felt that a postcourse review would encourage participants to maintain their commitment to changing their behaviour.
“I think a monthly or quarterly review (after the last session). Just call the participant “how are things, is everything OK, any challenges, can we support you? Say that you’ll be receiving a call from the team, who may ask about your diet? May be useful if you’re not someone that can self-motivate, you will just slide back to your old habit” (Service user 1011)
Many service users made close connections with their peers and would have liked to have maintained these once the course had finished. Some suggested sharing contact details, with one suggesting specifically setting up a WhatsApp group to connect peers as a source of support and advice.
Increasing engagement for users with impairments
Service users reported that it is important for course administrators to check with service users if they had any issues or impairments that limit their ability to participate with the delivery of an online programme. One service user with a visual impairment had difficulties in seeing the slides on their phone.
“The slides could have been clearer, so more work to be done on the slides so if you were viewing it on a computer or a phone, you would be able to see.” (Service user 1007)
Discussion
This evaluation demonstrates the feasibility of implementing a virtually delivered culturally tailored T2D self-management programme specifically aimed at the UK African and Caribbean population. To the best of our knowledge, this is the first diabetes management programme of its kind for this community delivered via a digital platform. Our findings showed a high level of acceptance among service users, as highlighted by a 77% completion rate of service users who attended the first HEAL-D Online session. Service users appreciated the convenience and flexibility that the online programme offered.
Service delivery staff were successful in delivering the key elements of the programme (educational sessions, exercise class, cooking workshop) using an online platform, while service users generally had few problems using the technology to access the programme. At the same time, qualitative findings highlighted potential safety issues that future service delivery staff need to be aware of in delivering, for example, exercise sessions, especially if HEAL-D Online is scaled up to a national level.
HEAL-D Online showed potential service user benefit in improving both understanding of diet and knowledge of diabetes management and its ability to encourage the behavioural change needed to elicit a subsequent reduction in weight and blood glucose level. A reduction in diabetes-related distress was also observed following attendance at the programme. Qualitative findings illustrated that the supportive elements provided by the educators could also be recreated using an online platform such as the ability to provide a safe environment for service users to ask questions, allowing open discussions and supporting conditions for peer support.
Service delivery data showed that attendance uptake of 62% for HEAL-D Online was high compared with the national attendance figure of 8.2% of people with T2D who are offered to attend a structured diabetes educational course.16 This suggests that HEAL-D Online is successfully targeting and engaging with individuals. Nevertheless, this evaluation was unable to record reasons why the remaining 38% did not attend their first session and it is important to understand if people are unable to take up the offer of HEAL-D Online because of its digital nature, and if non-attendance at session 1 was because of digital poverty and digital literacy. A limitation of this evaluation was that no attempt was made to explore these safety concerns; however, there is currently a clinical trial underway that may potentially address these issues.17
Service users were happy with the programme content but would have appreciated further follow-up afterwards. Specific improvements to the programme include providing post-intervention support from the HEAL-D Online team and a needs assessment for attendees with sensory disabilities to ensure better accessibility during the sessions and to check that programme participants can read the presented material, for them to gain the most out of the sessions.
Some caution is needed in interpreting these findings. Both the service delivery data and qualitative data are from service users who completed the course, which indicates some level of self-selection bias. It is not possible to comment on the representativeness of the service users in relation to the intended target population, as no demographic data were collected from those who completed the service delivery questionnaires. However, demographic data from the qualitative sample suggested that the intended population was indeed targeted. Future evaluations would need to incorporate the views of service users who did not complete the sessions or take up their places, to understand why they did not accept and explore potential barriers to accessing HEAL-D Online.
Our sample of service users appeared to be digitally literate or had family members who could provide necessary support. This sample had access to a range of devices such as laptops, tablets or mobile phones. Although the COVID-19 pandemic and associated rapid digital transformation have provided people with greater exposure and confidence in using digital technology, ‘digital poverty’ is still an issue, with 10% of the adult UK population lacking access, skills or confidence to use the internet or digital technology,18 and rates are highest in both older and socioeconomically deprived people, who are also more likely to live with T2D.19 In addition, specific issues such as distrust of technology and lack of understanding of how to navigate online health services are recognised in people from minority ethnicities.20 This is an area where more studies are needed to explore if digital-specific issues are a cause of non-attendance. This evaluation relied on self-reporting in measuring weight loss and future evaluation should aim to collect the relevant key clinical outcomes (weight and blood glucose levels) to objectively confirm that a change in clinical outcomes has occurred. Finally, as there was no control group, it cannot be concluded that the potential patient benefits identified were solely due to HEAL-D Online. Evaluating this question would require testing using an experimental design.
Conclusion
It is feasible to deliver HEAL-D using an online platform, with online delivery achieving similar goals compared with its face-to-face counterpart. Implementation challenges related to the identification, recruitment and referral of eligible patients into the programme, as well as safety issues associated with the exercise component, need to be carefully considered. Subsequent studies should establish the feasibility of scaled implementation and explore the causal links between HEAL-D Online and improvements in diabetes outcomes.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved under the Minimal Risk Registration, and ethical clearance was granted by King’s College London’s Research Ethics Office (ref: MRA-21/22-28498). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank Lipi Begum (LB) and Zoe Zambelli (ZZ) for conducting some of the service user interviews; Kate Lambe for reviewing the initial draft of the manuscript and all the service users and staff of HEAL-D Online who participated in this evaluation, as well as those who participated in our HEAL-D project lived experience reference group.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SL, LMG, SI, OB, NC, NS, AW conceived and designed the project. SL and JTSL designed data collection tools, and acquired and analysed the data. JTSL drafted the initial manuscript. SL, LMG, SI, OB, NC, NS and AW reviewed the manuscript critically for important intellectual content. All authors gave the final approval of the version to be published. JL acted as guarantor.
Funding This work was supported by NHS Accelerated Access Collaborative (AAC) and the National Institute for Health and Care Research (NIHR) through the NHS Insights Prioritisation Programme (NIPP).
Competing interests NS is the director of London Safety and Training Solutions, which offers training and improvement and implementation solutions to healthcare organisations and the pharmaceutical industry. JTSL, SL, LMG, SI, OB, NC and AW have no conflicts of interest to declare.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the 'Methods' section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.