Article Text

Abstract
Objective Several working groups (eg, miners, flight crews and soldiers) are subjected to chronic intermittent hypoxic exposure. The cardiovascular implications have been studied but not systematically reviewed with focus on possible negative health implications. The aim of the present review was to systematically evaluate the hypothesis that intermittent hypoxic exposure causes cardiovascular stress detrimental to health in workers.
Design Systematic review.
Data sources Electronic database search of PubMed, Scopus and Web of Science up to April 2020.
Eligibility criteria Studies of workers ≥18 years repeatedly subjected to months to years of irregular intermittent hypoxia, lasting from a few hours (eg, flight crews), one or a few days (eg, soldiers), or several days to weeks (eg, miners working at high altitude), written in English and evaluating the effect of intermittent hypoxia on cardiovascular disease were included. Animal studies, books, book chapters, personal communication and abstracts were excluded. The primary outcome measure was changes in standardised mortality ratio.
Data extraction and synthesis Two independent reviewers extracted data and assessed risk of bias using the Cochrane Collaboration’s tool.
Results 119 articles were identified initially, 31 of which met the inclusion criteria. Of these, 17 were retrospective cohort mortality studies (irregular short-term intermittent hypoxia), and 14 studies were observational (long-term intermittent hypoxia). The population of irregular short-term intermittent hypoxia users (flight crew) showed a lower mortality by cardiovascular disease. Long-term intermittent hypoxia over several years such as in miners or soldiers may produce increased levels of cardiac disorders (12 studies), though this is probably confounded by factors such as obesity and socioeconomic status.
Conclusion This systematic narrative review found that cardiovascular disease mortality in flight crews is lower than average, whereas miners and soldiers exposed to intermittent hypoxia experience increased risks of cardiovascular diseases. The impact of socioeconomic status and lifestyle appears of importance.
PROSPERO registry number CRD42020171301.
- physiology
- coronary heart disease
- occupational & industrial medicine
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
To our knowledge, this is the first investigation that has addressed whether intermittent exposure to high altitude could induce any cardiovascular diseases in workers.
We conducted a systematic review of 17 studies of irregular short-term intermittent hypoxia and 14 studies of long-term intermittent hypoxia. The review was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. We assessed risk of bias for all included studies using the Cochrane risk of bias tool.
Limitations were the lack of clarity about the methods of mortality quantification in some papers, as well as the lack of detailed information on confounding factors such as socioeconomic status, daily physical activity and malnutrition.
Introduction
Humans reside at altitudes up to ~5000 m,1 where the partial pressure of oxygen is reduced by ~50% compared with sea level. Numerous studies have investigated the physiological and clinical consequences of residence at high altitude. Distinct physiological phenotypes with increased haematocrit (Hct) and haemoglobin (Hb) concentration exist in some, but not all, high altitude populations.1 2 Despite the remarkably challenging environment, residing at high altitudes does not reduce life expectancy,3 which may be partly ascribed to acquired genetic traits.4
Unacclimatised lowlanders without a family history of hypoxic exposure frequently and repeatedly travel to altitude or are exposed to brief periods of hypoxia for various reasons. The central question addressed by the present narrative review is whether exposure to intermittent hypoxia should be considered a health hazard. Systemic hypoxia at altitude manifests as an oxygen saturation lower than the sea-level normal of ~98%. At altitudes higher than ~2500 m,5 the sigmoidal shape of the blood oxygen saturation curve is no longer enough to protect against systemic hypoxia, and saturation drops to ~95% at 2000 m and down to ~84% at 5000 m.6 It is well described that unacclimatised humans can experience acute mountain sickness after less than 6 hours of hypoxic exposure at >2500 m,7 including pulmonary and cerebral oedema,8 pulmonary hypertension9 and elevated mean arterial pressure.10 Groups frequently exposed to intermittent moderate hypoxia include working cohorts such as miners, flight crew and soldiers. However, no systematic review has addressed whether the frequent change of environment entails cardiovascular health implications.
To address this question, existing literature on intermittent hypoxia and the risk of cardiovascular disease was retrieved via a systematic search. The high variability of topics and methodology prompted us to complete a narrative review based on the systematic search. The aim of the present review is to address whether intermittent hypoxic exposure of workers not acclimatised to high altitudes poses an increased risk of cardiovascular disease.
Materials and methods
Search strategy
A comprehensive search of three electronic literature databases (PubMed (US National Library of Medicine National Institutes of Health), Web of Science and Scopus) was completed in April 2020 (full search strategy, see online supplemental table 1). The aim was to identify studies investigating the effect of intermittent hypoxia on cardiovascular disease in workers. The search strategy was implemented using the following keywords: flight crew illness, flight attendants health, aircraft cabin illness, aircraft cabin disease, flying personnel illness, flying personnel health, cabin pressure illness, military aircrew health, chronic intermittent hypoxic worker, worker high altitude, long-term intermittent high altitude, occupational health altitude and intermittent exposure high altitude. These keywords were mixed with hypoxia, altitude, pulmonary hypertension, cardiovascular disease and occupational. A PubMed search found 1506 items, a Scopus search found 1367 items and a Web of Science search found 1017 items within the following limits: publication date, limitation dates, 30 April 2020, humans, adults: 18–65 years, English language and article. This review was designed in accordance with the structured guidelines ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses’ and synthesis without meta-analysis (SWIM) checklist. This literature review was registered at the PROSPERO (international prospective register of systematic reviews) website on 28 April 2020, with the following record CRD42020171301. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020171301.
Supplemental material
Selection criteria
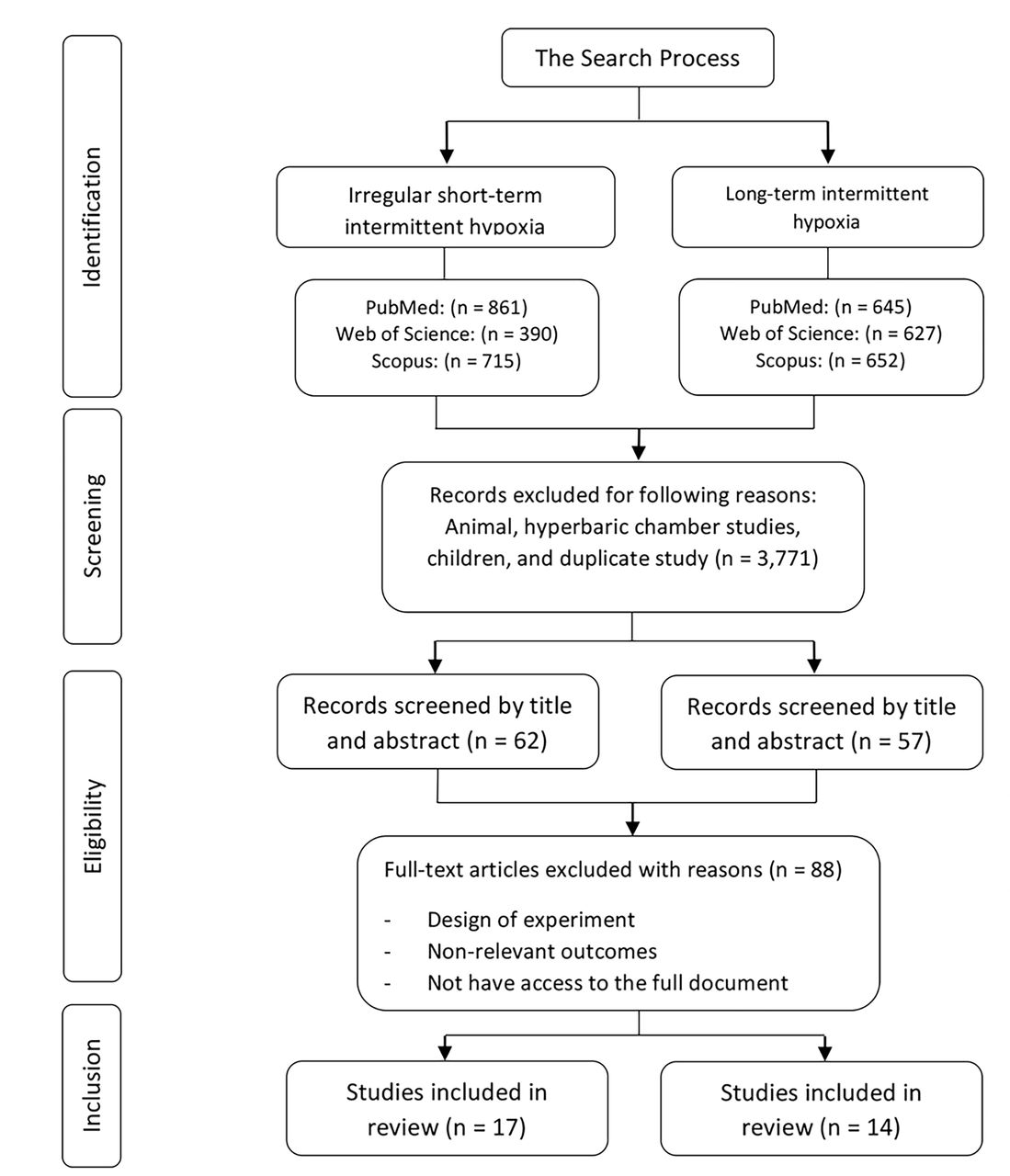
The search flow chart is illustrated in figure 1. In brief, studies of humans ≥18 years repeatedly subjected to months or years of irregular intermittent hypoxia lasting from a few hours (such as flight crews), one or a few days (such as soldiers) or several days to weeks (such as high mountain miners) were included. The following exclusion criteria were applied: non-English language, animal studies, books, book chapters, personal communication and abstracts. After removal of duplicates, acceptability for inclusion was evaluated based on title and abstract. If the abstract indicated potentially relevant information, the full article was obtained for further analysis. Studies without access to the full article were excluded.11 12 The search process was carried out independently by two authors (JA and JP-D) based on population, intervention, comparison and outcome criteria. The authors read the titles and abstracts and resolved any differences regarding study eligibility subsequently.

PRISMA flow chart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Risk of bias
JA and JP-D independently assessed the risk of bias of the selected documents using the Cochrane collaboration’s methodology. The risk of bias was tabulated for each study and was classified as low, high or unclear, as described in the Cochrane Handbook of Systematic Reviews of Interventions.13 RevMan V.5.3 was used to generate a graphical analyses of risk bias.14
Data extraction
The following information was retrieved from the included studies: (1) author identification and publication year; (2) number of participants; (3) sex; (4) age; (5) country; (6) level of hypoxia; (7) periods at sea level and in hypoxia; and (8) outcome.
Patient and public involvement
No patients involved.
Results
General overview
The diagram for the search strategy is shown in figure 1. The initial search identified 119 adequate articles, of which 31 were eligible for inclusion in the present review (figure 1). Of the included studies, 17 were retrospective cohort mortality studies of flight crew members15–31 repeatedly exposed to hypoxia on an irregular schedule for several months with each exposure lasting <24 hours (table 1). This type of hypoxic exposure is hereafter termed as ‘irregular short-term intermittent hypoxia’. Additionally, four prospective,32–35 four cross-sectional,36–39 two longitudinal40 41 and four observational studies42–45 were included (table 2). Eleven of these studies investigated repeated exposure of 4–14 days to hypoxia,32 36–45 while two studies investigated repeated hypoxic exposure lasting 3–4 weeks.33 34 These studies (table 2) are hereafter termed as ‘long-term intermittent hypoxia’.
Irregular short-term intermittent hypoxia
Long-term intermittent hypoxia
Irregular short-term intermittent hypoxia
A total of 15 studies were included in the evaluation of cardiovascular disease related mortality rates in flight personnel.15–26 29–31 In addition, two studies evaluated the standardised prevalence ratio (SPR) for cardiovascular diseases27 28 (table 1).
Of the 17 studies included, eight included males only, six analysed males and females separately and the remaining two studies pooled male and female participants in one analysis. The sample size ranged from 2327 to 93 771 participants, with an age span from 18 to ≥80 years. Professions included pilots, cockpit crew, cabin crew and flight engineers. The standardised mortality ratio (SMR) related to cardiovascular disease ranged from 0.18 to 1.40 in aircraft personnel (table 1), with 88 of 96 analyses demonstrating an SMR of less than 1. For analyses including males only, the cardiovascular disease related SMR ranged from 0.18 to 1.40, with 76 of 81 analyses reporting SMR below 1. Only two studies25 26 reported a SMR above 1.0. Specifically, male military pilots, navigators and mechanics aged 30–49 years are reported to have an SMR of 1.05–1.27, while the SMR of commercial pilots older than 80 years is 1.40.26 In addition, male cabin crew showed an SMR of 1.03.25
A gender-specific analysis of females demonstrates an SMR ranging from 0.16 to 1.28 (table 1), with two studies reporting a SMR of 1.28 and 1.17,15 23 and the remaining six studies (15 analyses) reporting a SMR between 0.16 and 0.81.15 20 23 25 26 31 Two studies reported the standard prevalence ratio (SPR) for cardiovascular diseases. One study reported an SPR less than 1 for, for example, coronary heart disease (0.53–0.73), hypertension (0.44–0.63) and high cholesterol (0.51–0.58) in 5366 persons.28 In contrast, an SPR of 1.39–3.51 for heart disease and 0.54–1.00 for hypertension has also been observed.27
Long-term intermittent hypoxia
A total of 14 studies were included in the analysis of the cardiovascular health of miners and soldiers32–45 (table 2). Participants’ age ranged from 18 to 65 years. The hypoxic exposure ranged from 3550 to 4600 m of altitude and lasted from 4 days to 14 days, except for two studies investigating 3–4 weeks’ exposure periods. Exposure was separated by a varying number of days at sea level, which most often corresponded to the exposure time (table 2). The investigated period ranged from 3 months to 22 years. Professions included were miners, soldiers, army officers and army draftees. Eleven studies included males only, while two studies included a small percentage of women as well (3%–12%).
The main variables evaluated were Hct, blood pressure, pulmonary blood pressure, Hb concentration and heart rate. Indications of increased cardiovascular problems were reported in 11 of the 13 retrieved studies, including elevated Hct, Hb concentration, erythropoietin concentration, plasma volume, blood pressure and heart rate.32 33 36–39 41–44 In addition, the prevalence of pulmonary hypertension appears increased after long-term intermittent hypoxia.33 35 38 39 43 Moreover, miners exhibit deteriorated lung function45 and increased pulmonary vascular resistance,33 as well as physical modifications in the anatomy of the heart that occur after long-term intermittent hypoxia exposure.32 39 In agreement with these factors, the prevalence of cardiovascular disease appears to be elevated in participants who are exposed to long-term intermittent hypoxia (see table 2). Indeed, 12 of 14 studies reported an elevated level of cardiac pathologies in the studied populations. In contrast, two studies report that 2.5 years of long-term intermittent hypoxia at 4500 m does not alter heart rate, or systolic and diastolic blood pressure40 and that 1 year of long-term intermittent hypoxia at 4000 m does not alter blood pressure in miners.45
Assessment of risk of bias
Figures 2 and 3 show the distribution of the risk of bias according to each category and domain specified in the Cochrane collaboration tool. Evaluation of the studies showed a low risk of bias in the following categories: blinding of outcome assessment (100%), disease evaluation (97%), evaluation period (97%), incomplete outcome data (85%), selective reporting (73%) and other bias (population demographic details, supplemental material, among others) (30%).

Risk of bias graph: authors’ assessments of each risk of bias item presented as percentages across all included studies.

{kind=link}
{kind=link}
{kind=link}
Risk of bias summary: authors' assessments of each risk of bias item for each included study.
The articles of Brito et al38 39 Hammer et al25 Linnersjö et al26 and Richalet et al32 were found to have the lowest risk of bias in the reporting of all items.
Discussion
The present systematic narrative review is the first to evaluate whether cardiovascular disease risk, quantified as an SMR, is increased with irregular short-term intermittent hypoxic exposure. Moreover, it is the first attempt to review the impact of long-term intermittent hypoxic exposure on cardiovascular-related risk of disease.
Irregular short-term intermittent hypoxia
In the present analysis, ‘irregular short-term intermittent hypoxic exposure’ was defined as repeated hypoxic exposure on an irregular schedule for several months, with each exposure lasting <24 hours. This definition is not universal but was developed to include as many studies as possible. Our literature search found that all the studies analysing potential health hazards of brief hypoxic exposures fit the definition. It was also evident that the best-studied population in this category is flight crew members. During a flight, cabin pressure is reduced to ~565 mm Hg, which corresponds to residing at ~2400 m above sea level. The physiological consequence is a reduction in PO2 to ~70 mm Hg, causing systemic hypoxia with an arterial saturation of ~90%.46 In general, systemic hypoxia is related to a variety of disease states, including heart failure, shock, pulmonary embolism and lung disease.47 However, our current systematic search demonstrates that irregular repeated exposure to hypoxia does not increase cardiovascular disease related SMR. Specifically, 88 out of 96 analyses demonstrated an SMR below 1 for both cockpit crew and cabin attendants. Pilots and flight crew members have to meet prescribed medical standards on recruitment and are required to pass periodic medical examinations,21 30 which may explain the low SMR. Additionally, the high socioeconomic status of pilots and flight crew members may contribute to the low SMR.25 26 Indeed, when comparing pilots with the highest income quintile of the general population, a significantly lower prevalence of obesity and smoking is apparent.21 Also, the low SMR of the cockpit crew and cabin attendants is evident for both genders (table 1). However, it must be noted that three studies report an SMR value higher than 1.15 23 26 In this context, it is important to note the wide CI observed, as a consequence of the low number of incidents (≤5). Specifically, military navigators and mechanics aged from 30 to 39 years showed one death from cardiovascular disease. However, 0.79 was expected, providing an SMR of 1.27, with a CI of 0.03 to 7.08.26
Finally, simulated intermittent hypoxic exposures may be an effective tool for managing and/or preventing cardiovascular diseases.48 Thus, in addition to the high socioeconomic status of pilots and flight crews, their exposure to intermittent hypoxia may contribute to the lower SMR by cardiovascular diseases. However, investigating the effect of a short-term intermittent hypoxic exposure on cardiovascular disease in patients is beyond the scope of the present review, and the reader is referred to existing reviews.48
In summary, cockpit crew members and cabin attendants exposed to irregular short-term intermittent hypoxia do not generally exhibit signs of increased mortality caused by cardiovascular disease. It appears that irregular short-term intermittent hypoxia either has no negative impact on cardiovascular health or at least that it does not cause negative effects large enough to compromise the generally good health of flight crews.
Long-term intermittent hypoxia
Hypoxic exposure for several days with different patterns of repetition was defined as ‘long-term intermittent hypoxic exposure’ in the present systematic review. This rather broad definition allowed the inclusion of studies primarily of miners and soldiers. Arterial saturation falls initially at higher altitudes. Due to the sigmoidal shape of the oxygen–haemoglobin dissociation curve, arterial saturation <92% becomes apparent from around pO2 below 75 mm Hg, which corresponds to ~2500 m. As a consequence, sympathetic activity, ventilatory response and pulmonary artery pressure increase.49 The acute impact of hypoxic exposure ranges from none or mild symptoms at ~2000 m to a lethal reduction of oxygen delivery in the unacclimatised individual at the highest altitudes, that is, above 8000 m or sometimes even less than this.50 In-between is the risk of development of pulmonary and cerebral oedema even at moderate altitude.51 If the stay at altitude is prolonged, such as a few days or weeks, physiological consequences include the risk of increased pulmonary artery pressure, pulmonary vascular remodelling, increased ventilation, and increases of erythrocyte and Hb concentration to maintain the delivery of oxygen at or above sea level values.49 However, the present term ‘long-term intermittent hypoxia’ is used to define the stage between the acute phase and the fully acclimatised condition, and the physiological adaptation to such exposure is less clear.
The present systematic search finds that miners and soldiers are the predominant populations exposed to long-term intermittent hypoxia, and they demonstrate clear potential hazardous phenotypes. Specifically, miners and army personnel may experience increased right ventricle wall thickness and left ventricular diastolic dysfunction,32 38 39 pulmonary hypertension33 35 38 39 and increased blood pressure,38 39 43 which is aggravated in participants with a record of hypertension.52 Also, Hb concentration is increased ~0.05 g/dL with years of long-term intermittent exposure.36 Excessive erythrocytosis is a risk factor for cardiovascular disease.53 Additionally, altered levels of nitric oxide synthase inhibitors, asymmetric dimethylarginine and monomethyl-L-arginine occur. All of these are associated with an increased risk of high-altitude pulmonary oedema.35 43 Only a few studies have included a low-altitude control group.32 37 40 41 44 It is evident from these investigations that the hypoxia groups had increased right ventricular dimension, elevated red cell volume and Hb concentration, as well as a decrease in forced expiratory volume.32 37 41
In the uncontrolled studies, changes were observed in erythropoietin,42 significant elevation of asymmetric dimethylarginine and L-monomethyl-L-arginine plasma concentrations35 43 and accelerated age-related lung function decline.34 Furthermore, some studies did not find an elevation in blood pressure.45 In contrast, the development of highly variable mild hypoxic pulmonary hypertension that resolves during a holiday period at lower altitude was reported.33
In summary, long-term intermittent hypoxia appears to increase the risk of conditions related to cardiovascular diseases, such as erythrocytosis, increased blood pressure and pulmonary blood pressure, as well as remodelling of the heart.
Strengths and limitations
The main strength of the current study is its novelty, given that no previous systematic review has analysed the risks of cardiovascular disease in workers who are subjected to intermittent hypoxia in either the irregular short term (flight crew) or the long term (miners/soldiers). A comprehensive search strategy was conducted in several medical databases (PubMed, Scopus and Web of sciences), and the search process was carried out independently by two authors, thereby minimising the likelihood of omitting eligible articles. However, different limitations must be considered in this study.
The main limitation was that the studies on miners/soldiers did not analyse the SMR. Therefore, we do not know whether the miners or soldiers affected by cardiovascular diseases died of this cause. The studies on miners/soldiers had smaller groups of participants who were observed for only a short period, making the results insufficient to show a possible acceleration in vascular ageing. Moreover, the studies on miners and flight crews were carried out in different countries, where lifestyle variations may interfere with the study target. For instance, miners are known to have a high rate of overweight and obesity, which is related to the development of cardiovascular disease,54 and mining is associated with adverse health effects independent of altitude.55 Both these factors may confound the results of long-term intermittent hypoxic exposure.
However, as far as we know, this is the first study that summarises the prevalence of certain type of cardiovascular disease in workers who have been subjected to intermittent hypoxia throughout a long period of their lives.
Conclusion
This systematic narrative review demonstrates that mortality from cardiovascular diseases in a population with irregular short-term intermittent hypoxia (2400 m) is not higher than average in a comparable population. However, individuals exposed to more severe long-term intermittent hypoxia (4200 m), such as miners and military personnel, appear to suffer an increased risk of cardiac disorders.
Acknowledgments
JA was funded by a Postdoctoral fellowship from the 'Fundación Alfonso Martín Escudero' (Spain). JP-D is part of the 'UGR Plan Propio de Investigación 2016' and the 'Excellence actions: Unit of Excellence on Exercise and Health (UCEES), University of Granada'.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors NN and JRH designed research (project conception, development of overall research plan and study oversight); JA, JB and JP-D conducted research (hands-on conduct of the experiments and data collection); NN and JRH provided essential reagents or provided essential materials; JP-D and JA analysed data or performed statistical analysis; JA, JB, JP-D and NN wrote the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no datasets generated and/or analysed for this study.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.