Article Text

Abstract
Objective Systemic immune-inflammation index (SII) is a novel biomarker that can predict poor outcomes in tumours, nervous system diseases and chronic heart failure. Here, we investigated the predictive value of SII on the poor postoperative outcomes and short-term prognosis of heart valve diseases (HVDs).
Design, setting and participants This retrospective cohort study enrolled all consecutive patients with HVDs (aortic stenosis, aortic regurgitation, mitral stenosis and mitral regurgitation) who underwent surgery (valve replacement or valve repair) at the Affiliated Hospital of North Sichuan Medical College between 2017 and 2020.
Main outcomes and measures Major complications in the perioperative period, all-cause mortality within 30 days and readmission within 30 days.
Results A total of 431 patients with HVDs were enrolled in this study, including 202 males and 229 females, aged 58.9±27.3 years. SII levels of patients in the poor outcomes group were significantly higher than those of patients in the favourable outcomes group (658.40±436.29 vs 335.72±174.76, respectively; p<0.001). Multivariate logistic regression analysis showed that age (OR 1.064, 95% CI 1.026 to 1.104, p=0.025), SII (OR 1.034, 95% CI 1.012 to 1.631, p=0.008) and aortic cross-clamping time (OR 1.013, 95% CI 1.004 to 1.023, p=0.006) were independent risk factors for poor outcomes and short-term prognosis in patients with HVD. The area under the curve of poor outcomes predicted by SII in patients with HVD was 0.806 (95% CI 0.763 to 0.848) and the optimised cut-off value 423.8×109 /L, with a sensitivity of 70.3% and specificity of 81.1%. The incidence of poor outcomes (p<0.001), 30-day mortality (p<0.001) and 30-day readmission rate (p=0.026) in the high SII group was significantly higher than that in the low SII group.
Conclusions SII is closely related to poor postoperative outcomes and short-term prognosis of HVD and can serve as an independent predictive factor.
- Valvular heart disease
- Adult cardiology
- Heart failure
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This is the first study to demonstrate the relationship between the systemic immune-inflammation (SII) index and poor postoperative outcomes and the short-term prognosis of heart valve diseases.
SII, as a simple and inexpensive biomarker, was used as an indicator to predict poor postoperative outcomes and the short-term prognosis of heart valve diseases.
Patients were divided into a favourable or poor outcomes group based on whether they had had major complications in the perioperative period, all-cause mortality within 30 days and readmission within 30 days.
Many patients were excluded due to incomplete raw data.
A retrospective cohort study design may lead to information bias and confounding bias.
Introduction
Heart valve disease (HVD) is a common condition resulting from cardiac surgery in adults, and valve replacement or valvuloplasty under cardiopulmonary bypass (CPB) is the primary operative procedure to treat HVD.1 Due to ischaemia-reperfusion injury caused by long-term CPB, some patients have a poor prognosis and may even die.2 Therefore, identifying the predictive factors of the poor postoperative outcomes of HVD is of immense significance to improve prognosis. Recent studies have shown that neutrophils, lymphocytes and platelets play an essential role in chronic inflammation and are important factors in the progression of cardiovascular diseases.3 Moreover, HVD and CPB can induce the inflammatory response syndrome, resulting in increased postoperative complications involving the vital organs and may even result in mortality.4 Biomarkers related to inflammation such as C reactive protein, as well as the neutrophil/lymphocyte ratio (NLR) and platelet/lymphocyte ratio (PLR) are used to predict complications and mortality related to cardiovascular diseases.5 6 Systemic immune-inflammation index (SII) is a new biomarker that has been receiving increasing interest in recent years.7 SII integrates the characteristics of neutrophils, platelets and lymphocytes, and provides a higher predictive value compared with NLR and PLR predictions alone. Studies have verified that a high SII score is related to the prognosis of tumours, nervous system diseases and chronic heart failure.8–10 However, to the best of our knowledge, there are no studies on whether SII can serve as a predictive value for postoperative HVD having a poor prognosis. In this study, we evaluated the predictive value of SII in poor postoperative outcomes and the short-term prognosis of HVD.
Patients and methods
General information
Adult patients with HVD having complete data were retrospectively investigated. Surgery on patients was performed at the Cardiovascular Surgery, Affiliated Hospital of North Sichuan Medical College between February 2017 and January 2020. All patients were explicitly diagnosed using echocardiography. The main heart-valve pathologies include aortic stenosis, aortic regurgitation, mitral stenosis and mitral regurgitation, regardless of the presence of tricuspid stenosis or tricuspid regurgitation. All patients underwent heart valve surgery (valve replacement or valve repair) by CPB. The inclusion criteria were as follows: (1) patients diagnosed with HVD before the operation, regardless of stenosis and insufficiency; (2) all patients who received surgical treatment and (3) patients >18 years of age. The exclusion criteria were as follows: (1) patients who underwent other cardiac surgeries (cardiac tumour surgery, coronary artery bypass grafting, vascular surgery) at the same time; (2) patients <18 years of age; (3) patients who underwent ≥2 counts of valve surgeries during a hospital stay or had a history of valve surgery; (4) patients with incomplete or missing clinical data; (5) patients who underwent interventional valve replacement or repair without CPB; (6) patients with infective endocarditis and (7) patients with a malignant tumour.
Data collection
Related preoperative variables in this study included: general information such as age, gender, body mass index, body weight, blood pressure, family history (diabetes, cerebral infarction, smoking and drinking history), valve pathologies; preoperative laboratory examination including leucocyte count, erythrocyte count, platelet count and lymphocyte count; and haemoglobin, alanine aminotransferase, aspartate aminotransferase, albumin, bilirubin, creatinine, troponin T and creatine kinase isoenzyme levels. SII was obtained using the leucocyte classification count calculation (SII=P× N/L, where P, N and L represent platelet, neutrophil and lymphocyte counts, respectively). Perioperative period parameters recorded in this study included the main surgical procedures, operation time, CPB duration, aortic cross-clamping time and the usage of erythrocytes. Postoperative complications of vital organs, mechanical ventilation time, length of the intensive care unit (ICU) stay, hospitalisation time, 30-day mortality and readmission rate within 30 days were recorded. All data were obtained from electronic databases and/or hospital archives.
Outcomes and definitions
Patients were divided into the following two groups based on whether they had a poor outcome postoperatively: the favourable outcomes group and the poor outcomes group. The poor primary outcomes assessed included major complications in the perioperative period and all-cause mortality within 30 days in the postoperative period. Primary postoperative complications were determined based on the definition of European perioperative period clinical outcomes11: (1) primary adverse cardiovascular events (eg, myocardial infarction, malignant ventricular arrhythmia and application of mechanical aids in low cardiac output syndrome); (2) lung complications (acute lung injury, acute respiratory distress syndrome and the requirement of prolonged mechanical ventilation or tracheotomy); (3) new-onset renal failure (serum creatinine levels increased to more than three times that at baseline, absolute value was increased and ine levels increased to more than three times that at baselirequirement of prolonged mechanical ventilation or tracheotomy); (3) wound complications requiring reoperation; (8) massive haemorrhage of the digestive tract. Secondary outcomes were as follows: readmission for any reason within 30 days in the postoperative period.
Statistical analyses
SPSS V.22.0 was used for statistical analysis. Data are expressed as‾x±s, and Student’s t-test or Wilcoxon rank-sum test were used for comparisons between groups. Count data are expressed as frequency (rate or percentage), and the χ2 test or Fisher’s exact test was performed to compare groups. Factors related to poor postoperative outcomes were analysed using univariate analysis. Variables with statistical significance in the univariate analysis were analysed using multivariate logistic regression analysis. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the accuracy of SII in predicting poor outcomes, and the results are expressed as the area under the curve (AUC). The optimised cut-off value, sensitivity and specificity were recorded. Based on the SII-optimised cut-off value, patients were assigned to the high SII or low SII group, followed by comparisons of the primary complications between both groups. Kaplan-Meier analysis was performed to compare the complication-free survival within 30 days and readmission rate within 30 days between groups, and the log-rank test was used to determine significance. Bilateral p values <0.05 were considered to be statistically significant.
Patient and public involvement
Patients or the public were not involved in the design, implementation, reporting or dissemination of this research.
Results
Patient characteristics
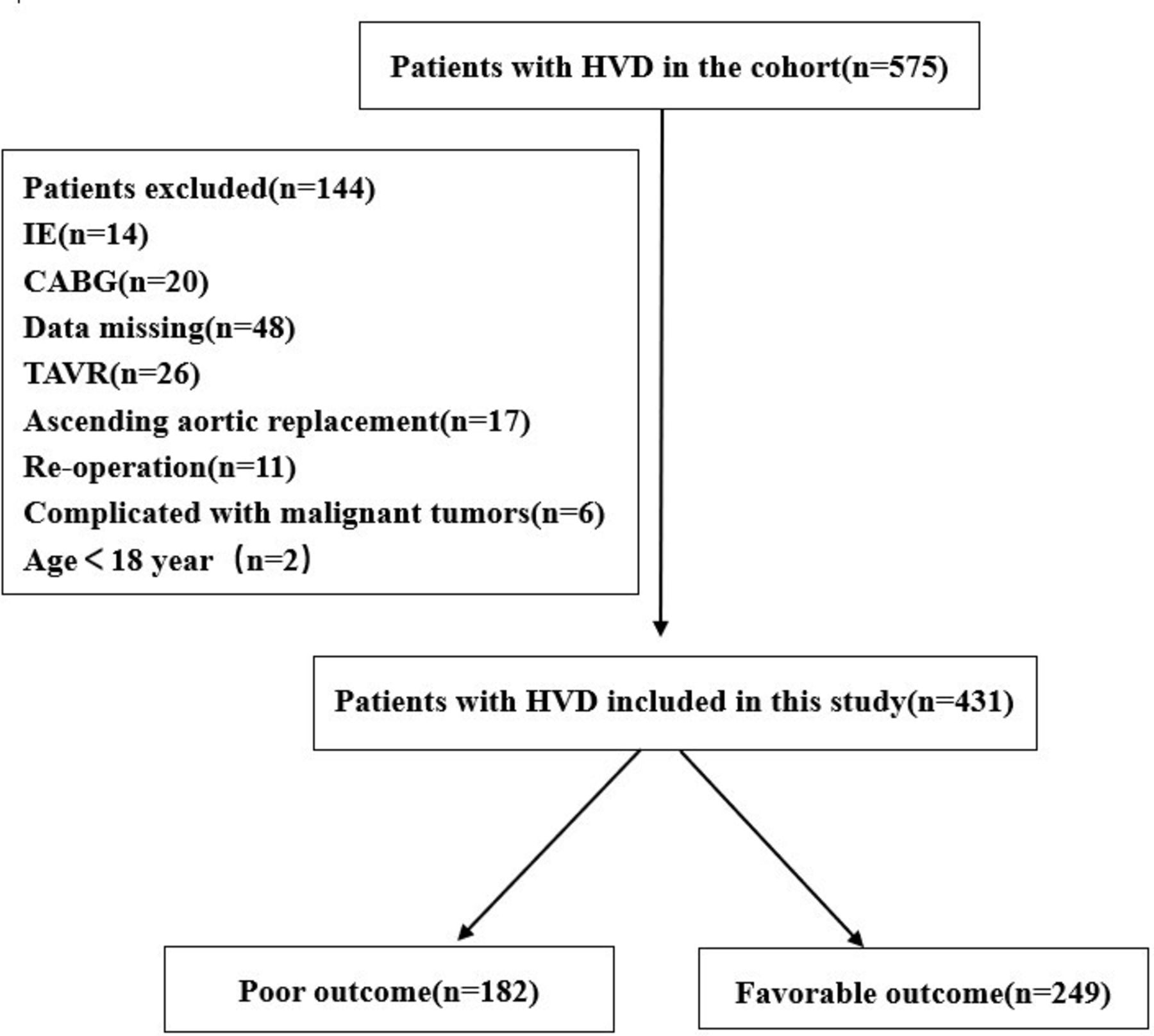
A total of 575 patients with HVD underwent valve replacement or valve repair. Patients were screened based on the inclusion and exclusion criteria. Lastly, a total of 431 patients (202 males and 229 females, mean age 58.9±27.3 years) were enrolled (figure 1), In this study, there were 182 cases with primary poor outcomes (41.23%), 23 cases with all-cause deaths within 30 days (5.33%) and 15 cases with readmission within 30 days (3.48%) (table 1).

Flow chart for patients enrollment and study design. CABG, coronary artery bypass grafting; HVD, heart valve diseases; IE, infective endocarditis; TAVR, transcatheter aortic valve replacement.
General characteristics of HVD patients
Clinical outcomes
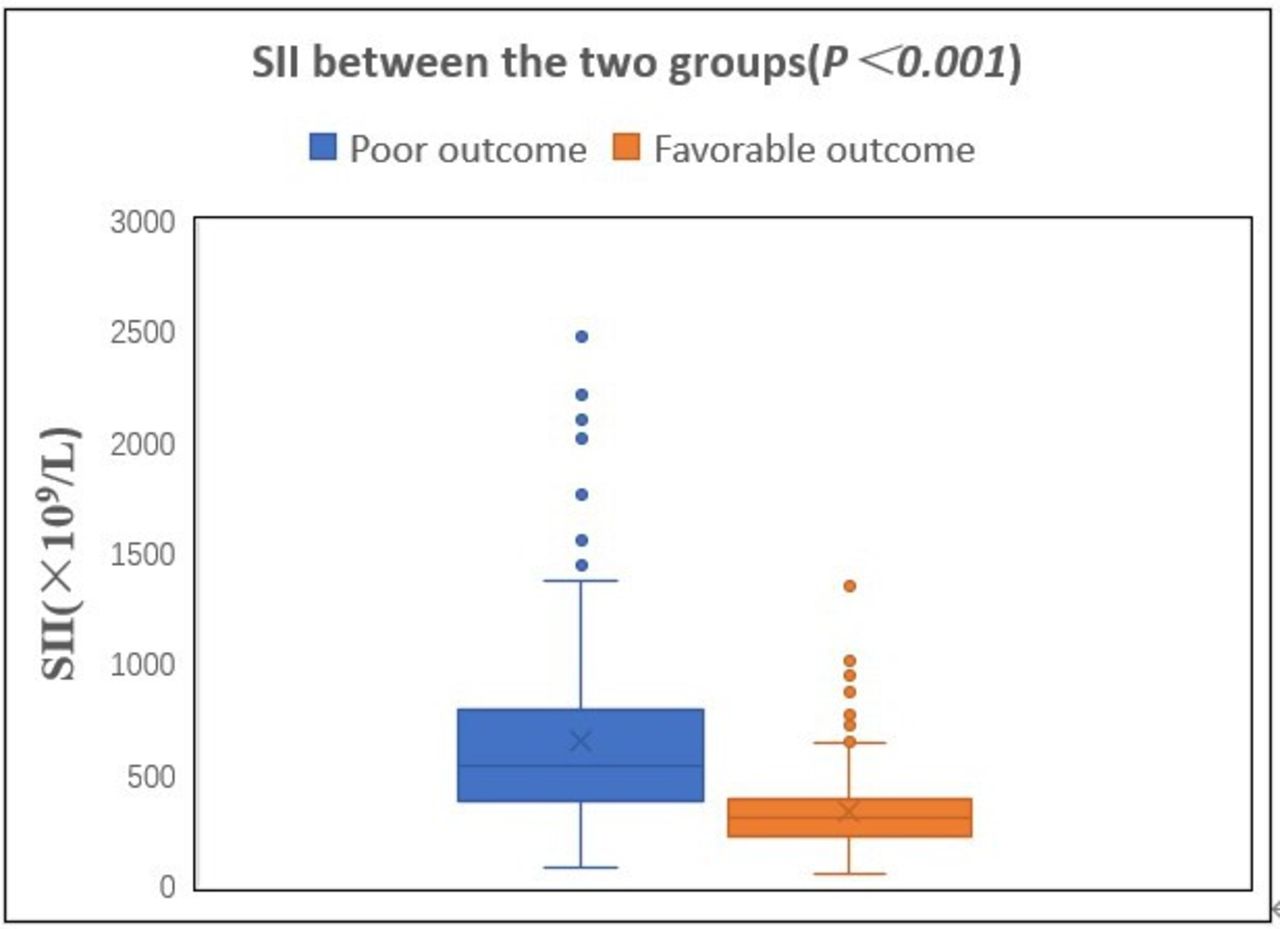
The general clinical data and intraoperative data of patients with HVD in the two groups are shown in table 2. The SII level of the poor outcomes group was significantly higher than that of the favourable outcomes group (658.40±436.29 vs 335.72±174.76, p<0.001; figure 2). Results from the univariate analysis showed that age, systolic blood pressure, haemoglobin, albumin, SII, left ventricular ejection fraction (LVEF), N-terminal probrain natriuretic peptide, New York Heart Association grade ≥3, diabetes history, CPB time, aortic cross-clamping time and intraoperative infusion of erythrocyte suspension were risk factors for perioperative poor outcomes in adult HVD (p<0.05 in all cases). Results from multivariate logistic regression analysis showed that age (OR 1.064, 95% CI 1.026 to 1.104, p=0.025), SII (OR 1.034,95% CI 1.012 to 1.631, p=0.008) and aortic cross-clamping time (OR 1.013, 95% CI 1.004 to 1.023, p=0.006) were independent risk factors for poor postoperative outcomes and short-term prognosis in patients with HVD (table 3).
Univariate analyses of variables associated with poor outcomes

Comparison of SII between poor outcomes and favourable outcomes groups. SII, systemic immune-inflammation index.
Univariate and multivariate logistic regression analysis of variables associated with poor outcomes
Sensitivity and specificity of SII in predicting poor outcomes
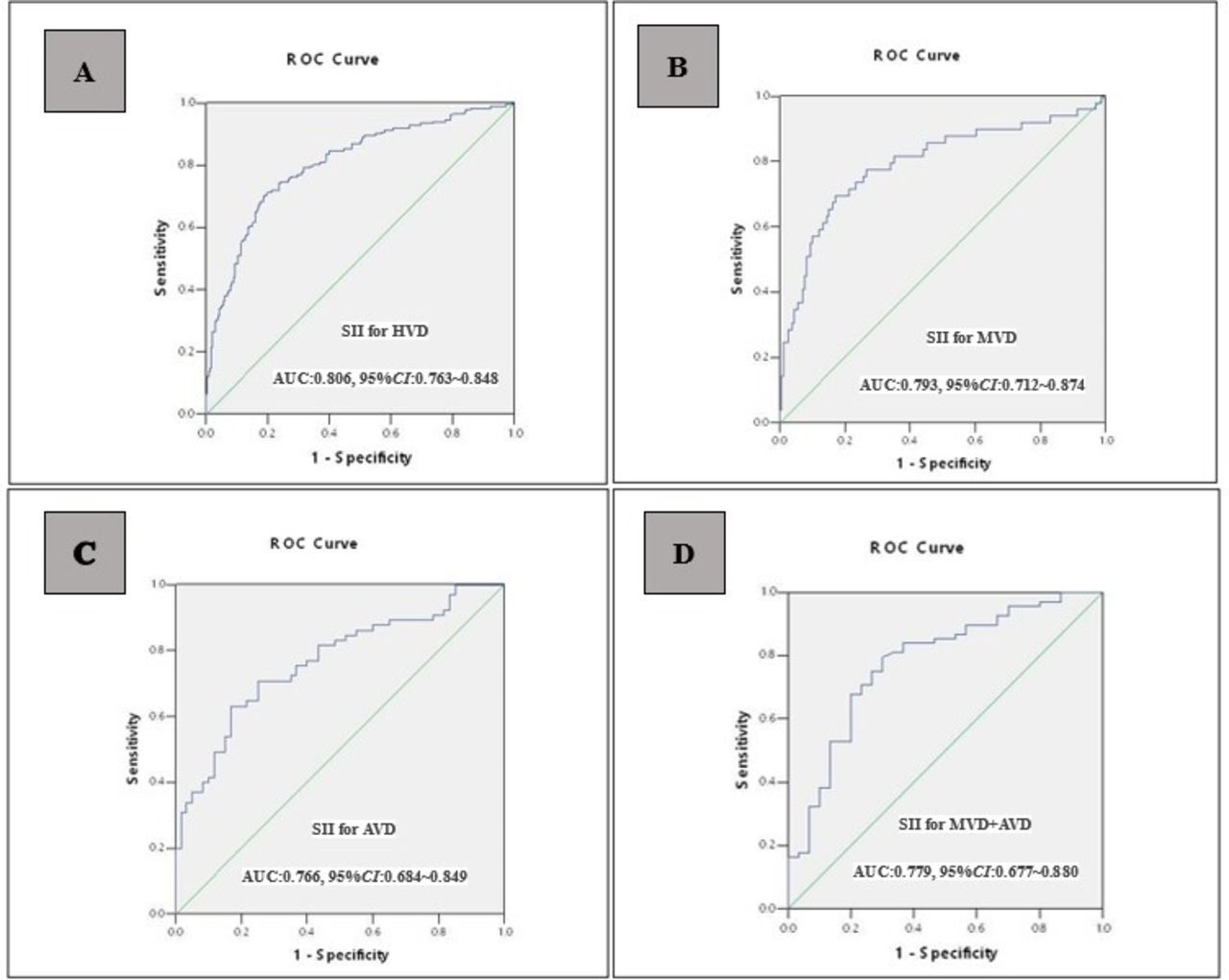
ROC analysis was used to determine the cut-off values of SII in predicting poor outcomes. The results showed that SII could effectively predict poor postoperative outcomes in patients with HVD, with an AUC of 0.806 (95% CI 0.763 to 0.848), optimised cut-off value of 423.8×109 /L, sensitivity of 70.3% and specificity of 81.1% (figure 3A). We also verified the predictive value of SII for poor outcomes in different heart valve pathologies. The results showed that SII could also effectively predict poor postoperative outcomes in patients with mitral valve disorder (figure 3B), aortic valve disorder (figure 3C) and aortic and mitral valve disorders (figure 3D), and the AUCs were 0.793 (95% CI 0.712 to 0.874), 0.766 (95% CI 0.684 to 0.849) and 0.779 (95% CI 0.677 to 0.880), respectively (table 4).

The ROC curve showing the predicting value of SII for poor outcomes in different type of heart valve pathologie before PSM. AUC, area under the curve; AVD, aortic valve disorder; HVD, heart valve diseases; MVD, mitral valve disorder; PSM, propensity score matching; ROC, receiver operating characteristic; SII, systemic immune-inflammation index.
Predictive value of SII for poor outcomes before PSM
Subgroup analyses
Subgroup analysis was conducted to determine the correlation between SII and poor outcomes across comorbidities and different parameters, and the results were shown in table 5. Stratification factors did not have a significant impact on the relationship between SII and poor outcomes (interaction p>0.05). In addition, the results of the study showed that in all subgroups, the increase in SII levels was closely related to the increase in the poor outcomes of patients with HVD (table 5).
Subgroup analysis of the correlation between SII and poor outcomes
Comparison of clinical outcomes between the high SII and low SII groups
To investigate the impact of SII on clinical outcomes, a secondary analysis of the data was conducted. Based on the SII-optimised cut-off value (423.8×109/L) obtained using the ROC curve, patients were assigned to the high SII group (C curve, p/L) or the low SII group (<423.8×109 /L). There were 169 patients in the high SII group and 262 in the low SII group. The clinical outcomes of the two groups were compared and the results showed that the incidence of poor outcomes (p<0.001), malignant arrhythmia (p=0.016), low cardiac output syndrome (p=0.027), acute liver failure (p=0.002), acute lung injury (p<0.001), acute kidney injury (p<0.001), continuous renal replacement therapy (p=0.044) and septicaemia (p=0.032) increased significantly in the high SII group. Moreover, mechanical ventilation, ICU stay and hospital stay were significantly prolonged in the high SII group (p<0.001 in all cases; table 6). Kaplan-Meier analysis showed that compared with patients in the low SII group, those in the high SII group had a significant increase in postoperative mortality within 30 days (p<0.001; figure 4A) and an increase in readmission rate within 30 days (p=0.026; figure 4B).
Comparison of complications between patients with different SII groups

Kaplan-Meier curves showing the 30-day all-cause mortalities (A) and 30-day readmissions (B) stratified by cut-off value of SII in patients with HVD before PSM. HVD, heart valve diseases; PSM, propensity score matching; SII, systemic immune-inflammation index;
Prognostic value of SII after propensity score matching
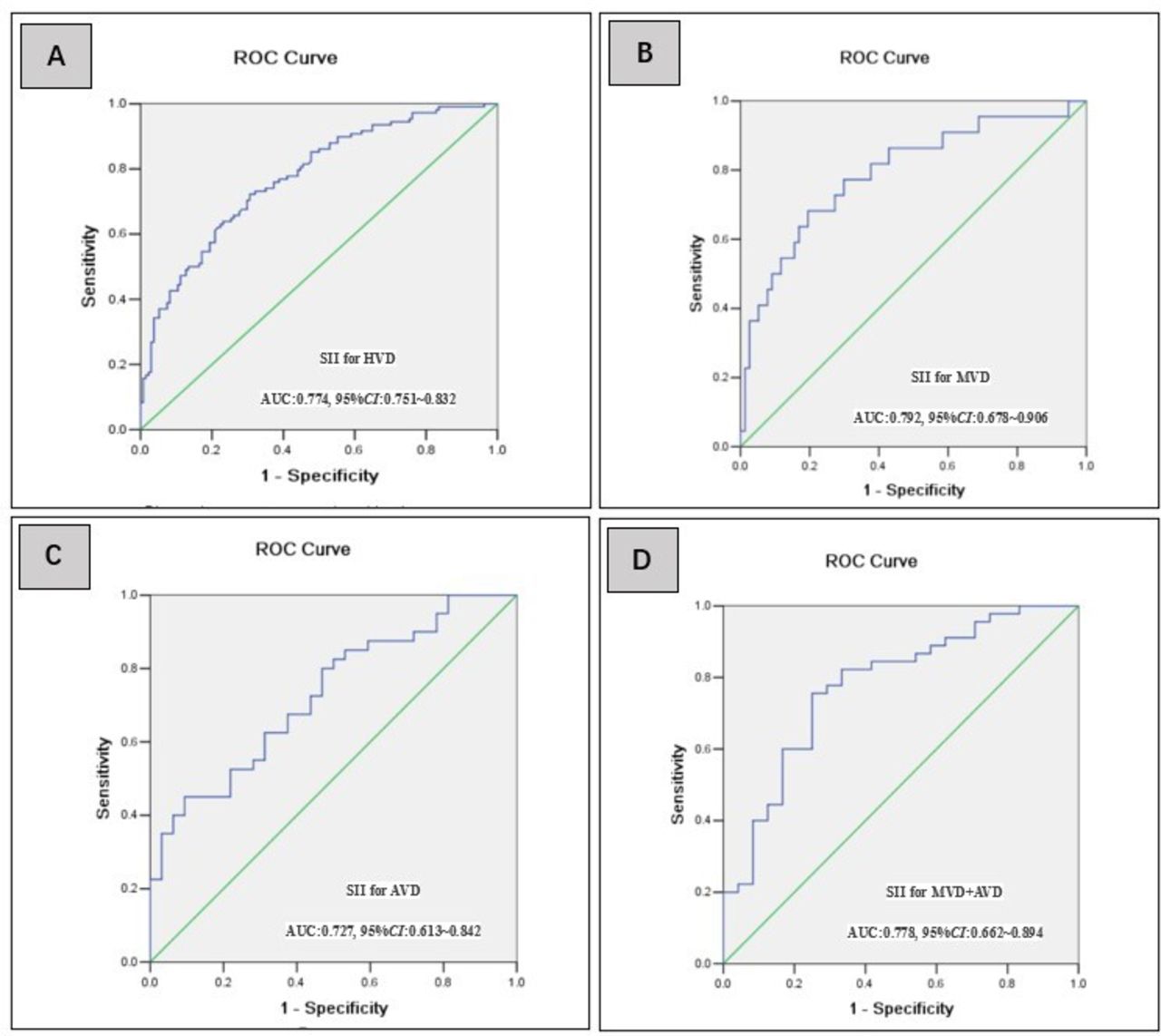
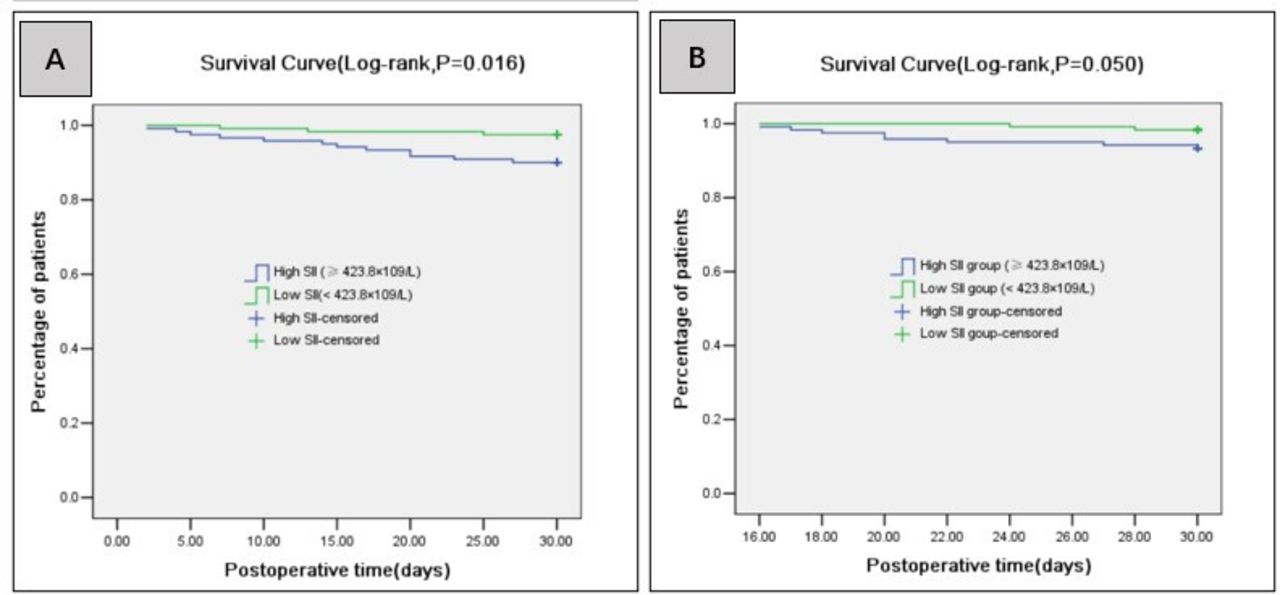
Propensity score matching (PSM) analysis with 1:1 matching was conducted to effectively balance the confounding factors and improve the credibility of our results. After PSM, 121 pairs of research objects were generated and the differences in age, systolic blood pressure, haemoglobin, albumin, LVEF, NT-pro-BNP, NYHA class ≥3, diabetes history, CPB time, aortic cross-clamping time and intraoperative infusion of erythrocyte suspension were balanced between the two groups, with good matching performance (table 7). After PSM, compared with the low SII level group, subjects in the high SII level group still had higher poor outcome rates (64.46% vs 24.79%, p<0.001), higher 30-day all-cause mortalities (9.92% vs 2.48%, p=0.016), and higher 30-day readmission rates (6.61% vs 1.65%, p=0.050). ROC analysis revealed that SII could effectively predict poor postoperative outcomes in patients with HVD after PSM with an AUC of 0.774 (95% CI 0.751 to 0.823), optimised cut-off value of 447.9×109 /L, sensitivity of 72.2% and specificity of 79.4% (figure 5, table 8). After PSM, Kaplan-Meier analysis showed that compared with patients in the low SII group, those in the high SII group had a significant increase in 30-day all-cause mortality (p=0.016; figure 6A) and 30-day readmission rates (p=0.050; figure 6B).
Comparison of variables between different SII groups after PSM

The ROC curve showing the predicting value of SII for poor outcomes in different type of heart valve pathologie after PSM. AUC, area under the curve; AVD, Aortic valve disorder; HVD, heart valve diseases; MVD, mitral valve disorder; PSM, propensity score matching; ROC, receiver operating characteristic; SII, systemic immune-inflammation index.
Predictive value of SII for poor outcomes after PSM

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves showing the 30-day all-cause mortalities (A) and 30-day readmissions (B) stratified by cut-off value of SII in patients with HVD after PSM. HVD, heart valve diseases; PSM, propensity score matching; SII, systemic immune-inflammation index.
Discussion
In this study, the prognostic value of SII in predicting postoperative short-term mortality and the readmission of 431 patients with HVD who underwent surgery were assessed. The main finding was that preoperative systemic inflammation evaluated using SII was significantly associated with an increased risk of postoperative composite complications, all-cause mortality and readmission within 30 days after valvular replacement or valvuloplasty.
HVD is the third-leading cause of cardiovascular death in developing countries after coronary heart disease and hypertension.1 Owing to the limitations of economic and geographical factors, some patients are at the end stages of the disease at their initial visits, resulting in increased surgical complications and mortality. HVD postoperative mortality is reported as 1.8%–30.2%.2 12 Reducing the complications and mortality in patients with HVD is a pressing issue. Therefore, the early identification of risk factors responsible for the poor prognosis in patients with HVD is of great significance to reduce mortality and improve prognosis. Previous studies13 14 have demonstrated that age, preoperative liver function/renal function injury, LVEF, intraoperative blood transfusion and CPB duration are important factors affecting the prognosis in patients with HVD. We found that preoperative SII was significantly correlated with postoperative complications of HVD and short-term prognosis, which have not been reported in previous studies.
It has been reported that15 inflammation and immune responses are closely related to the occurrence, postoperative complications and death in patients with HVD. Platelets adhere to the vascular wall to promote leucocyte recruitment. Moreover, the invasion of leucocytes into the diseased valves leads to disease progression, suggesting that local and systemic inflammatory processes may be involved in HVD progression.16 Investigations reveal that systemic inflammation and immune system activation are independent predictors of the long-term prognosis in patients with chronic heart failure.17 Recent studies have demonstrated that some inflammatory indices calculated based on blood cell count, including PLR, NLR and N/LP, could serve as indicators to predict complications and the poor prognoses of cardiovascular diseases.5 6 Moreover, they can predict the severity, mechanical ventilation and in-hospital mortality of patients with COVID-19.18 19 SII integrates the details of neutrophil, platelet and lymphocyte counts. A comprehensive analysis of these three blood cell counts can better clarify the interaction of inflammatory immune cells in disease states and indicate a better predictive value compared with PLR and NLR alone.7 Currently, research on SII mainly focuses on tumours, nervous system diseases, sepsis and ischaemic diseases, but only a few studies report the predictive value of SII in cardiovascular diseases.
Seo et al evaluated patients with chronic heart failure and found that those in the high SII group had a worse prognosis.20 Hayıroğlu et al21 followed up 1011 patients with intracardiac defibrillators (ICDs) for heart failure with reduced ejection fraction (HFrEF) for 10 years and found that SII may be an independent predictive marker for both long-term mortality and appropriate ICD therapy in patients with HFrEF. Some recent studies have reported the predictive value of SII in infective endocarditis and coronary heart disease.22–24 Selçuk et al23 reported that SII is a predictor of postoperative atrial fibrillation in patients with coronary artery bypass grafting and is better than NLR and PLR. Another recent report showed that SII could predict poor postoperative outcomes (eg, acute kidney injury, cardiovascular events, cerebrovascular accidents, sepsis) in patients after coronary artery bypass grafting.24 HVD is an inflammatory disease sharing the pathophysiology (eg, lipoprotein deposition, calcification and chronic inflammation) with coronary heart disease.25 There are only a few studies on whether SII has similar effects in patients with HVD. Yoon et al26 reported that high SII is closely related to postoperative 30-day mortality in patients after tricuspid valve under thoracoscopy and that it is an independent biomarker of poor prognosis in patients with isolated tricuspid regurgitation undergoing thoracoscopic surgery. Tosu et al27 investigated 120 patients who underwent transcatheter aortic valve implantation (TAVI) for aortic stenosis and found that SII was an independent predictive factor in TAVI for postoperative adverse cardiac events. The AUC of adverse cardiac events predicted by SII was 0.960, with a specificity of 94% and a sensitivity of 96%. In this study, the preoperative SII in the poor outcomes group was significantly higher than that in the favourable outcomes group. Multivariate logistic regression analysis revealed that SII was an independent influencing factor of poor outcomes of HVD with an AUC of 0.806 (95% CI 0.763 to 0.848), optimised cut-off value of 423.8×109/L, sensitivity of 70.3% and specificity of 81.1%. In addition, the incidence of poor postoperative outcomes and mortality in the high SII group was significantly increased, which was consistent with that reported in previous studies, suggesting that high SII (≥423.8×109/L) is closely related to HVD poor postoperative outcomes and short-term prognosis.
Currently, the relationship between SII and HVD poor postoperative prognosis remains elusive and may be related to the inflammatory response by the circulating immune cells (platelets, neutrophils and lymphocytes). Neutrophils can regulate inflammatory responses, secrete inflammatory mediators and exhibit strong chemotaxis and phagocytosis. Increasing neutrophil counts indicate an overactivated inflammatory response. Neutrophils induce cardiomyocyte injury by adhesion, phagocytosis, the release of several proinflammatory cytokines, and the formation of neutrophil extracellular traps, thereby further attracting and activating other inflammatory cells to participate in cardiac immunity and myocardial injury.28 Therefore, neutrophils have been used as markers in the diagnosis and prognosis of cardiovascular diseases.28 29 Platelets are derived from the mononuclear phagocyte system. They interact with leucocytes and vascular endothelial cells, activate and induce monocyte adhesion and transport, and are involved in the release of interleukin-1, tumour necrosis factor-α and other inflammatory factors, and jointly promote local myocardial inflammation and fibrosis in patients with HVD.30 Increased platelet counts have also been reported to be related to the poor prognosis in patients with cardiovascular diseases.31 On the contrary, lymphocytes are mainly involved in specific immunity. Decreased lymphocyte counts are a hallmark of immune decline. Patients with HVD usually suffer from chronic heart failure. Chronic inflammation, oxidative stress and neurohormonal activation in patients with chronic heart failure increase plasma cortisol levels and catecholamine release, resulting in the downregulation of lymphocytic differentiation and proliferation, followed by an increase in lymphocyte apoptosis.32 Therefore, lymphocyte reduction is an independent predictive factor for poor survival in patients with chronic and advanced heart failure.33 Although we found that preoperative high SII could predict poor postoperative prognosis in patients with HVD, the specific mechanism could not be clarified, thereby warranting further research.
However, our study has some limitations. First, the retrospective collection of data was prone to recall bias and other biases; for example, the time of blood collection and basic information collection may not have been on the same day, which may have introduced some bias. Second, this was a single-centre retrospective cohort study with a small sample size and short follow-up time due to which the statistical power was limited. Third, the SII boundary value was obtained using the ROC curve and there might be a more accurate SII boundary value. Fourth, we did not conduct statistical analysis on other factors affecting prognosis, such as the use of vasoactive drugs. In future studies, we plan to evaluate more possible risk factors to improve our study. Fifth, although multivariate analysis was performed, there may have been some unmeasured confounding factors affecting the results of the study. Therefore, more rigorous multicentre prospective randomised controlled studies are needed to further corroborate our findings.
Conclusions
SII, as a simple and inexpensive biomarker, is an independent risk factor for the poor postoperative prognosis of HVD. Thus, it can be used as a predictor of poor postoperative outcomes and the short-term prognosis in patients with HVD, making it worthy of further development for use as a diagnostic aid in a clinical setting.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the ethics committee of the Affiliated Hospital of North Sichuan Medical College (2018 ER(A)037).
Acknowledgments
The authors would like to thank Dr. Zhigang Deng of the Department of Cardiothoracic Surgery, Affiliated Hospital of Traditional Chinese Medicine, Southwest Medical University (Luzhou, China) for support and assistance. And we also would like to thank MJ Language Editing Services (https://www.scimj.com/) for its linguistic assistance during the preparation of this manuscript.
References
Footnotes
JX and LH are joint first authors.
Contributors JX designed the experiment and wrote the manuscript. LH contributed to the collection of data and statistical analysis. DL helped with data collection and SW helped with statistical analysis. ZW modified the manuscript and provided financial support. ZW is the guarantor of the manuscript.All authors have read and agreed to the published version of the manuscript.
Funding This research was supported by the National Natural Science Foundation of China(82172060),University-level scientific research project of North Sichuan Medical College (CBY21-QA22) and Cooperative scientific research project of Science and Technology Bureau of Nanchong, Sichuan Province (22SXQT0007).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.